Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Muri As 2016Dokument7 SeitenMuri As 2016Vlady78Noch keine Bewertungen
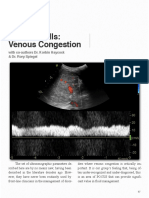
- Venous Congestion ChapterDokument8 SeitenVenous Congestion ChapterpcarrascoeNoch keine Bewertungen
- TOE Liver TransplantDokument10 SeitenTOE Liver TransplantpcarrascoeNoch keine Bewertungen
- Basic Perioperative Transesophageal Echocardiography Examination - A Consensus Statement of The American Society of Echocardiography and The Society of Cardiovascular AnesthesiologistsDokument14 SeitenBasic Perioperative Transesophageal Echocardiography Examination - A Consensus Statement of The American Society of Echocardiography and The Society of Cardiovascular AnesthesiologistsAdam ForshawNoch keine Bewertungen
- DSTC LDokument465 SeitenDSTC LRizki Irwansyah100% (2)
- Capnography and AnesthesiaDokument10 SeitenCapnography and AnesthesiapcarrascoeNoch keine Bewertungen
- Bezold JarishDokument11 SeitenBezold JarishpcarrascoeNoch keine Bewertungen
- Obese Patients PDFDokument10 SeitenObese Patients PDFpcarrascoeNoch keine Bewertungen
- Epidural Thoracic AnesthesiaDokument8 SeitenEpidural Thoracic AnesthesiapcarrascoeNoch keine Bewertungen
- 2014 - Addiction Science Uncovering Neurobiological ComplexityDokument15 Seiten2014 - Addiction Science Uncovering Neurobiological ComplexityBartolomé Pérez GálvezNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Family Psychoeducation & Care of The Schizophrenic ClientDokument70 SeitenFamily Psychoeducation & Care of The Schizophrenic ClientEcaroh Hew SmailliwNoch keine Bewertungen
- Epidemiology and Clinical Research Design, Part 1 - Study TypesDokument23 SeitenEpidemiology and Clinical Research Design, Part 1 - Study TypesShahiza Isa100% (1)
- EPOC Study Designs AboutDokument3 SeitenEPOC Study Designs AboutAleCsss123Noch keine Bewertungen
- Efficacy of Aromatherapy On Dental AnxietyDokument39 SeitenEfficacy of Aromatherapy On Dental AnxietyDafne MendozaNoch keine Bewertungen
- Virtual Simulation in Nursing Education A.9Dokument9 SeitenVirtual Simulation in Nursing Education A.9Abdishakur Mohamud HassanNoch keine Bewertungen
- Prevention Strategies To Reduce Future Impact of Low Back Pain: A Systematic Review and Meta-AnalysisDokument10 SeitenPrevention Strategies To Reduce Future Impact of Low Back Pain: A Systematic Review and Meta-AnalysisShivangi SaxenaNoch keine Bewertungen
- Ictus Ortesis MmiiDokument10 SeitenIctus Ortesis MmiiCeto Ust Puerto MonttNoch keine Bewertungen
- CH5 Exercises Solutions PDFDokument23 SeitenCH5 Exercises Solutions PDFhelloagainhelloNoch keine Bewertungen
- Global Covid Report PDFDokument73 SeitenGlobal Covid Report PDFmunirjssipgkperlisgm100% (3)
- WWC Soundpartners 092110Dokument9 SeitenWWC Soundpartners 092110api-256861915Noch keine Bewertungen
- Antenatal Care: Routine Care For The Healthy Pregnant WomanDokument304 SeitenAntenatal Care: Routine Care For The Healthy Pregnant WomanNadia Gina AnggrainiNoch keine Bewertungen
- 14.impact of Prognostic Discussions On The Patient-Physician Relationship Prospective Cohort StudyDokument7 Seiten14.impact of Prognostic Discussions On The Patient-Physician Relationship Prospective Cohort Studybunga mawarNoch keine Bewertungen
- Effect of A Thin Neck Pacifier On Primary Dentition RCTDokument10 SeitenEffect of A Thin Neck Pacifier On Primary Dentition RCTKiki PuchiNoch keine Bewertungen
- 6516516584123XDokument398 Seiten6516516584123Xmaya_fitrianaNoch keine Bewertungen
- Essential Messages - 2023 CMDokument14 SeitenEssential Messages - 2023 CMimran karimNoch keine Bewertungen
- Pediatric ResuscitationDokument55 SeitenPediatric ResuscitationMargaretDeniseDelRosarioNoch keine Bewertungen
- Chris Littlewood - Stephen May - Understanding Physiotherapy Research-Cambridge Scholars Publishing (2013)Dokument136 SeitenChris Littlewood - Stephen May - Understanding Physiotherapy Research-Cambridge Scholars Publishing (2013)Aya KhalilNoch keine Bewertungen
- Critical Appraisal 2017Dokument65 SeitenCritical Appraisal 2017Fransiscus RivaldyNoch keine Bewertungen
- EBPDokument32 SeitenEBPKlinikbersalin BpsadyamyshaNoch keine Bewertungen
- Risk Management in EndodonticsDokument39 SeitenRisk Management in EndodonticsDrSree KanthNoch keine Bewertungen
- 2012 Mirror Therapy For Improving Motor Function After StrokeDokument68 Seiten2012 Mirror Therapy For Improving Motor Function After StrokeMarcelo Ortiz Valenzuela100% (1)
- Conservative and Surgical Modalities in The Management of Pediatric Parapneumonic Effusion and EmpyemaDokument14 SeitenConservative and Surgical Modalities in The Management of Pediatric Parapneumonic Effusion and EmpyemaPamela JumpNoch keine Bewertungen
- Sensory Integration Therapy and Auditory Integration TrainingDokument10 SeitenSensory Integration Therapy and Auditory Integration TrainingMuskaan KhannaNoch keine Bewertungen
- 1 1 Apr 2006 PDFDokument30 Seiten1 1 Apr 2006 PDFnanistaciaNoch keine Bewertungen
- Aquatic Exercise in The Treatment of Low Back PainDokument13 SeitenAquatic Exercise in The Treatment of Low Back PainCíntia Spagnolo GomesNoch keine Bewertungen
- Full Text: Publication Info: Mental Health Weekly Digest Atlanta (Atlanta) 26 Feb 2018: 70Dokument2 SeitenFull Text: Publication Info: Mental Health Weekly Digest Atlanta (Atlanta) 26 Feb 2018: 70Ismalloh HanifNoch keine Bewertungen
- Bakker Vaneerde Designresearch InpressDokument57 SeitenBakker Vaneerde Designresearch InpressScent CemoNoch keine Bewertungen
- Chest.126.2.592 MBE EN UCIDokument9 SeitenChest.126.2.592 MBE EN UCIJaime RomeroNoch keine Bewertungen
- ASPEN NutritionDokument18 SeitenASPEN Nutritionsilvio da costa guerreiroNoch keine Bewertungen
- RCT+Appraisal+sheets. TherapyDokument2 SeitenRCT+Appraisal+sheets. Therapydian_c87Noch keine Bewertungen