Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Twilight PrincessDokument49 SeitenTwilight PrincessHikari DiegoNoch keine Bewertungen
- Introduction To LCCDokument32 SeitenIntroduction To LCCGonzalo LopezNoch keine Bewertungen
- Purpose in LifeDokument1 SeitePurpose in Lifeaashish95100% (1)
- AssessmentDokument9 SeitenAssessmentJuan Miguel Sapad AlpañoNoch keine Bewertungen
- 3 Tasks and ANS - Gamma Maths PDFDokument6 Seiten3 Tasks and ANS - Gamma Maths PDFNora ZhangNoch keine Bewertungen
- JKJKJDokument3 SeitenJKJKJjosecarlosvjNoch keine Bewertungen
- Sony Cdm82a 82b Cmt-hpx11d Hcd-hpx11d Mechanical OperationDokument12 SeitenSony Cdm82a 82b Cmt-hpx11d Hcd-hpx11d Mechanical OperationDanNoch keine Bewertungen
- Prestige Institute of Management & Research: Guided By:-Submitted By: - Prof. Arpit Loya Sumeet RattanDokument21 SeitenPrestige Institute of Management & Research: Guided By:-Submitted By: - Prof. Arpit Loya Sumeet RattanSumeet700005Noch keine Bewertungen
- Nasopharyngeal Angiofibroma - PPTX Essam SrourDokument10 SeitenNasopharyngeal Angiofibroma - PPTX Essam SrourSimina ÎntunericNoch keine Bewertungen
- Design and Development of Automatic Pneumatic Jack in Four Wheeler Ijariie5374Dokument5 SeitenDesign and Development of Automatic Pneumatic Jack in Four Wheeler Ijariie5374Saravanan ViswakarmaNoch keine Bewertungen
- G1CDokument12 SeitenG1CKhriz Ann C ÜNoch keine Bewertungen
- Percent by VolumeDokument19 SeitenPercent by VolumeSabrina LavegaNoch keine Bewertungen
- Emw 2007 FP 02093Dokument390 SeitenEmw 2007 FP 02093boj87Noch keine Bewertungen
- Market AnalysisDokument4 SeitenMarket AnalysisSaniya CharaniyaNoch keine Bewertungen
- Improve On-Time DeliveriesDokument24 SeitenImprove On-Time DeliveriesUdayNoch keine Bewertungen
- Case Studies of Transportation Public-Private Partnerships Around The WorldDokument158 SeitenCase Studies of Transportation Public-Private Partnerships Around The WorldzhenhuaruiNoch keine Bewertungen
- SDHI18 - Komparativna Analiza Primene Vodostana I Sinhronih Regulatora TurbinaDokument13 SeitenSDHI18 - Komparativna Analiza Primene Vodostana I Sinhronih Regulatora TurbinaAleksandar PetkovicNoch keine Bewertungen
- Innerwear Industry Pitch PresentationDokument19 SeitenInnerwear Industry Pitch PresentationRupeshKumarNoch keine Bewertungen
- Cecilia-Puff-Tee-Final-OUSM-Designs-12 MESES A TALLA 8Dokument19 SeitenCecilia-Puff-Tee-Final-OUSM-Designs-12 MESES A TALLA 8Jose SanchezNoch keine Bewertungen
- Managing Diabetic Foot Ulcers ReadingDokument21 SeitenManaging Diabetic Foot Ulcers Readinghimanshugupta811997Noch keine Bewertungen
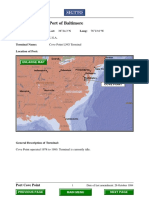
- Port Name: Port of BaltimoreDokument17 SeitenPort Name: Port of Baltimoremohd1khairul1anuarNoch keine Bewertungen
- Safe Lorry Loader Crane OperationsDokument4 SeitenSafe Lorry Loader Crane Operationsjdmultimodal sdn bhdNoch keine Bewertungen
- Math COT 3Dokument18 SeitenMath COT 3Icy Mae SenadosNoch keine Bewertungen
- Immigrant Italian Stone CarversDokument56 SeitenImmigrant Italian Stone Carversglis7100% (2)
- Inferring The Speaker's Tone, ModeDokument31 SeitenInferring The Speaker's Tone, Modeblessilda.delaramaNoch keine Bewertungen
- Basic Geriatric Nursing 6th Edition Williams Test BankDokument10 SeitenBasic Geriatric Nursing 6th Edition Williams Test Bankmaryrodriguezxsntrogkwd100% (49)
- CBSE DetailsDokument6 SeitenCBSE DetailsNARESH KUMARNoch keine Bewertungen
- Material Specification - 077154C-000-JSS-1700-009 - DDokument13 SeitenMaterial Specification - 077154C-000-JSS-1700-009 - DStructures ProductionNoch keine Bewertungen
- Module-4 (PDFDrive)Dokument67 SeitenModule-4 (PDFDrive)Divya priya KNoch keine Bewertungen
- 300 PSI CTS (MP-1115) Operation Manual Rev1.3Dokument18 Seiten300 PSI CTS (MP-1115) Operation Manual Rev1.3Juan Manuel VizosoNoch keine Bewertungen