Das könnte Ihnen auch gefallen
- BP Measurement BookletDokument13 SeitenBP Measurement BookletMohd KhateebNoch keine Bewertungen
- Ankle Brachial Index PDFDokument8 SeitenAnkle Brachial Index PDFIncredibleNoch keine Bewertungen
- Procedure: Ankle Brachial Index (ABI) in Adults Using A Handheld DopplerDokument8 SeitenProcedure: Ankle Brachial Index (ABI) in Adults Using A Handheld DopplerFachril ismailNoch keine Bewertungen
- Management of HypertensionDokument93 SeitenManagement of Hypertensionhasibsb28Noch keine Bewertungen
- Referat Ulkus DMDokument33 SeitenReferat Ulkus DMAisyah Fatinah AgamNoch keine Bewertungen
- WECOC - Diagnosing HypertensionDokument37 SeitenWECOC - Diagnosing HypertensionDhira 'Princess Kalonk' AninditaNoch keine Bewertungen
- Peripheral Vascular Disease Surgical PresentationDokument26 SeitenPeripheral Vascular Disease Surgical PresentationqreenNoch keine Bewertungen
- Chapter 07 Taking Vital SignsDokument22 SeitenChapter 07 Taking Vital SignsNephNoch keine Bewertungen
- Hypertension - Docx NCPDokument9 SeitenHypertension - Docx NCPMarjorie BelanteNoch keine Bewertungen
- Cardiovascular System (Diagnostic Procedure) : Prepared By: Kriegel Paman Bihasa RM, RN, UsrnDokument17 SeitenCardiovascular System (Diagnostic Procedure) : Prepared By: Kriegel Paman Bihasa RM, RN, UsrnKriegel Paman BihasaNoch keine Bewertungen
- Assessment and Diagnostic TestsDokument55 SeitenAssessment and Diagnostic TestsEmma IntiaNoch keine Bewertungen
- Understanding Ambulatory Blood Pressure Monitoring: by Abhishek Jha Jr2Dokument27 SeitenUnderstanding Ambulatory Blood Pressure Monitoring: by Abhishek Jha Jr2imranqazi11Noch keine Bewertungen
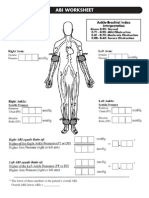
- Abi SheetsDokument2 SeitenAbi Sheetszaky soewandi0% (1)
- Cardiac Catheterization and MonitoringDokument40 SeitenCardiac Catheterization and MonitoringMarissa Asim100% (1)
- How To Measure Ankle Brachial IndexDokument4 SeitenHow To Measure Ankle Brachial Indexzaky0% (1)
- Ankle-Brachial Index For Assessment of Peripheral Arterial DiseaseDokument3 SeitenAnkle-Brachial Index For Assessment of Peripheral Arterial DiseaseKukuh Rizwido PrasetyoNoch keine Bewertungen
- A B C D e AssessmentDokument6 SeitenA B C D e AssessmentANGELICA JANE FLORENDONoch keine Bewertungen
- The Ankle-Brachial Pressure Index:: An Under-Used Tool in Primary Care?Dokument8 SeitenThe Ankle-Brachial Pressure Index:: An Under-Used Tool in Primary Care?andiniNoch keine Bewertungen
- Ankle-Brachial Index-3 PDFDokument9 SeitenAnkle-Brachial Index-3 PDFSarah HalanNoch keine Bewertungen
- Cardiac Stress TestingDokument24 SeitenCardiac Stress TestingRhoda Dela Torre ContrerasNoch keine Bewertungen
- Geron CardioDokument45 SeitenGeron CardioApril AlomiaNoch keine Bewertungen
- 9 - The Cardiovascular AssessmentDokument54 Seiten9 - The Cardiovascular Assessmente.mb275Noch keine Bewertungen
- Clinical Skills Handbook 2015 MEDN40060 2Dokument66 SeitenClinical Skills Handbook 2015 MEDN40060 2Wilson KhawNoch keine Bewertungen
- Hypovolemic Shock Nursing Care Management and Study GuideDokument1 SeiteHypovolemic Shock Nursing Care Management and Study GuideRoselyn VelascoNoch keine Bewertungen
- Hypertension Self ManagementDokument23 SeitenHypertension Self ManagementElizabeth HoNoch keine Bewertungen
- Peripheral Vascular DiseaseDokument3 SeitenPeripheral Vascular DiseaseJordiann A. BarnesNoch keine Bewertungen
- 3 NopalpamogasDokument5 Seiten3 NopalpamogasFeb NamiaNoch keine Bewertungen
- CC-Concept Map 2Dokument5 SeitenCC-Concept Map 2MDCITY50% (2)
- Ankle-Brachial Index For Assessment of Peripheral Arterial DiseaseDokument5 SeitenAnkle-Brachial Index For Assessment of Peripheral Arterial DiseaseindrawepeNoch keine Bewertungen
- Diabetic Ketoacidosis DKA Acute Management ABCDEDokument10 SeitenDiabetic Ketoacidosis DKA Acute Management ABCDESSNoch keine Bewertungen
- Care For Dialysis PatientsDokument18 SeitenCare For Dialysis PatientsHemanth PrakashNoch keine Bewertungen
- Effects of Aging On The HeartDokument56 SeitenEffects of Aging On The HeartJustin Ahorro-DionisioNoch keine Bewertungen
- Cardiogenic ShockDokument3 SeitenCardiogenic Shockmerin sunilNoch keine Bewertungen
- Hypertension Syakib Bakri - BPJS 2015 FINALDokument116 SeitenHypertension Syakib Bakri - BPJS 2015 FINALPeriyent Liveryent VozzervodNoch keine Bewertungen
- PBL 2 Session 2 PresentationDokument44 SeitenPBL 2 Session 2 PresentationElisaNoch keine Bewertungen
- Endocrinology and Diabetes Department RSUP DR M Djamil Padang 2018Dokument13 SeitenEndocrinology and Diabetes Department RSUP DR M Djamil Padang 2018Septiandry Ade PutraNoch keine Bewertungen
- Arthvhjvjherial Bgtfutvcivbjknllood Flojbjkbkjbw Vhjvof The Lehbvkhbkgs-DamaskDokument3 SeitenArthvhjvjherial Bgtfutvcivbjknllood Flojbjkbkjbw Vhjvof The Lehbvkhbkgs-DamaskNicoh AvilaNoch keine Bewertungen
- Nursing DiagnosisDokument5 SeitenNursing DiagnosisGeovanni Rai HermanoNoch keine Bewertungen
- Activtiy UntitledDokument6 SeitenActivtiy UntitledJan Cyrel ColomaNoch keine Bewertungen
- Pre-Op Assessment: Dr. Ayesha Ehsan House Surgeon S-IIDokument25 SeitenPre-Op Assessment: Dr. Ayesha Ehsan House Surgeon S-IIFatima MNoch keine Bewertungen
- NICE 2011 SlidesetDokument25 SeitenNICE 2011 SlidesetMocanu Cristina-VioricaNoch keine Bewertungen
- Anesthesia For Cesarean SectionDokument70 SeitenAnesthesia For Cesarean SectionElsya ParamitasariNoch keine Bewertungen
- Diabetic Foot Dr. Sobia FinDokument139 SeitenDiabetic Foot Dr. Sobia FinvizzieNoch keine Bewertungen
- Cardiology NotesDokument13 SeitenCardiology NotesFreeNursingNotes78% (9)
- Peripheral Vascular Disease: Aditya Adella Pratama G1A220012 Dr. Amran Sinaga, Sp. BDokument22 SeitenPeripheral Vascular Disease: Aditya Adella Pratama G1A220012 Dr. Amran Sinaga, Sp. BTriyanihzamNoch keine Bewertungen
- 5 Upper Extremity Arterial Duplex Evaluation Updated 2018 PDFDokument8 Seiten5 Upper Extremity Arterial Duplex Evaluation Updated 2018 PDFHasan Mohammad NayeemNoch keine Bewertungen
- 4B MS Midterm NotespdfDokument23 Seiten4B MS Midterm NotespdfNorbelisa Tabo-ac CadungganNoch keine Bewertungen
- Cardiovascular System: AnatomyDokument19 SeitenCardiovascular System: AnatomyStephanie MacVeighNoch keine Bewertungen
- Pediatric Cardiology: Betsy Johnson, MSN, CPNP-PC Aya Rahav, MS, RN, CPNDokument90 SeitenPediatric Cardiology: Betsy Johnson, MSN, CPNP-PC Aya Rahav, MS, RN, CPNGelsey Gelsinator JianNoch keine Bewertungen
- Criteri Dimissione ICUDokument4 SeitenCriteri Dimissione ICUgianriciNoch keine Bewertungen
- Pe Abh What Is Peripheral Vascular Disease Ucm 300323Dokument2 SeitenPe Abh What Is Peripheral Vascular Disease Ucm 300323Mahmoud ElsabbaghNoch keine Bewertungen
- Cardiac ComplicationDokument12 SeitenCardiac ComplicationResa ShotsNoch keine Bewertungen
- Ambulatory Blood Pressure MonitoringDokument5 SeitenAmbulatory Blood Pressure Monitoringابو عبد الرحمنNoch keine Bewertungen
- Kuliah Thrombosis 2015 NNDokument39 SeitenKuliah Thrombosis 2015 NNBeladiena Citra SiregarNoch keine Bewertungen
- Pathophysiology of Congestive Heart Failure: Reported By: Jay - Ann M. Cabia BSN II-ADokument21 SeitenPathophysiology of Congestive Heart Failure: Reported By: Jay - Ann M. Cabia BSN II-Ajoyrena ochondraNoch keine Bewertungen
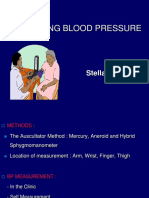
- Measuring Blood Pressure: Stella PalarDokument30 SeitenMeasuring Blood Pressure: Stella Palarastrid abrahamsNoch keine Bewertungen
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingVon EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNoch keine Bewertungen
- Abi SheetsDokument2 SeitenAbi Sheetszaky soewandi0% (1)
- A Quasi-Experimental Study To Assess The Impact of Four Adolescent Sexual Health Interventions in Sub-Saharan AfricaDokument10 SeitenA Quasi-Experimental Study To Assess The Impact of Four Adolescent Sexual Health Interventions in Sub-Saharan Africazaky soewandiNoch keine Bewertungen
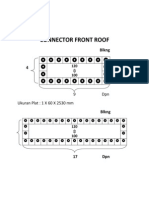
- Connector Front RoofDokument2 SeitenConnector Front Roofzaky soewandiNoch keine Bewertungen
- CranioplastyDokument2 SeitenCranioplastyzaky soewandiNoch keine Bewertungen