Das könnte Ihnen auch gefallen
- Your Social Security Rights in UK - enDokument29 SeitenYour Social Security Rights in UK - enSara Loureiro da LuzNoch keine Bewertungen
- Dwell Prefab Sourcebook Summer 2013Dokument172 SeitenDwell Prefab Sourcebook Summer 2013Sara Loureiro da Luz100% (4)
- Members GuideDokument53 SeitenMembers GuideSara Loureiro da LuzNoch keine Bewertungen
- General Dental Performers List ApplicationDokument24 SeitenGeneral Dental Performers List ApplicationSara Loureiro da LuzNoch keine Bewertungen
- List of EEA Competent AuthoritiesDokument6 SeitenList of EEA Competent AuthoritiesSara Loureiro da LuzNoch keine Bewertungen
- Indemnity Application For Dental Membership of The Medical Protection SocietyDokument12 SeitenIndemnity Application For Dental Membership of The Medical Protection SocietySara Loureiro da LuzNoch keine Bewertungen
- Bio Degrade Dental AmalgamDokument10 SeitenBio Degrade Dental AmalgamJaswanth ReddyNoch keine Bewertungen
- Dental X-Ray ExamsDokument2 SeitenDental X-Ray ExamsSara Loureiro da LuzNoch keine Bewertungen
- Evidence of Basic Formal Qualifications For Dentists From The EEADokument6 SeitenEvidence of Basic Formal Qualifications For Dentists From The EEASara Loureiro da LuzNoch keine Bewertungen
- Periodontal Disease AdaDokument6 SeitenPeriodontal Disease AdaSara Loureiro da LuzNoch keine Bewertungen
- Endo AdaDokument2 SeitenEndo AdaSara Loureiro da LuzNoch keine Bewertungen
- Patient ConsentDokument8 SeitenPatient ConsentSara Loureiro da LuzNoch keine Bewertungen
- Your Guide To Treatment Options For The Diseased ToothDokument6 SeitenYour Guide To Treatment Options For The Diseased ToothSara Loureiro da LuzNoch keine Bewertungen
- Your Smile - An Owner's ManualDokument11 SeitenYour Smile - An Owner's ManualSara Loureiro da LuzNoch keine Bewertungen
- London Rail Tube MapDokument1 SeiteLondon Rail Tube MapSara Loureiro da LuzNoch keine Bewertungen
- Bioactive Glass-Published ArticleDokument4 SeitenBioactive Glass-Published ArticleSara Loureiro da LuzNoch keine Bewertungen
- A Guide For International Post UsersDokument16 SeitenA Guide For International Post UsersSara Loureiro da LuzNoch keine Bewertungen
- Dental - NHS and Private Application Form To Register - 2013-10-EDokument15 SeitenDental - NHS and Private Application Form To Register - 2013-10-ESara Loureiro da LuzNoch keine Bewertungen
- ExciTE F - ExciTE F DSCDokument6 SeitenExciTE F - ExciTE F DSCSara Loureiro da LuzNoch keine Bewertungen
- Zinc Oxide Eugenol2012Dokument18 SeitenZinc Oxide Eugenol2012Sara Loureiro da LuzNoch keine Bewertungen
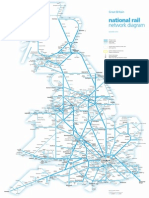
- National Rail Network Diagram: Great BritainDokument1 SeiteNational Rail Network Diagram: Great BritainSara Loureiro da LuzNoch keine Bewertungen
- Maintaining StandardsDokument90 SeitenMaintaining StandardsSara Loureiro da LuzNoch keine Bewertungen
- National Rail Operators MapDokument1 SeiteNational Rail Operators MapSara Loureiro da LuzNoch keine Bewertungen
- 752861Dokument7 Seiten752861Natalia Lépez HermosillaNoch keine Bewertungen
- Remote PrescribingDokument1 SeiteRemote PrescribingSara Loureiro da LuzNoch keine Bewertungen
- Complaints HandlingDokument12 SeitenComplaints HandlingSara Loureiro da LuzNoch keine Bewertungen
- A Diagnostic Comparison of Observer Performance in Panoramic and Periapical Radiographs For Some Common Dental PathosesDokument5 SeitenA Diagnostic Comparison of Observer Performance in Panoramic and Periapical Radiographs For Some Common Dental PathosesSara Loureiro da LuzNoch keine Bewertungen
- EP7 Final Programme WebDokument99 SeitenEP7 Final Programme WebSara Loureiro da LuzNoch keine Bewertungen
- Cold Testing Through Full-Coverage RestorationsDokument6 SeitenCold Testing Through Full-Coverage RestorationsSara Loureiro da LuzNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Feasibility Study For A Sustainability Based Clothing Start-UpDokument49 SeitenFeasibility Study For A Sustainability Based Clothing Start-UpUtso DasNoch keine Bewertungen
- Court Documents From Toronto Police Project Brazen - Investigation of Alexander "Sandro" Lisi and Toronto Mayor Rob FordDokument474 SeitenCourt Documents From Toronto Police Project Brazen - Investigation of Alexander "Sandro" Lisi and Toronto Mayor Rob Fordanna_mehler_papernyNoch keine Bewertungen
- Quanser Active Mass Damper UserManual PDFDokument21 SeitenQuanser Active Mass Damper UserManual PDFCHAVEZ MURGA ARTURO ALEJANDRONoch keine Bewertungen
- SAi Sankata Nivarana StotraDokument3 SeitenSAi Sankata Nivarana Stotrageetai897Noch keine Bewertungen
- Easy Pork Schnitzel: With Apple Parmesan Salad & Smokey AioliDokument2 SeitenEasy Pork Schnitzel: With Apple Parmesan Salad & Smokey Aioliclarkpd6Noch keine Bewertungen
- Cyber Ethics IssuesDokument8 SeitenCyber Ethics IssuesThanmiso LongzaNoch keine Bewertungen
- High-Performance Cutting and Grinding Technology For CFRP (Carbon Fiber Reinforced Plastic)Dokument7 SeitenHigh-Performance Cutting and Grinding Technology For CFRP (Carbon Fiber Reinforced Plastic)Dongxi LvNoch keine Bewertungen
- Chapter 2 Demand (ECO415)Dokument28 SeitenChapter 2 Demand (ECO415)hurin inaniNoch keine Bewertungen
- Building Envelop Design GuidDokument195 SeitenBuilding Envelop Design GuidCarlos Iriondo100% (1)
- Promises From The BibleDokument16 SeitenPromises From The BiblePaul Barksdale100% (1)
- 47 Vocabulary Worksheets, Answers at End - Higher GradesDokument51 Seiten47 Vocabulary Worksheets, Answers at End - Higher GradesAya Osman 7KNoch keine Bewertungen
- 09 - Arithmetic Progressions - 16 PDFDokument16 Seiten09 - Arithmetic Progressions - 16 PDFShah RukhNoch keine Bewertungen
- Workbook Answers: AS/A-level English Literature WorkbookDokument42 SeitenWorkbook Answers: AS/A-level English Literature WorkbooktelmarventuraNoch keine Bewertungen
- Comparative Study of The Prison System in India, UK and USADokument12 SeitenComparative Study of The Prison System in India, UK and USAHarneet Kaur100% (1)
- JLPT N2 Vocab - 04Dokument345 SeitenJLPT N2 Vocab - 04raj_kumartNoch keine Bewertungen
- Systems Analysis and Design 11th Edition Tilley Test BankDokument15 SeitenSystems Analysis and Design 11th Edition Tilley Test Banksusanschroederoqdrkxtafn100% (15)
- Test For Determining Agency - Analysis Using Case LawsDokument7 SeitenTest For Determining Agency - Analysis Using Case Lawsanitta joseNoch keine Bewertungen
- Hotel BookingDokument1 SeiteHotel BookingJagjeet SinghNoch keine Bewertungen
- Research Article: Old Sagay, Sagay City, Negros Old Sagay, Sagay City, Negros Occidental, PhilippinesDokument31 SeitenResearch Article: Old Sagay, Sagay City, Negros Old Sagay, Sagay City, Negros Occidental, PhilippinesLuhenNoch keine Bewertungen
- Chapter 13 Creating and Managing TeamsDokument40 SeitenChapter 13 Creating and Managing TeamsH.Noch keine Bewertungen
- Romeuf Et Al., 1995Dokument18 SeitenRomeuf Et Al., 1995David Montaño CoronelNoch keine Bewertungen
- Financial Accounting Theory Craig Deegan Chapter 7Dokument9 SeitenFinancial Accounting Theory Craig Deegan Chapter 7Sylvia Al-a'maNoch keine Bewertungen
- Campos V BPI (Civil Procedure)Dokument2 SeitenCampos V BPI (Civil Procedure)AngeliNoch keine Bewertungen
- SBMPTN 2016 Kode 333Dokument6 SeitenSBMPTN 2016 Kode 333Allisa MasithaNoch keine Bewertungen
- DeathoftheegoDokument123 SeitenDeathoftheegoVictor LadefogedNoch keine Bewertungen
- Mudbound: Virgil Williams and Dee ReesDokument125 SeitenMudbound: Virgil Williams and Dee Reesmohan kumarNoch keine Bewertungen
- Net Present Value AnalysisDokument6 SeitenNet Present Value AnalysisAmna Khalid100% (1)
- CHANDRA RAHU Yuti (Moon Rahu Conjunction)Dokument3 SeitenCHANDRA RAHU Yuti (Moon Rahu Conjunction)Shailendra Shrivastava0% (1)
- Co-Publisher AgreementDokument1 SeiteCo-Publisher AgreementMarcinNoch keine Bewertungen
- Chapter 8 Supplier Quality ManagementDokument71 SeitenChapter 8 Supplier Quality ManagementAnh NguyenNoch keine Bewertungen