Das könnte Ihnen auch gefallen
- AVBS2001Dokument81 SeitenAVBS2001Celine Berjot100% (1)
- Lecture 3 - ProtistaDokument41 SeitenLecture 3 - ProtistaLee KaiYangNoch keine Bewertungen
- Acute Otitis Media: Jama Patient PageDokument1 SeiteAcute Otitis Media: Jama Patient PageS. JohnNoch keine Bewertungen
- Questionnaire (MP)Dokument15 SeitenQuestionnaire (MP)Angelo MercedeNoch keine Bewertungen
- Handbook of Immunological Investigations in Children: Handbooks of Investigation in ChildrenVon EverandHandbook of Immunological Investigations in Children: Handbooks of Investigation in ChildrenNoch keine Bewertungen
- Measles BasicsDokument39 SeitenMeasles Basicstummalapalli venkateswara raoNoch keine Bewertungen
- History of ImmunologyDokument6 SeitenHistory of ImmunologyKitt KittNoch keine Bewertungen
- History Anesthesia 2003-2007Dokument9 SeitenHistory Anesthesia 2003-2007John RaufNoch keine Bewertungen
- Measles: 1. Disease ReportingDokument18 SeitenMeasles: 1. Disease ReportingMemo AliNoch keine Bewertungen
- Microbiology's 50 Most Significant Events 1875-PresentDokument47 SeitenMicrobiology's 50 Most Significant Events 1875-PresentMeidinaInasa100% (1)
- Introduction To The Immune System: Department of Biotechnology Ramaiah University of Applied Sciences BangaloreDokument86 SeitenIntroduction To The Immune System: Department of Biotechnology Ramaiah University of Applied Sciences Bangaloreprathyoosha baskaran100% (1)
- History of VirologyDokument25 SeitenHistory of VirologySANDEEPANM100% (1)
- Historical Development of Medical MicrobiologyDokument84 SeitenHistorical Development of Medical MicrobiologyH.K. DL67% (3)
- History of ImmunologyDokument4 SeitenHistory of Immunologyaurax143100% (1)
- Frontiers in Clinical Drug Research - Hematology: Volume 3Von EverandFrontiers in Clinical Drug Research - Hematology: Volume 3Noch keine Bewertungen
- The History of TuberculosisDokument9 SeitenThe History of Tuberculosispimpaliukas1100% (1)
- Leslie J. Reagan, Nancy Tomes, Paula A. Treichler-Medicine's Moving Pictures - Medicine, Health, and Bodies in American Film and Television (Rochester Studies in Medical History) (2007)Dokument356 SeitenLeslie J. Reagan, Nancy Tomes, Paula A. Treichler-Medicine's Moving Pictures - Medicine, Health, and Bodies in American Film and Television (Rochester Studies in Medical History) (2007)Sergio Peralta100% (1)
- Cell Mediated Immunity LectDokument22 SeitenCell Mediated Immunity LectNova PamastaNoch keine Bewertungen
- Asphyxia KSDokument109 SeitenAsphyxia KSBnB Usmle100% (1)
- Genetic Disorders: Ma. Minda Luz M. Manuguid, M.DDokument65 SeitenGenetic Disorders: Ma. Minda Luz M. Manuguid, M.Djulo_05100% (1)
- Chromosomal AbnormalitiesDokument3 SeitenChromosomal AbnormalitiesYra Mie DitaroNoch keine Bewertungen
- Booklist For MedDokument16 SeitenBooklist For Medngc1100% (1)
- Depanshu Belwal Power PointDokument12 SeitenDepanshu Belwal Power PointvickyvermaNoch keine Bewertungen
- What Is Pompe Disease and What Are The Causes of Pompe Disease?Dokument4 SeitenWhat Is Pompe Disease and What Are The Causes of Pompe Disease?Gamze Hatlar100% (1)
- History of Microbiology 16th CENTURYDokument3 SeitenHistory of Microbiology 16th CENTURYMeangel QuillaoNoch keine Bewertungen
- Measles PDFDokument3 SeitenMeasles PDFdrpranandhaNoch keine Bewertungen
- General Medical MicrobiologyDokument20 SeitenGeneral Medical MicrobiologySadiya RhasyaNoch keine Bewertungen
- Krok 1anatomy2Dokument1 SeiteKrok 1anatomy2Sandeep KumarNoch keine Bewertungen
- BacteriaDokument21 SeitenBacteriatapas kunduNoch keine Bewertungen
- 5 ImmunoglobulinsDokument39 Seiten5 ImmunoglobulinsAlexandra SpiridonNoch keine Bewertungen
- History of ImmunologyDokument6 SeitenHistory of ImmunologyCatherine MerillenoNoch keine Bewertungen
- Authentic Assessment (Genetics)Dokument2 SeitenAuthentic Assessment (Genetics)Raquel Lizardo100% (2)
- RemoraDokument5 SeitenRemoraVicente Anislado TolentinoNoch keine Bewertungen
- Evolution: Evidence in Fossil RecordsDokument10 SeitenEvolution: Evidence in Fossil RecordsAlexa Cuevas100% (1)
- The Pyridine Nucleotide CoenzymesVon EverandThe Pyridine Nucleotide CoenzymesJohannes EverseNoch keine Bewertungen
- Best Physiology TextbookDokument3 SeitenBest Physiology TextbookPeterNoch keine Bewertungen
- Minireview: Intestinal Pathophysiology in AutismDokument11 SeitenMinireview: Intestinal Pathophysiology in Autism__aguNoch keine Bewertungen
- M4 Lecture 7 Infectious DiseaseDokument20 SeitenM4 Lecture 7 Infectious DiseaseChing CHANNoch keine Bewertungen
- Nature of DiseaseDokument14 SeitenNature of DiseaseLambo Ignacio Queen Quin100% (1)
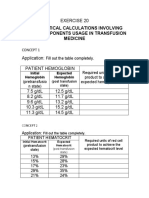
- Mathematical Calculations Involving Blood Components Usage in Transfusion MedicineDokument8 SeitenMathematical Calculations Involving Blood Components Usage in Transfusion MedicineNatalie CuNoch keine Bewertungen
- Selected Topics in the History of Biochemistry. Personal Recollections. Part IIIVon EverandSelected Topics in the History of Biochemistry. Personal Recollections. Part IIIBewertung: 1 von 5 Sternen1/5 (1)
- Anaerobic Infections in HumansVon EverandAnaerobic Infections in HumansSydney FinegoldBewertung: 5 von 5 Sternen5/5 (1)
- Eucaryotic Gene RegulationVon EverandEucaryotic Gene RegulationRichard AxelNoch keine Bewertungen
- Introduction To ImmunologyDokument41 SeitenIntroduction To ImmunologymicrokannanNoch keine Bewertungen
- Part A:: History of DNADokument4 SeitenPart A:: History of DNAmercy mukisaNoch keine Bewertungen
- A Coloring Book From Our CollectionsDokument9 SeitenA Coloring Book From Our CollectionsMaríaLujánNoch keine Bewertungen
- The Origins of The History and Physical ExaminationDokument21 SeitenThe Origins of The History and Physical ExaminationNEuRoLoGisT CoFFeeCuPNoch keine Bewertungen
- Modeling The Cell Cycle and MitosisDokument4 SeitenModeling The Cell Cycle and MitosisFroilan Mae Olado CahaponNoch keine Bewertungen
- The Edaphic Factors and The Soil Inhabitants: Exercise No.. 2Dokument7 SeitenThe Edaphic Factors and The Soil Inhabitants: Exercise No.. 2Sakib R SiddiqueNoch keine Bewertungen
- Karyotype Lab: Objective: Students Will Interpret Karyotypes To Determine The Gender of Individuals and Whether TheyDokument7 SeitenKaryotype Lab: Objective: Students Will Interpret Karyotypes To Determine The Gender of Individuals and Whether Theyjeannine limoli100% (1)
- Examn of Molecular BiologyDokument11 SeitenExamn of Molecular BiologycegfracNoch keine Bewertungen
- VNS Faculty of Pharmacy: Mentors - Presented byDokument1 SeiteVNS Faculty of Pharmacy: Mentors - Presented bypoplu100% (1)
- Lsm3212 CA3 EssayDokument3 SeitenLsm3212 CA3 EssayAbraham KangNoch keine Bewertungen
- Gastrointestinal DiseasesDokument853 SeitenGastrointestinal DiseasesCiobanasu Denisa100% (1)
- Micro Zoubi PDFDokument73 SeitenMicro Zoubi PDFVims BatchNoch keine Bewertungen
- Kimberly F. v. Mary Hitchcock, 1st Cir. (1993)Dokument34 SeitenKimberly F. v. Mary Hitchcock, 1st Cir. (1993)Scribd Government DocsNoch keine Bewertungen
- Virus Family Envelope Stuff To Know Treatment/ VaccineDokument10 SeitenVirus Family Envelope Stuff To Know Treatment/ Vaccinebtoy1Noch keine Bewertungen
- Urgent: Invented by William H. Gates (Aka Bill Gates) and Others, Listing Energy HarvestingDokument3 SeitenUrgent: Invented by William H. Gates (Aka Bill Gates) and Others, Listing Energy HarvestingShayna A PitreNoch keine Bewertungen
- DAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcDokument12 SeitenDAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcMahezha DhewaNoch keine Bewertungen
- West Nile FeverDokument23 SeitenWest Nile Fevertummalapalli venkateswara raoNoch keine Bewertungen
- Comprehensive Review FundaDokument47 SeitenComprehensive Review FundaNoey TabangcuraNoch keine Bewertungen
- 01 - Adult Vaccination Recommendation and How To Build Immunization Clinic - Prof Samsuridjal Djauzi PDFDokument44 Seiten01 - Adult Vaccination Recommendation and How To Build Immunization Clinic - Prof Samsuridjal Djauzi PDFfaizahafnitaNoch keine Bewertungen
- ASOT Serum TestDokument4 SeitenASOT Serum TestPrincess SaniaNoch keine Bewertungen
- Natural History of Cervical NeoplasiaDokument32 SeitenNatural History of Cervical NeoplasianellieauthorNoch keine Bewertungen
- Mims Abbreviation IndexDokument1 SeiteMims Abbreviation IndexHendry RamadhanNoch keine Bewertungen
- Flu Religious ExemptionDokument3 SeitenFlu Religious ExemptionFRANCHESCA DEL MUNDONoch keine Bewertungen
- SeizuresDokument3 SeitenSeizuresMarie PetalcorinNoch keine Bewertungen
- December 14, 2018 Strathmore TimesDokument20 SeitenDecember 14, 2018 Strathmore TimesStrathmore TimesNoch keine Bewertungen
- Jurnal Demam TifoidDokument6 SeitenJurnal Demam TifoidCysta NarisaNoch keine Bewertungen
- RabiesDokument2 SeitenRabiesninzah wanzahNoch keine Bewertungen
- Nexus Magazine - Vol 21 #4, June-July 2014 - Nexus VariousDokument114 SeitenNexus Magazine - Vol 21 #4, June-July 2014 - Nexus VariousKLANIARIS100% (1)
- CFLGA Field Testing - Handbook PDFDokument63 SeitenCFLGA Field Testing - Handbook PDFAbe Anshari100% (1)
- Management of Hemophilia: Dr. Zoona Qazi Post Graduate ResidentDokument33 SeitenManagement of Hemophilia: Dr. Zoona Qazi Post Graduate ResidentZuna QaziNoch keine Bewertungen
- Monoclonal AntibodiesDokument240 SeitenMonoclonal AntibodiesArepalli SanthoshNoch keine Bewertungen
- Virus: Measuring The Size of VirusesDokument18 SeitenVirus: Measuring The Size of VirusesVargheseNoch keine Bewertungen
- English Las1 q3Dokument9 SeitenEnglish Las1 q3Allysa Rotubio EmbudoNoch keine Bewertungen
- Waaw Posters PDFDokument4 SeitenWaaw Posters PDFRitna HaniNoch keine Bewertungen
- Clinical Laboratory Immunology 1st Edition Maahon Tice Test BankDokument8 SeitenClinical Laboratory Immunology 1st Edition Maahon Tice Test BankBrian Craig100% (37)
- (Edited) N31-G6-SOP-and-Conceptual-FrameworkDokument5 Seiten(Edited) N31-G6-SOP-and-Conceptual-Frameworkst michael machine shopNoch keine Bewertungen
- Salt Lake County Weekly Flu ReportDokument5 SeitenSalt Lake County Weekly Flu ReportAdam ForgieNoch keine Bewertungen
- Body Defense MechanismsDokument4 SeitenBody Defense MechanismsDessrae CabanlitNoch keine Bewertungen
- FORUMDokument4 SeitenFORUMGan Jia JingNoch keine Bewertungen
- Pneumonia in Immunocompromised Patients: Respirology (2009) 14 (Suppl. 2) S44 - S50Dokument7 SeitenPneumonia in Immunocompromised Patients: Respirology (2009) 14 (Suppl. 2) S44 - S50intankmlsNoch keine Bewertungen
- GY339 Environmental Classification of Excreta Related Disease 2017Dokument58 SeitenGY339 Environmental Classification of Excreta Related Disease 2017Lorraine100% (1)
- Demon in The Freezer Final QuestionsDokument3 SeitenDemon in The Freezer Final QuestionseddfungusNoch keine Bewertungen
- Q & A Info Sheet PDFDokument3 SeitenQ & A Info Sheet PDFJopit Olavario RiveraNoch keine Bewertungen