Das könnte Ihnen auch gefallen
- Uterine FibroidDokument46 SeitenUterine FibroidAfiqi FikriNoch keine Bewertungen
- The Management of Uterine Leiomyomas: DR .Ashraf FoudaDokument158 SeitenThe Management of Uterine Leiomyomas: DR .Ashraf Foudakhadzx100% (2)
- The Management of Uterine Leiomyomas: Egypt - Damietta General HospitalDokument158 SeitenThe Management of Uterine Leiomyomas: Egypt - Damietta General HospitalKhaye MendozaNoch keine Bewertungen
- Uterine FibroidsDokument21 SeitenUterine FibroidsPrasun BiswasNoch keine Bewertungen
- Surgical Approach To Hysterectomy For Benign Gynaecological DiseaseDokument19 SeitenSurgical Approach To Hysterectomy For Benign Gynaecological DiseasebambangtrionocNoch keine Bewertungen
- The Management of Uterine Leiomyomas: Egypt - Damietta General HospitalDokument158 SeitenThe Management of Uterine Leiomyomas: Egypt - Damietta General HospitalAdhy HermawanNoch keine Bewertungen
- Management of Ovarian EndometriomaDokument13 SeitenManagement of Ovarian EndometriomaAghnia PutriNoch keine Bewertungen
- OB-GYN 101: Uterine LeiomyomaDokument3 SeitenOB-GYN 101: Uterine Leiomyomamadmax500Noch keine Bewertungen
- Diagnosis, Evaluation, and Treatment of AdenomyosisDokument3 SeitenDiagnosis, Evaluation, and Treatment of AdenomyosisAndres MahechaNoch keine Bewertungen
- Fibroids: DR F HoveDokument18 SeitenFibroids: DR F HoveKelvin MaikanaNoch keine Bewertungen
- 4083 15383 1 PBDokument5 Seiten4083 15383 1 PBAljoieRoseNoch keine Bewertungen
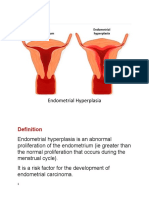
- Abnormalities of The EndometriumDokument3 SeitenAbnormalities of The EndometriumDymas R SyahputraNoch keine Bewertungen
- Kista Ovarium 21906150Dokument43 SeitenKista Ovarium 21906150NUR ATHIFAHNoch keine Bewertungen
- Uterine FibroidsDokument47 SeitenUterine FibroidsMoh Aldhy HusaintNoch keine Bewertungen
- MenorrhagiaDokument3 SeitenMenorrhagiajermie22100% (1)
- Myomectomy & Adenomyosis ResectionDokument31 SeitenMyomectomy & Adenomyosis ResectionagathapradanaNoch keine Bewertungen
- The Role of Hysteroscopic and Robot-Assisted Laparoscopic Myomectomy in The Setting of InfertilityDokument13 SeitenThe Role of Hysteroscopic and Robot-Assisted Laparoscopic Myomectomy in The Setting of InfertilityMarco Julcamoro AsencioNoch keine Bewertungen
- Ijrcog-13356 oDokument5 SeitenIjrcog-13356 on2763288Noch keine Bewertungen
- Myoma UteriDokument21 SeitenMyoma UteriLangitBiruNoch keine Bewertungen
- PDF Consentimiento InformadoDokument24 SeitenPDF Consentimiento InformadoSara Elena Rodriguez RodriguezNoch keine Bewertungen
- MacyDokument5 SeitenMacyMacy CalibodNoch keine Bewertungen
- Uterine MyomaDokument45 SeitenUterine MyomaAndiniMayudhaNoch keine Bewertungen
- Fibroids by EasterDokument7 SeitenFibroids by EasterIGA ABRAHAMNoch keine Bewertungen
- Myoma Uteri/Fibroids/ Leiomyomata: Symptoms of Uterine Myoma May IncludeDokument3 SeitenMyoma Uteri/Fibroids/ Leiomyomata: Symptoms of Uterine Myoma May IncludeDiane MargretNoch keine Bewertungen
- By, DR - Viknesvaran AnbalaganDokument28 SeitenBy, DR - Viknesvaran AnbalaganViknesvaran AnbalaganNoch keine Bewertungen
- DR - Mohammed Abdalla Egypt. Domiat G. Hospital: Controversies in GynecologyDokument66 SeitenDR - Mohammed Abdalla Egypt. Domiat G. Hospital: Controversies in Gynecologymadmax500Noch keine Bewertungen
- Hum. Reprod. Update-2016-Donnez-665-86 Myomas Update PDFDokument22 SeitenHum. Reprod. Update-2016-Donnez-665-86 Myomas Update PDFernestosandNoch keine Bewertungen
- Management of Uterine Fibroid 2Dokument37 SeitenManagement of Uterine Fibroid 2api-3705046100% (3)
- Predisposing Factors For Fibroids and Outcome of LDokument10 SeitenPredisposing Factors For Fibroids and Outcome of LAashish KalikaNoch keine Bewertungen
- AdenomyosisDokument16 SeitenAdenomyosisWiwik'RatnaSariPratiwi'100% (2)
- Vaginal Agenesis or HypoplasiaDokument18 SeitenVaginal Agenesis or Hypoplasianikd_6Noch keine Bewertungen
- Uterine Fibroids PDFDokument3 SeitenUterine Fibroids PDFmervat_aastNoch keine Bewertungen
- Embolizacion Uterina FrifroicaDokument8 SeitenEmbolizacion Uterina FrifroicaALGORTONoch keine Bewertungen
- Page 1 of 5: Guidelines/green-Top-Guidelines/gtg - 67 - Endometrial - Hyperplasia PDFDokument5 SeitenPage 1 of 5: Guidelines/green-Top-Guidelines/gtg - 67 - Endometrial - Hyperplasia PDFfitrah fajrianiNoch keine Bewertungen
- New Horizons in Fibroid ManagementDokument10 SeitenNew Horizons in Fibroid ManagementSwastik GhoshNoch keine Bewertungen
- Endometrial Polyps: DR Philip ThomasDokument4 SeitenEndometrial Polyps: DR Philip Thomasapache_sp2208465Noch keine Bewertungen
- Pretreatment of Leiomyoma With GNRH Agonists/Antagonists B of Any ValueDokument5 SeitenPretreatment of Leiomyoma With GNRH Agonists/Antagonists B of Any ValueAdi TriNoch keine Bewertungen
- MR 20 45301Dokument6 SeitenMR 20 45301MOSTOFA SHAMIM FERDOUSNoch keine Bewertungen
- Articulo Endometrio y Menopáusisa 2021Dokument5 SeitenArticulo Endometrio y Menopáusisa 2021Fabiola Milagros Castillo LlicaNoch keine Bewertungen
- DIQUE Polypectomy Possible Endometrial SamplingDokument5 SeitenDIQUE Polypectomy Possible Endometrial Samplingmarjorie Dela CruzNoch keine Bewertungen
- Endometrial Hyperplasia: by Dr. Mervat AliDokument48 SeitenEndometrial Hyperplasia: by Dr. Mervat AliAsh AmeNoch keine Bewertungen
- Phyllodes TumorsDokument4 SeitenPhyllodes TumorsNexi anessaNoch keine Bewertungen
- C. Nodal Status: A. Mitotic Number B. GradeDokument46 SeitenC. Nodal Status: A. Mitotic Number B. GradeOstazNoch keine Bewertungen
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDokument9 SeitenEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyJose Alfredo Juarez VelazquezNoch keine Bewertungen
- Endometrial MalignancyDokument8 SeitenEndometrial MalignancySusmita HalderNoch keine Bewertungen
- Role of Laparoscopic Surgery in The Treatment of Uterine FibroidsDokument9 SeitenRole of Laparoscopic Surgery in The Treatment of Uterine FibroidsCentral Asian StudiesNoch keine Bewertungen
- IJSHR50Dokument12 SeitenIJSHR50OMKAR DANDEKARNoch keine Bewertungen
- Surgical Management of HMBDokument9 SeitenSurgical Management of HMBYasmin AlkhatibNoch keine Bewertungen
- Uterine FibroidsDokument9 SeitenUterine FibroidssalamredNoch keine Bewertungen
- Uterine Myoma: An Individual Case Study OnDokument22 SeitenUterine Myoma: An Individual Case Study OnDeh MehNoch keine Bewertungen
- Ijcam 12 00483Dokument4 SeitenIjcam 12 00483PriyakrishnaVasamsettiNoch keine Bewertungen
- MSN Ii An-Uterine FibroidDokument33 SeitenMSN Ii An-Uterine FibroidSifanaNoch keine Bewertungen
- Endometriosis and Adenomyosis: Bahaa MaliDokument40 SeitenEndometriosis and Adenomyosis: Bahaa Mali'محمد علي' محمد لافيNoch keine Bewertungen
- GynecolMinimInvasiveTher7110-839238 231843Dokument6 SeitenGynecolMinimInvasiveTher7110-839238 231843Isma RotinNoch keine Bewertungen
- Abnormal Uterine BleedingDokument28 SeitenAbnormal Uterine BleedingHuzaifaNoch keine Bewertungen
- Five Emrcs NotesDokument18 SeitenFive Emrcs NotesDeen MohammadNoch keine Bewertungen
- Fibroids Miracle Cure: The Ultimate Fibroids Diet To Heal NaturallyVon EverandFibroids Miracle Cure: The Ultimate Fibroids Diet To Heal NaturallyBewertung: 3.5 von 5 Sternen3.5/5 (7)
- Hysterectomy, (Removal of Uterus) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHysterectomy, (Removal of Uterus) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBewertung: 5 von 5 Sternen5/5 (1)
- WH oDokument1 SeiteWH oAde Churie TanjayaNoch keine Bewertungen
- Developed By: Phillip Graham Captain/ Paramedic Red, White and Blue Fire Protection DistrictDokument29 SeitenDeveloped By: Phillip Graham Captain/ Paramedic Red, White and Blue Fire Protection DistrictAde Churie TanjayaNoch keine Bewertungen
- 02a. - PatCenterCare (Dr. Adib)Dokument22 Seiten02a. - PatCenterCare (Dr. Adib)fairahNoch keine Bewertungen
- Fibromyalgia: o o o o o oDokument2 SeitenFibromyalgia: o o o o o oEsteban OrellanaNoch keine Bewertungen
- Developed By: Phillip Graham Captain/ Paramedic Red, White and Blue Fire Protection DistrictDokument29 SeitenDeveloped By: Phillip Graham Captain/ Paramedic Red, White and Blue Fire Protection DistrictAde Churie TanjayaNoch keine Bewertungen
- Torehj 6 1 PDFDokument20 SeitenTorehj 6 1 PDFSaifuddin HaswareNoch keine Bewertungen
- Frak TurDokument1 SeiteFrak TurSofi ArianiNoch keine Bewertungen
- Peralatan Alkes Rs Type C PDFDokument19 SeitenPeralatan Alkes Rs Type C PDFAde Churie TanjayaNoch keine Bewertungen
- Alcoholic Liver DiseaseDokument22 SeitenAlcoholic Liver DiseaseVikramjeet SinghNoch keine Bewertungen
- Bartilin 2Dokument4 SeitenBartilin 2Ade Churie TanjayaNoch keine Bewertungen
- Pacemaker Therapy in Bifascicular and Trifascicular BlockDokument1 SeitePacemaker Therapy in Bifascicular and Trifascicular BlockAde Churie TanjayaNoch keine Bewertungen
- Immunization Principles and Vaccine Use: (Table 122-1) (Table 122-2)Dokument2 SeitenImmunization Principles and Vaccine Use: (Table 122-1) (Table 122-2)Ade Churie TanjayaNoch keine Bewertungen
- Ncbi HCV 2015Dokument16 SeitenNcbi HCV 2015Ade Churie TanjayaNoch keine Bewertungen
- 2801 6280 1 SM PDFDokument4 Seiten2801 6280 1 SM PDFAde Churie TanjayaNoch keine Bewertungen
- Bartholin's Gland Cyst MarsupializationDokument3 SeitenBartholin's Gland Cyst MarsupializationAde Churie Tanjaya50% (2)
- Bartoli NDokument3 SeitenBartoli NAde Churie TanjayaNoch keine Bewertungen
- SeleniumDokument7 SeitenSeleniumAde Churie TanjayaNoch keine Bewertungen
- Spinal Cord InjuryDokument56 SeitenSpinal Cord InjuryAde Churie TanjayaNoch keine Bewertungen
- 02 Ipfd V1N4 07R13Dokument4 Seiten02 Ipfd V1N4 07R13Ade Churie TanjayaNoch keine Bewertungen
- NorepinefrinDokument9 SeitenNorepinefrinAde Churie TanjayaNoch keine Bewertungen
- ComaDokument67 SeitenComaAde Churie TanjayaNoch keine Bewertungen
- Ipi 107451Dokument5 SeitenIpi 107451Ade Churie TanjayaNoch keine Bewertungen
- Ipi 107451Dokument5 SeitenIpi 107451Ade Churie TanjayaNoch keine Bewertungen
- POPstix Insert OptDokument1 SeitePOPstix Insert OptAde Churie TanjayaNoch keine Bewertungen
- Sindrom Hellp, Eklampsia, Dan Perdarahan Intrakranial: Case SummaryDokument5 SeitenSindrom Hellp, Eklampsia, Dan Perdarahan Intrakranial: Case SummaryAde Churie TanjayaNoch keine Bewertungen
- Male Reproductive SystemDokument8 SeitenMale Reproductive SystemkcNoch keine Bewertungen
- She Comes FirstDokument8 SeitenShe Comes FirstDimas Farayndra PranidhanaNoch keine Bewertungen
- EndometriosisDokument29 SeitenEndometriosisJohnnyDeepNoch keine Bewertungen
- Sexual DeviationsDokument24 SeitenSexual DeviationsMary MayNoch keine Bewertungen
- Abortion Laws in AmericaDokument7 SeitenAbortion Laws in AmericaBinoy SinhaNoch keine Bewertungen
- PlevonorgestrelDokument16 SeitenPlevonorgestrelChris ChowNoch keine Bewertungen
- Pelvic Inflammatory DiseaseDokument8 SeitenPelvic Inflammatory DiseaseAndyan Adlu Prasetyaji0% (1)
- Young Talk, October 2006Dokument3 SeitenYoung Talk, October 2006Straight Talk FoundationNoch keine Bewertungen
- Rupture of UterusDokument5 SeitenRupture of UterussamarbondNoch keine Bewertungen
- Will Balbir Pasha Help Fight: Aids ??Dokument50 SeitenWill Balbir Pasha Help Fight: Aids ??ariefakbarNoch keine Bewertungen
- Insightec - Ultrasound Guided TherapyDokument23 SeitenInsightec - Ultrasound Guided Therapysamanthaokwan1015Noch keine Bewertungen
- 5 Types of Orgasms PDFDokument13 Seiten5 Types of Orgasms PDFRamesh Kumar100% (2)
- Crit Paper 1Dokument8 SeitenCrit Paper 1api-333929199Noch keine Bewertungen
- Pelvic Inflammatory Disease (PID)Dokument23 SeitenPelvic Inflammatory Disease (PID)Diana Rashid100% (1)
- Chapter 05 The Gliding MechanismDokument11 SeitenChapter 05 The Gliding Mechanismwoat86Noch keine Bewertungen
- Health Promotion and MaintenanceDokument170 SeitenHealth Promotion and Maintenancepopota100% (1)
- Contraception Brochure Sample#1Dokument2 SeitenContraception Brochure Sample#1Kelsey NuñezNoch keine Bewertungen
- Ap Lang Synthesis EssayDokument2 SeitenAp Lang Synthesis Essayapi-319010818Noch keine Bewertungen
- FemaraDokument2 SeitenFemaraMyraIntisarNoch keine Bewertungen
- Annotated Bibliography Teen PregnancyDokument5 SeitenAnnotated Bibliography Teen Pregnancyapi-357525581Noch keine Bewertungen
- Report On Adolescent Reproductive Health in SchoolsDokument2 SeitenReport On Adolescent Reproductive Health in SchoolsJESUS MOSA, JR.100% (1)
- Ethics of AbortionDokument16 SeitenEthics of AbortionJames Louis B. Antonio0% (1)
- SOGC CLINICAL PRACTICE GUIDELINE Vaginal Delivery of Breech PresentationDokument8 SeitenSOGC CLINICAL PRACTICE GUIDELINE Vaginal Delivery of Breech PresentationsobgyniaNoch keine Bewertungen
- Tubal LigationDokument3 SeitenTubal LigationFebie GonzagaNoch keine Bewertungen
- Ak 18121952Dokument2 SeitenAk 18121952raghavremNoch keine Bewertungen
- Cha Report Chlamydia Hpeb 553 Artifact For Key Insight 3Dokument8 SeitenCha Report Chlamydia Hpeb 553 Artifact For Key Insight 3api-375325483Noch keine Bewertungen
- DR InstrumentsDokument16 SeitenDR InstrumentsKrisia Castuciano100% (1)
- What Are The Types of Birth Control?Dokument7 SeitenWhat Are The Types of Birth Control?Remy Castelo Santos CortezNoch keine Bewertungen
- Bad Girl's Bible BDSM ChecklistDokument2 SeitenBad Girl's Bible BDSM Checklistbob frost50% (4)
- Miscarriage What Is It?Dokument4 SeitenMiscarriage What Is It?Suseno AjiNoch keine Bewertungen