Beruflich Dokumente
Kultur Dokumente
SM 2
Hochgeladen von
Smitha Kapani gowdaOriginalbeschreibung:
Originaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
SM 2
Hochgeladen von
Smitha Kapani gowdaCopyright:
Verfügbare Formate
Role of genetic factors in the
pathogenesis of aggressive
periodontitis
ALEXANDRE R. VI EI RA & JASI M M. ALBANDAR
Both genetic and environmental factors have roles in
the development of chronic diseases. Some of the
most common chronic disorders, such as heart dis-
ease, diabetes and Alzheimers disease, are associated
with mutations in multiple genes, combined with
environmental effects (116). Available data suggest
that, similarly to these common chronic disorders,
chronic periodontitis and aggressive periodontitis are
also caused by the combined effects of environmental
and genetic factors.
Following a periodontal infection an inammatory
process will ensue in order to fend off the infectious
assault and protect the host. However, this process
may also result in loss of the supporting tissues of
teeth, which may occur through an up-regulation
of pro-inammatory mediators (140) or as a result of
particular defects in the host response to the infec-
tious assault (62). To that extent, both of these mech-
anisms appear to be genetically determined. This
article critically reviews the evidence for a role of
genetic factors in the pathogenesis of aggressive peri-
odontitis and discusses the approaches commonly
used in studies designed to identify genetic risk fac-
tors for this disease.
Role of genetic factors in
periodontal diseases
Syndromic periodontal diseases
Certain monogenic disorders, or single-gene muta-
tions, are associated with severe forms of periodonti-
tis (48), whereas other periodontal disease
phenotypes seem to occur through different genetic
associations. Aggressive forms of severe periodontitis
associated with single-gene diseases or syndromes
are described elsewhere (65). These syndromes are
etiologically diverse and their genetic triggering fac-
tors have been identied (Table 1).
The PapillonLefevre syndrome is an example of
the monogenic disorders that have a periodontal
component. This disease is an autosomal-recessive
trait characterized by a diffuse palmar-plantar kerato-
sis and rapid loss of the periodontal tissue attach-
ment and alveolar bone, and the primary and
permanent teeth are lost at a young age (26). In
patients with PapillonLefevre syndrome periodontal
pathogens do not seem to play a signicant role in
the pathogenesis of the periodontal tissue loss (3). On
the other hand, these patients show immune defects
that are thought to predispose these individuals to
the severe loss of periodontal tissue (65). Studies
show that in the PapillonLef evre syndrome there is a
loss-of-function mutation affecting the cathepsin C
gene (CTSC; MIM 245000) on chromosome 11q14.2,
and this inuences a key enzyme essential in the acti-
vation of certain immune cells and in the regulation
of epithelial cells (30).
Studies have reported the identication of CTSC
mutations in families with prepubertal children
exhibiting aggressive forms of periodontal destruction
but no other systemic clinical manifestations (47, 105,
107). It should be noted that the CTSC mutation
reported by Hart et al. (47) in prepubertal children
with periodontitis is the same mutation previously
reported in a patient with PapillonLef evre syndrome
for which a complete loss of cathepsin C activity was
demonstrated (138). These data suggest that aggres-
sive periodontitis, in some families, represents a par-
tially penetrant PapillonLef evre syndrome (52).
There is evidence that in prepubertal children
exhibiting aggressive periodontitis, mutations segre-
gate in an autosomal-recessive manner, similarly to
92
Periodontology 2000, Vol. 65, 2014, 92106 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Printed in Singapore. All rights reserved
PERIODONTOLOGY 2000
the segregation pattern in the PapillonLef evre
syndrome. It is possible that the reported cases of
periodontitis in prepubertal children (47, 105, 107)
may be associated with a yet-undetected systemic
disorder, and this may explain the autosomal-reces-
sive pattern observed in these subjects. Another
explanation, however, is that these children indeed
exhibited aggressive periodontitis, and as such the
reported inheritance pattern is particular to these
subjects.
Hewitt et al. (52) did not nd a statistically signi-
cant difference in cathepsin C enzyme activity
between a group of 30 subjects with aggressive peri-
odontitis and age- and gender-matched controls. The
study, in addition, found three CTSC mutations and
negligible cathepsin C enzyme activity in one subject
with aggressive periodontitis, suggesting complete
loss of function of cathepsin C.
ChediakHigashi syndrome is another monogenic
disease transmitted in an autosomal-recessive man-
ner and characterized by involvement of teeth with
severe periodontitis (63, 64). In patients with Chediak
Higashi syndrome, mutations have been identied
in the CHS1/LYST gene on chromosome 1q42.3 (MIM
214500), and the proteins encoded by this gene are
thought to be associated with the signicant immune
defects seen in these patients.
Severe periodontal manifestations are also associ-
ated with congenital neutropenia (MIM 202700), cyc-
lic neutropenia (MIM 162800), leukocyte adhesion
deciency type I (MIM 116920) and type II (MIM
266265), glycogen storage disease (MIM 232220),
EhlersDanlos syndrome (MIM 130000) and Cohen
syndrome (MIM 216550) (65). There is also a report of
aggressive periodontitis associated with Fanconi ane-
mia (109). Fanconi anemia is an autosomal-recessive
disorder affecting all bone marrow elements and is
associated with cardiac, renal and limb malforma-
tions as well as with dermal pigmentary changes
(MIM 227650). Fanconi anemia can be caused by
mutation in one of the Fanconi anemia complemen-
tation group genes: FANCA (16q24.3), FANCB
(Xp22.31), FANCC (9q22.3), FANCD1 (13q12.3),
FANCD2 (3p25.3), FANCE (6p22-p21), FANCF (11p15),
FANCG (9p13), FANCJ (17q22), FANCL (2p16.1) and
FANCM (14q21.3). Aggressive periodontitis was also
reported in a Turkish patient with tetraploid/diploid
mosaicism (139), but was not described in another 14
subjects previously reported with tetraploid/diploid
mosaicism (5).
Nonsyndromic periodontal diseases
There is strong evidence for a role of genetic factors
in increasing the host susceptibility to periodontal
diseases (13, 74), particularly aggressive forms of peri-
odontitis. An analysis of clinical parameters of peri-
odontal disease was performed in 75 families to
assess the familial aggregation of indices of periodon-
tal disease (15). The study found evidence for a famil-
ial aggregation of dental plaque measurements after
adjustment for age, gender, race and oral hygiene
habits. The plaque index showed greater familial
resemblance compared with other measures of peri-
odontal disease. Sizable fractions of the variances in
gingival index and attachment loss were also attrib-
uted to differences among families, although these
two variables did not attain statistical signicance in
the study.
The relative contribution of environmental and
host genetic factors to clinical measures of periodon-
tal disease was investigated in twins reared together
or reared apart (88). Probing depth, clinical attach-
ment loss, gingival inammation and dental plaque
Table 1. Syndromes with clinical manifestations of severe periodontitis
Syndrome Mutated gene Chromosome region
PapillonLef evre Cathepsin C (CTSC) 11q14.1q14.3
ChediakHigashi Lysosomal trafcking regulator CHS1/LYST 1q42.1q42.2
Hypophosphatasia ALPL 1p36.12
Congenital and cyclic neutropenia ELANE 19p13.3
Leukocyte adhesion deciency type I Beta-2 integrin chain 21q22.3
Leukocyte adhesion deciency type II GDP-fucose transporter-1 11p11.2
Glycogen storage disease SLC37A4 11q23.3
EhlersDanlos Collagen alpha-1(V) gene (COL5A1) or the
collagen alpha-2(V) gene (COL5A2)
9q34, 2q31
Genetic factors in aggressive periodontitis
93
were assessed in 110 pairs of adult twins consisting of
63 monozygous and 33 dizygous twin pairs reared
together, and 14 monozygous twin pairs reared apart.
A statistically signicant genetic component was
found for gingivitis, probing depth, attachment loss
and dental plaque. Furthermore, it was estimated that
3882% of the population variance for these clinical
measures of periodontal disease may be attributed to
genetic factors. In the latter study group the genetic
variance of alveolar bone height was assessed using
panoramic radiographs, and the estimates of the in-
traclass correlations of alveolar bone heights for the
twin groups were 0.70, 0.52 and 0.55 for the monozy-
gous and dizygous twins reared together and the
monozygous twins reared apart, respectively, suggest-
ing that there is a signicant genetic variance in the
population for alveolar bone height (89).
It has been estimated that approximately half of
the population variance in chronic periodontitis
could be accounted for by genetic factors and that
the inheritance mainly inuences biological, and not
behavioral, variables (90). A large population study in
4,908 twin pairs found that the concordance rates
were 0.38 for monozygotic twins and 0.16 for dizy-
gotic twins, implying that genetic factors make an
important contribution to the risk of chronic peri-
odontitis (24). A more recent population study in
10,000 twin pairs reported that genetic factors con-
tributed to 14% of the variation in tooth loss among
women and to 39% of the variation in tooth loss
among men (95). Furthermore, the study concluded
that genetic factors have a moderate role in the path-
ogenesis of oral diseases and suggested that interac-
tions of genetic and environmental factors may have
an important role.
Several studies investigated gene polymorphisms in
patients with chronic periodontitis. The gene poly-
morphisms explored typically encoded proteins
involved in immune regulation or in other periodon-
tal tissue defects. The rst report of an association of
a specic gene polymorphism with chronic periodon-
titis was for interleukin-1 (72), and several studies
have been published since that report associations
between an array of gene polymorphisms and
increased risk for periodontitis (68). Evidence using a
mouse model suggests discrete sets of differentially
expressed genes are associated with genetically deter-
mined susceptibility or resistance to alveolar bone
loss following infection with the periodontal patho-
gen Porphyromonas gingivalis (43). Other mecha-
nisms of genetic predisposition to chronic
periodontitis have also been investigated and docu-
mented in animal models (13).
Genetic associations in aggressive
periodontitis
The genetic association study approach is useful for
identifying genetic variants that affect susceptibility
to common complex diseases (66, 121). A leading
hypothesis of increased susceptibility to aggressive
periodontitis entails decient host response to peri-
odontal infection (87, 129), particularly infections
with virulent periodontal pathogens (73). It is now
established that genetic factors regulate the innate
immune system (6, 146) and that certain genetic poly-
morphisms may render the immune system defective
and unable to successfully fend off assaults by infect-
ing microorganisms. Genetic factors may play a more
signicant role in the pathogenesis of aggressive peri-
odontitis than in chronic periodontitis (133), and this
may be attributed, to a certain extent, to the signi-
cance of the innate immune system in the pathogen-
esis of this disease (122). Although local etiological
factors are less prevalent in aggressive periodontitis
than in chronic periodontitis (12), alveolar bone loss
and tooth loss are signicantly more pronounced in
aggressive periodontitis. Periodontal tissue destruc-
tion in aggressive periodontitis commences at an
early age, shows a rapid rate of progression and has a
unique pattern where it affects multiple teeth and
occurs bilaterally (4). In addition, differences in the
microbiologic ora or in other environmental factors
do not fully explain the variance in the severity and
age of onset between these two diseases (8, 50).
In the quest to identify genetic risk markers of
aggressive periodontitis, association studies have
focused on genetic factors that regulate the immune
response. We carried out a systematic review of asso-
ciation studies of major gene polymorphisms in
aggressive periodontitis by performing a comprehen-
sive search of the biomedical literature published in
PubMed up to May 2012 using a combination of the
subject heading terms aggressive periodontitis,
periodontal disease, gene, genetic and polymor-
phism.
Neutrophil chemotaxis and functions
Neutrophils represent the rst line of defense against
infection and are an essential component of the
human innate immune system (70). Neutrophils are
attracted to the site of infection in an attempt to elim-
inate or reduce the infectious load, and they kill bac-
teria by oxidative bursts and phagocytose bacteria
and antigens. In an early study, Suzuki et al. (136)
studied neutrophil functions in subjects with different
Vieira & Albandar
94
forms of aggressive periodontitis and in controls. In
addition to uncovering abnormalities in peripheral-
blood neutrophil chemotaxis in more than half of the
subjects with aggressive periodontitis, they also found
abnormalities in other neutrophil functions in signi-
cant numbers of the subjects with aggressive peri-
odontitis. In-vitro assays using radiolabeled bacterial
spores detected defects in phagocytosis in 62% and
29% of subjects with localized and generalized forms
of the disease, respectively, and spore-germination
assays identied defects in the killing of bacteria by
neutrophils in 65% and 38% of such subjects, respec-
tively (136). Subsequent studies provided more infor-
mation on the various neutrophil abnormalities in
patients with aggressive periodontitis, and a compre-
hensive review of this topic has recently been
published (122).
These studies suggest that defects in neutrophil
chemotaxis and function may be key etiological fac-
tors in the pathogenesis of aggressive periodontitis
because these defects impede the host immune
response and contribute to pronounced loss of peri-
odontal tissue. Formyl peptide receptors on the cell
surface of leukocytes are involved in mediating
immune-cell responses to infection. The bacteria-
derived N-formyl-methionyl peptides have high afn-
ity to the N-formyl-methionyl peptide cell receptor,
and after binding to the neutrophil receptor the neu-
trophils become activated, thus triggering them to
migrate to the site of infection. Early studies sug-
gested that neutrophils from the serum of patients
with aggressive periodontitis show impaired chemo-
taxis to these antigens (20, 23) and these ndings
were later validated by several other studies (62, 122).
Conversely, some reports suggest that the abnormal
neutrophil chemotactic response to N-formyl-me-
thionyl peptides is limited to some, but not to all,
cases of aggressive periodontitis (114).
It is believed that major aspects of the innate
immune system are genetically determined (6, 146).
However, certain defects in the innate immune
response to infection may also be induced, such as
defects in neutrophil chemotaxis, phagocytosis and
other functions (1, 9, 10, 69). The human FPR1 gene,
which encodes the N-formyl peptide receptor, was
cloned and sequenced in 1992/1993 (28, 96). Gwinn
et al. (41) studied the frequency of two single nucleo-
tide polymorphisms, 329T>C and 378C>G, in the
FPR1 in a group of African-American patients with
aggressive periodontitis compared with controls, and
reported that 29 of those patients had one or both
single nucleotide polymorphisms, but that the single
nucleotide polymorphisms were not present in any of
the controls. They concluded that these alterations
may play a role in the decreased chemotactic activity
of neutrophils in this disease. By contrast, Zhang
et al. (150) tested the latter hypothesis in a group of
226 ethnically diverse individuals, comprising 111
subjects with aggressive periodontitis and 115 ethni-
cally matched controls, but neither of these two single
nucleotide polymorphisms were detected in the
452 chromosomes sequenced in their study. The
authors therefore concluded that these two polymor-
phisms may not play an etiologic role in aggressive
periodontitis.
A different FPR1 polymorphism (single nucleotide
polymorphism c.348T>C) has also been investigated;
an association of this polymorphism was noted with
aggressive periodontitis in African-American patients,
and mainly the 348T/T genotype was associated with
signicantly impaired polymorphonuclear cell che-
motaxis (81). An in-vitro experiment showed that
phosphoinositide-dependent kinase-1 regulates neu-
trophil chemotaxis (145); this suggests that the
expression and activation levels of phosphoinositide-
dependent kinase-1 which are signicantly reduced
in aggressive periodontitis may explain the impaired
neutrophil chemotaxis in such patients. Another
study in Japanese subjects found signicant associa-
tions of aggressive periodontitis with polymorphisms
at ve functional FPR1 variants (12915C>T,
10056T>C, 8430A>G, 301G>C and 546C>A) and
one haplotype (-12915T-301G-546C) (39).
Several studies have investigated the signicance of
genetic polymorphisms that affect neutrophil func-
tions in aggressive periodontitis. Nebali et al. (103)
studied the genetic basis of neutrophil functions in
Caucasian patients and their results suggest that the
C242T polymorphism of the CYBA gene (which
encodes p22
phox
) was associated with an oxidative
burst in response to challenge with Aggregatibacter
actinomycetemcomitans and that the FccIIa polymor-
phism was associated with the phagocytic index of
Escherichia coli. Ho et al. (53) studied, in Taiwanese
patients, the association of polymorphism of FccIIIb
the neutrophil-specic receptor involved in the
phagocytosis of IgG-opsonized bacteria and found
signicant association with aggressive periodontitis.
A systematic review of 17 studies investigated the
association of three Fcc receptor polymorphisms
(FccRIIA H131R, FccRIIIA F158V and FccRIIIB NA1/
NA2) with susceptibility to aggressive periodontitis
(32). The study concluded that the FccRIIIB NA1/NA2
polymorphism was associated with aggressive peri-
odontitis as well as with chronic periodontitis,
whereas the two other polymorphisms showed only a
Genetic factors in aggressive periodontitis
95
weak association or were not associated with a higher
risk for aggressive periodontitis.
Albandar et al. (2) reported that the serum levels of
IgA reactive to periodontal pathogens were signi-
cantly higher in patients with generalized aggressive
periodontitis compared with healthy controls. Fur-
thermore, neutrophils from patients with periodonti-
tis show increased levels of expression of the FcaRI
receptor (71). Cross-linking of IgA with the Fca recep-
tor on phagocytes triggers an array of host cellular
responses, such as phagocytosis, antibody-dependent
cell-mediated cytotoxicity, superoxide generation and
the release of inammatory mediators (93). Hence, it
may be hypothesized that individuals with increased
expression levels of FcaRI receptor on phagocytes,
and elevated levels of IgA reactive to periodontal
pathogens, may be at higher risk for aggressive
periodontitis.
Relative to this, Kaneko et al. (61) identied a novel
FcaRI gene polymorphism at nucleotide position 324
in the EC1 domain that was associated with a signi-
cantly increased rate of carriage of aggressive peri-
odontitis (65.2%) vs. a control group (42.5%).
Furthermore, they found that neutrophils from
patients with the nt 324 A/A genotype exhibited
decreased phagocytosis compared with patients with
the nt 324 G/G genotype.
Cytokines
Several studies have investigated the association of
aggressive periodontitis with polymorphisms in the
interleukin-1 (IL1) gene cluster and the ndings were
inconsistent. Generally, there is either limited or no
evidence of association between this genotype and
this disease in Caucasian subjects (34, 38, 55, 125).
Meanwhile, some studies maintain that signicant
associations were detected in other race-ethnicity
groups (40, 75).
Interleukin-4 and interleukin-13 are closely related
cytokines and have similar functions and anti-inam-
matory properties (18, 84). It has been shown that
patients with aggressive periodontitis and the 34 TT
and 590 TT interleukin-4 genotypes have signi-
cantly increased expression of IL4 and STAT6 genes
and produce higher concentrations of interleukin-4
in activated CD4
+
cells (36). Two studies investigated
the association of IL4 promoter/intron with compos-
ite genotype (PP
+
/IP
+
) but found no signicant asso-
ciations with aggressive periodontitis in Caucasian,
Brazilian and Japanese patients (35, 115). A study in a
Taiwanese population found an association between
the IL13 1113 CC genotype and a higher frequency
of aggressive periodontitis (144). Furthermore, it has
been shown that T-helper 1 cells from patients homo-
zygous for the 34T and 590T alleles show higher
interferon-c and interleukin-2 expression and signi-
cantly increased interleukin-13 production (37). This
suggests an increased production of interleukin-13 by
the T cells of aggressive periodontitis patients with
the IL4 genotype.
The cytokine interleukin-6 is encoded by the IL6
gene and has pro-inammatory as well as anti-
inammatory functions. One study found that the IL6
polymorphisms 1363 and 1480 may be associated
with increased susceptibility to aggressive periodonti-
tis (99). A meta-analysis of six published studies
found that the IL6 174G allele and 572 C/G poly-
morphisms were associated with aggressive peri-
odontitis (132). Using a large study sample
comprising 534 patients with periodontitis and 231
controls, Nibali et al. (102) concluded that IL6 poly-
morphisms and haplotypes are moderately associated
with periodontitis and that this association was stron-
ger for the localized form of aggressive periodontitis
than for generalized aggressive periodontitis or
chronic periodontitis.
A study in Germans of Caucasian descent evaluated
IL10 polymorphisms at positions 1082G>A,
819C>T and 590C>A, reported that the combina-
tion ATA/ATA was detected only in patients with
aggressive periodontitis and concluded that the hap-
lotype ATA is a low interleukin-10 producer and may
be a risk indicator for this disease (117). A similar
association was reported for the IL10 haplotype ATA
in a group of Taiwanese patients (57). However, three
other studies found no signicant associations
between IL10 polymorphisms and aggressive peri-
odontitis (60, 67, 85). One study, on IL12, reported
signicantly higher frequencies of variant alleles of
IL12Rb2 in Japanese patients with aggressive peri-
odontitis compared with controls (137).
The cytokine interleukin-17 is a central player in
the immune system in complex diseases that inte-
grate innate and adaptive immune mechanisms
(148). This cytokine is secreted by a variety of innate
cells and it has been shown that it exerts a host-
defense role in many infectious diseases, but also pro-
motes inammation and tissue loss in autoimmune
diseases (111). The interleukin-17 receptor (IL-17RA)
is expressed on most host cells and therefore these
cells can potentially respond to this cytokine. The role
of interleukin-17 or its receptor in bone loss triggered
by infection was studied in Il17ra knockout mice
(147). Upon infecting the IL-17RA-decient mice with
the pathogen P. gingivalis, the mice exhibited
Vieira & Albandar
96
reduced serum chemokine levels and reduced neu-
trophil migration to bone, although neutrophils from
these mice functioned normally ex vivo. Furthermore,
the mice showed enhanced periodontal bone loss
reminiscent of a neutrophil deciency.
A study in 102 patients with aggressive periodontitis
and 67 periodontally healthy controls showed that
interleukin-17 was present at signicantly higher con-
centrations in sera from the patients and was barely
detectable in the control individuals (130). The study
concluded that interleukin-17 may play a role in the
pathogenesis of aggressive periodontitis. Another
study, however, found that the concentration of inter-
leukin-17 in the gingival crevicular uid was signi-
cantly lower in the group of patients with aggressive
periodontitis than in the healthy control group (11).
Studies assessing the relationship between IL17 geno-
types and this disease are still lacking.
Vitamin D
Vitamin D plays an important role in bone metabo-
lism and in calcium and phosphorus homeostasis,
and also regulates the expression of a large number of
genes (80, 141). The blood concentration of the pre-
hormone calcifediol (calcidiol) is considered as the
best indicator of a subjects level of vitamin D (49). A
study found higher plasma levels of calcifediol and
osteocalcin and lower serum levels of inorganic phos-
phorus in subjects with aggressive periodontitis than
in healthy controls (78).
The vitamin D receptor (VDR) gene is found not
only in tissues involved in calcium homeostasis, but
also in a variety of cell lines involved primarily in
immune regulation, including mononuclear cells,
dendritic cells, antigen-presenting cells and activated
B lymphocytes and CD4
+
T cells, and it is therefore
thought to play an important role in the pathogenesis
of autoimmune and inammatory diseases (42). A
number of studies investigated the association of
VDR polymorphisms and aggressive periodontitis.
Carriage of the less frequent allele (t) of the VDR TaqI
gene was found to be signicantly associated with
localized aggressive periodontitis in Caucasian sub-
jects from the UK (51) and in Chinese and Italian sub-
jects with aggressive periodontitis (83, 134). Two
studies found signicant associations of the VDR FokI
gene polymorphism with generalized aggressive peri-
odontitis in Korean (113) and Chinese (76) patients.
The latter two studies did not nd signicant associa-
tions with the VDR BsmI or TaqI gene polymorphisms
in Korean patients, or with the VDR BsmI, TaqI or
ApaI gene polymorphisms in Chinese patients. A
recent study reported a meta-analysis of data from 15
studies of aggressive periodontitis, as well as of
chronic periodontitis (29). The study evaluated four
VDR polymorphisms BsmI, TaqI, ApaI and FokI
and concluded that there were no signicant associa-
tions between any of these VDR gene polymorphisms
and aggressive periodontitis. A second study that also
used a meta-analysis methodology to evaluate the
same four VDR polymorphisms concluded that the
four gene loci did not have a statistically signicant
association with aggressive periodontitis when all
race-ethnicity groups were combined (22). However,
the mutant allele F of the FokI locus was associated
with aggressive periodontitis in Asian subjects (odds
ratio = 1.6).
Pattern recognition receptor genes
Pattern recognition receptors are an array of proteins,
expressed by cells of the innate immune system,
which identify patterns associated with pathogen
molecules, yet are distinguishable from host mole-
cules, and therefore contribute to the rapid host
response to microbial pathogens (91). Toll-like recep-
tors comprise a subgroup of pattern recognition
receptors. For example, toll-like receptor-4 detects
lipopolysaccharide from gram-negative bacteria and
is thus important in the activation of the innate
immune system. CD14 is a subgroup of pattern recog-
nition receptors involved in recognition and phagocy-
tosis of bacteria and acts as a co-receptor to toll-like
receptor-2 and toll-like receptor-4 (131, 149).
A study in 73 Caucasian subjects concluded that the
Asp299Gly TLR4 gene polymorphism is associated with
a decreased risk of aggressive periodontitis in western
European patients, whereas no association was found
for the CD14 single nucleotide polymorphisms 159
and 1359 (59). Other studies found no signicant
associations for the Arg753Gln and Arg677Trp poly-
morphisms of the TLR2 gene, or for the Asp299Gly and
Thr399Ile polymorphisms of the TLR4 gene, in Turkish
(33), Chinese (151) or European (106, 120) patients
with aggressive periodontitis. In a meta-analysis of
four studies comprising 295 patients with aggressive
periodontitis and 456 controls, Ozturk & Vieira (112)
concluded that the TLR4 399Ile polymorphism
(TLR4+1196 C>T) may have a protective effect against
aggressive periodontitis (odds ratio = 0.29).
Other polymorphisms
Calprotectin is an antimicrobial protein released from
activated leukocytes, particularly neutrophils, and it
Genetic factors in aggressive periodontitis
97
belongs to the family of calcium-binding S100 pro-
teins encoded by the S100A8 gene in humans. Mem-
bers of this protein family have been implicated in
the calcium-dependent regulation of a variety of
intracellular activities, and it is thought that this pro-
tein is involved in inammation. An enzyme immu-
noassay showed that the plasma concentration of
calprotectin was signicantly higher in patients with
aggressive periodontitis than in controls (135). A
study of 73 Chinese families found that the single
nucleotide polymorphism rs3795391 (A>G) of the
S100A8 gene might contribute to increased suscepti-
bility to aggressive periodontitis (118).
Cyclooxygenases are enzymes involved in the for-
mation of important inammatory mediators, includ-
ing prostaglandins. Cyclooxygenase-2 plays an
important role in mediating periodontal inamma-
tion (94). A study found a signicant association of
the rare G allele of the COX2 haplotype, rs6681231,
with aggressive periodontitis in a large group of Euro-
peans (odds ratio = 1.6 after adjusting for smoking,
diabetes and gender) (94).
A genome-wide analysis found a statistically signi-
cant association of aggressive periodontitis with the
intronic single nucleotide polymorphism rs1537415,
which is located in the glycosyltransferase gene
GLT6D1 (127). Glycosyltransferases are enzymes that
catalyze glycosidic bond formation.
Polymorphism in the promoter region of the sero-
tonin transporter 5-HTT gene is linked to certain psy-
chological conditions such as depression, anxiety and
stress, and was found to be associated with aggressive
periodontitis in Brazilian subjects (25).
Genegene and geneenvironment
interactions
Aggressive as well as chronic forms of periodontitis
are complex diseases that have multifactorial etiology
and in which the effects of various etiological factors
are modied via a complex mechanism of interac-
tions. Genes encode the information for building pro-
teins, and proteins regulate various processes of the
host. While one gene may make only one protein, the
effects of those proteins may interact, and thereby
the expression of one gene may interfere with or
enhance the expression of another gene. Hence, epis-
tasis (or genegene interaction) plays a role in suscep-
tibility to common human diseases (92), including
periodontal diseases.
Most studies of the genetic associations of peri-
odontitis assessed one or a few related variants
(haplotypes). However, aggressive periodontitis
appears to be associated with a few loci, each with
relatively small effects (27). Only a few studies have
investigated the co-occurrence of multiple polymor-
phisms, although more studies may be forthcoming.
A large study of 224 patients and 231 healthy controls
estimated that there is a strong association of the
concomitant presence of the C242T p22phox NADPH
oxidase T allele and FccRIIIb NA1 homozygosity with
generalized aggressive periodontitis in Caucasian
subjects (odds ratio = 30.4) (97). Another study exam-
ined 124 cases and 94 controls and concluded that
the co-occurrence of polymorphisms of CCR2-V64I
and MCP-1-2518A/G genes may be associated with
generalized aggressive periodontitis in female
Chinese subjects, in whom the VV and G+ genotypes,
respectively, apparently impart a protective effect
(odds ratio = 0.2) (152).
A recent study investigated a potential epistasis
among functional gene variants affecting either the
amount or the activity of the protein produced from
each gene and that had previously shown signicant
associations with aggressive periodontitis when
tested individually (126). The study found evidence of
statistically signicant genegene interaction effects
associated with this disease in a group of Italian Cau-
casian subjects comprising 122 cases and 246 con-
trols. The analysis revealed a main independent effect
of the IL6 (572) gene polymorphism (P = 0.0008)
and interactions of IL6 (6106) and IL6 (1480) poly-
morphisms with IL18 (P < 0.0001) and IL4
(P = 0.0001) and with IL2 (P = 0.038). The study also
detected associations of the disease with the seleno-
protein S (SEPS1) gene, independently (P = 0.005)
and in association (P = 0.0002) with IL2. The SEPS1
gene is involved in the stress response in the endo-
plasmic reticulum, redox signaling and inammation
control. Yet another nding in the study is a signi-
cant association of the disease with an interaction
between TNFRSF1B and IL2 genes (P = 0.0008). The
TNFRSF1B gene encodes the tumor necrosis factor
receptor superfamily member 1B protein in humans.
Disease phenotypes are also affected by their envi-
ronment (119). For instance, smoking may potentiate
the associations of CCR2 VV (odds ratio = 7.4) and
MCP1 G+ (odds ratio = 4.9) genotypes with aggres-
sive periodontitis in male Chinese subjects (152).
Also, an interaction between smoking and the VDR
gene 1056 TaqI polymorphism has been shown to
be associated with periodontitis (odds ratio = 1.3)
and with severe disease progression (odds
ratio = 15.2) in Caucasian subjects (100). There is also
evidence suggesting that complex interactions may
Vieira & Albandar
98
take place between the periodontal microbiota and
the host genome. For example, Fcc receptor and IL6
gene polymorphisms have been associated with
increased odds of detecting A. actinomycetemcomi-
tans, P. gingivalis and Tannerella forsythia in patients
with aggressive periodontitis (98, 101).
Major-effect genes vs. small-effect
genes
Traditionally, the prevailing view was that aggressive
periodontitis is transmitted by a Mendelian pattern of
inheritance, and early studies used this assumption
to investigate genetic markers of the disease; for
instance, the study by Amer et al. (7) in which the sig-
nicance of the HLA locus was assessed. Based on
these studies a hypothesis was put forward that
aggressive periodontitis may be caused by a genetic
variant that has a major effect. However, most of the
associations initially reported between genes and the
disease were not conrmed in subsequent studies.
It has been shown that in several complex traits an
initial study often suggests a stronger genetic effect
than is found by subsequent studies (58). In these ini-
tial studies, the overestimation of the disease predis-
position, or protection, conferred by a genetic
polymorphism may be attributed to study bias, as well
as to genuine population diversity. Results from asso-
ciation studies have been systematically revisited, and
reports of meta-analyses of specic candidate genes,
although useful in increasing the understanding of
the variances in the reported literature, have not pro-
vided conclusive evidence in favor of, or against, spe-
cic genetic contributions (32, 68, 104, 106, 122, 132).
More recently, some studies have shifted their
focus towards a genome-wide approach, rather than
a candidate gene approach, thereby contemplating
the possibility that perhaps multiple genes may con-
tribute as causal factors to aggressive periodontitis.
Sch aefer et al. (127) performed a genome-wide asso-
ciation study in two independent phases. In the rst
phase, the genome-wide analysis was performed in a
group of German subjects consisting of 141 patients
with aggressive periodontitis and 500 controls, and in
the second phase the same analysis was performed in
a separate group of German subjects comprising 142
patients and 472 controls. The results of the two inde-
pendent analyses were then compared, and only one
genetic variant (rs1537415) showed a statistically
signicant association with aggressive periodontitis
in both study groups. This single nucleotide
polymorphism is located within intron 2 of the glyco-
syltransferase 6 domain containing 1 (GLT6D1) gene
on chromosome 9 (9q34.3). The authors then validated
the results by replicating their ndings in a third group
of Dutch subjects comprising 164 patients and 368 con-
trols. The results of the latter study are consistent with
the hypothesis that aggressive periodontitis is passed
by a complex mode of inheritance, rather than by a
major gene Mendelian mode. Notably, however, the
latter study did not identify known disease-causing
coding mutations in the gene. Moreover, the GLT6D1
gene was not expressed differently in healthy tissues vs.
inamed gingival tissues. Hence, it is challenging to
interpret the results of this study with respect to a pos-
sible role of this gene in aggressive periodontitis.
Careful ne mapping of a locus previously linked to
aggressive periodontitis also yielded novel results.
One linkage study in African-American families (77)
showed that aggressive periodontitis is linked to the
marker D1S492, located on chromosome 1q, and
identied a susceptibility locus between the markers
D1S196 and D1S533. This region of chromosome 1
(from base pair 165,770,752 to base pair 192,424,848)
includes the cytogenetic regions from 1q24.2 to
1q31.3. The goal was to ne map this region to inves-
tigate the hypothesis that genetic variation located
between 1q24.2 and 1q31.3 contributes to susceptibil-
ity to aggressive periodontitis (21).
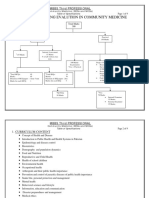
There is evidence that the family with sequence
similarity 5, member C [FAM5C (now called bone
morphogenetic protein/retinoic acid inducible
neural-specic 3 or BRINP3)] gene contributes to
aggressive periodontitis, and it is likely that the
markers rs1935881 and rs1342913 are candidate
functional variants (based on multispecies nucleo-
tide sequence comparisons and electronic tran-
scription-binding site predictions). Notably, the
FAM5C gene is only 3 megabases from the COX2
gene (Fig. 1) located on chromosome 1q. The COX2
gene has previously been associated with localized
aggressive periodontitis in affected individuals in
four African-American multigenerational families
(77). Interestingly, gene markers near the FAM5C
locus showed borderline statistical signicance in a
German study group [see Sch aefer et al. (127);
Table 2]. The pattern of FAM5C functional expres-
sion in aggressive periodontitis was found to be sig-
nicantly higher in diseased periodontal tissues,
and to present a modest, but statistically signi-
cant, correlation with the expression of interleukin-
1beta, interleukin-17A, interleukin-4 and RANKL.
Therefore, it is likely that the FAM5C gene may
modulate or interfere in the cytokine network in
diseased periodontal tissues, and may inuence the
Genetic factors in aggressive periodontitis
99
disease outcome. However, the mechanism of its
effect is still unknown.
Proposed modes of inheritance of
aggressive periodontitis
In 1969, Butler (19) described periodontal ndings in a
family where two of ve siblings had clinical and radio-
graphic features of aggressive periodontitis, the mother
of the children had lost all her teeth in her late teens,
and an aunt and the grandfather of the siblings on the
mothers side had lost their teeth at an early age. Other
early studies (14, 56, 110, 124, 142, 143) also described
aggressive periodontitis case reports clustered in fami-
lies, suggesting a signicant genetic contribution.
The heritability of aggressive periodontitis is esti-
mated to be approximately 30% (31). Segregation
analysis is an important research tool in human
genetics and it tests whether an observed pattern of
phenotypes in families (ratios) is compatible with an
explicit mode of inheritance. Early studies investi-
gated whether Mendelian models of inheritance are
adequate to explain the relationship of genetic factors
and aggressive periodontitis. Aggressive periodontitis
has been described as both X-linked and autosomal.
The rst important validation of the X-linked mode of
transmission of aggressive periodontitis was provided
by Melnick et al. (86), who presented the most com-
plete study to that date and concluded that the
inheritance mode is X-linked dominant with reduced
penetrance. This conclusion was based on their
assessment that the female:male ratio among affected
persons was approximately 2:1 and that there was no
father-to-son transmission of the disease.
However, the results of most other studies are not
consistent with the X-linked mode of transmission,
and subsequent studies with larger and more com-
plete samples documented father-to-son transmis-
sion of aggressive periodontitis, supporting an
autosomal mode (45). Also, female subjects were
shown to be three times more likely than male sub-
jects to be initially ascertained as aggressive peri-
odontitis probands (44) and this bias may have
contributed to the difculties in validating the mode
of inheritance of the disease.
Hodge et al. (54) characterized the inheritance
mode in their study sample as either autosomal domi-
nant or X-linked dominant. Long et al. (79) compared
the likelihood of autosomal-recessive and X-linked
dominant inheritance patterns and concluded that
the X-linked dominant hypothesis is inadequate.
Sax en (124) examined a study group comprising 31
subjects with aggressive periodontitis, 60 parents, 64
siblings and three offspring children, and concluded
that the disease inheritance pattern is consistent with
an autosomal-recessive trait. The same authors later
published a second report (123) in 30 families and
again concluded that their data concurred with the
hypothesis of autosomal-recessive inheritance of
aggressive periodontitis. Beaty et al. (14) studied this
relationship in 28 families, and also suggested that
Table 2. Single nucleotide polymorphisms associated with the FAM5C gene in German patients with aggressive peri-
odontitis
Single nucleotide polymorphism P-value Odds ratio 95% condence interval Phenotype
rs2789394 0.00021 1.66 1.272.17 Generalized aggressive periodontitis
rs10798049 0.00026 1.99 1.372.88 Localized aggressive periodontitis
rs10911886 0.00039 1.94 1.342.82 Localized aggressive periodontitis
rs10911887 0.00015 2.02 1.402.93 Localized aggressive periodontitis
rs6681231 0.00032 1.86 1.322.61 Localized aggressive periodontitis
185000000 186000000 189000000
1q31.1
190000000
rs10737562 rs10911902
rs4140564
NHGRI Catalog of Published Genome-Wide Association Studies
UCSC Genes Based on RefSeq , Uniport , GenBank, CCDS and Comparative Genomics
RNF2
AF508905
AF510427
HMCN1
TPR
PLA2G4A
C1orf99 PTGS2
PRG4
HMCN1 EDEM3
EDEM3
rs1400544
rs1935881
DBCCR1L
FAM5C
188000000
Chromosome Bands Localized by FISH Mapping Clones
187000000
2 Mb
1q25.3
Fig. 1. The family with sequence similarity 5, member C (FAM5C) gene is about 3 megabases from the cyclooxygenase 2
(COX2 or PTGS2) gene on chromosome 1q. Obtained from the UCSC Genome Browser on Human, February 2009 assembly.
Vieira & Albandar
100
aggressive periodontitis is inherited in an autosomal-
recessive manner. However, the latter authors noted
a relatively high (40%) type II error in their data when
comparing simulations of competing models.
An autosomal-dominant mode of transmission of
aggressive periodontitis was rst suggested in a large
ve-generation extended-family study (16). Further-
more, a robust study that included 100 families ascer-
tained through 104 probands with aggressive
periodontitis (both localized and generalized forms)
was consistent with an autosomal-dominant locus,
with 70% penetrance for African-American subjects
and 73% for Caucasian subjects (82). Also, ndings of
other studies suggest an autosomal-dominant inheri-
tance mode of this disease (44, 45, 54).
Although some studies have suggested an autoso-
mal-recessive inheritance of aggressive periodontitis,
the issue of imposing age limitations when the phe-
notype (aggressive periodontitis) is ascertained may
be confounding the genetic segregation analysis.
Individuals with aggressive periodontitis whose age is
beyond that dened in the case denition may be
assigned a different case category, such as severe
chronic periodontitis, and therefore the subject is
denoted as unaffected in the genetic segregation
analysis. This could result in a dominant form of the
disease appearing to be recessive.
In addition to the age limitations in clinical pheno-
typic diagnosis of the disease, the inconsistent results
regarding the inheritance mode of aggressive peri-
odontitis may also be attributed to a number of other
factors, such as differences in the race and gender
composition of the samples in these studies, the
methods used to ascertain the phenotypes and other
factors. It has been acknowledged that problems exist
with regards to the methodology of genetic modeling
used in these studies, including the availability of lim-
ited family data, problems with phenotype assign-
ment of adults by the use of previous dental records
and a presumed gender bias in the participation in
these studies (17, 45). Hence, adequately designed
studies are needed for exhaustive evaluation and test-
ing to verify the validity of these inheritance models.
If one would infer from this review that aggressive
periodontitis has a Mendelian inheritance, then the
assumption is that this disease is caused by one or
more major genes. However, over the past decade
several studies have investigated potential candidate
genes to test this hypothesis, but no major causal
gene has been identied (128). de Carvalho et al. (27)
performed a study in 74 extended families and found
an excess of heterozygous transmission as the best-t
model explaining the inheritance pattern of the
families segregating aggressive periodontitis. This
suggests that a limited number of genes, each with a
relatively small effect, may contribute to the develop-
ment of the disease. Hence, instead of chasing a sin-
gle major gene, research should be focused on a few
gene variants that may be contributing to the disease
occurrence, and with each gene variant potentially
affecting a small percentage of the cases. It should be
noted that genetic studies of aggressive periodontitis
have often examined limited numbers of families
(typically, 10 or fewer), and this may partly explain
the inconsistent ndings in previous studies reviewed
above, and the conjecture that autosomal Mendelian
models may be the best-t models. On the other
hand, studies with larger numbers of families suggest
differently. For instance, Marazita et al. (82), who
examined 104 families, reported that incomplete pen-
etrance of 30% was present, clearly suggesting that
typical Mendelian models are not the best-t models
for aggressive periodontitis.
To that extent, there is some evidence of associa-
tions between the gene loci 1q25, 4q and 11q14 and
aggressive periodontitis. A haplotype analysis detected
an association between localized aggressive peri-
odontitis and a locus on chromosome 1q25 region
D1S492 in four out of eight African-American families
studied (77). Although this chromosomal region also
includes the COX2 gene (the precursor of prostaglan-
din E) which plays a role in the pathogenesis of peri-
odontal diseases (108), the study did not nd a
mutation in the COX2 gene in these patients (39).
Boughman et al. (16) demonstrated linkage of a
polymorphism in the gene encoding vitamin D-bind-
ing protein (GC) located on chromosome 4q12q13,
with an apparently dominant form of aggressive peri-
odontitis, which co-segregates with dentinogenesis
imperfecta in one large kindred. However, Hart et al.
(46) assessed linkage with 11 markers on chromo-
some 4q, including the GC gene, in 19 extended kin-
dreds (15 African American and four Caucasian) with
aggressive periodontitis , and the statistical analysis
excluded linkage between susceptibility for the dis-
ease and this chromosomal region. Hence, it is likely
that the subjects studied by Boughman et al. (16)
may have had an uncommon form of aggressive peri-
odontitis associated with the chromosome 4q region.
References
1. Agarwal S, Suzuki JB, Piesco NP, Aichelmann-Reidy MB.
Neutrophil function in juvenile periodontitis: induction of
adherence. Oral Microbiol Immunol 1994: 9: 262271.
Genetic factors in aggressive periodontitis
101
2. Albandar JM, DeNardin AM, Adesanya MR, Diehl SR, Winn
DM. Associations between serum antibody levels to peri-
odontal pathogens and early-onset periodontitis. J Period-
ontol 2001: 72: 14631469.
3. Albandar JM, Khattab R, Monem F, Barbuto SM, Paster BJ.
The subgingival microbiota of Papillon-Lefevre syndrome.
J Periodontol 2012: 83: 902908.
4. Albandar JM. Aggressive periodontitis: case denition and
diagnostic criteria. Periodontol 2000 2014: 65: 1326.
5. Alonso L, Melaragno I, Bortolai A, Takeno S, Brunoni D.
Tetraploid/diploid mosaicism: case report and review of
the literature. Ann Genet 2002: 45: 177180.
6. Alper S, Laws R, Lackford B, Boyd WA, Dunlap P, Freed-
man JH, Schwartz DA. Identication of innate immunity
genes and pathways using a comparative genomics
approach. Proc Natl Acad Sci USA 2008: 105: 70167021.
7. Amer A, Singh G, Darke C, Dolby AE. Association between
HLA antigens and periodontal disease. Tissue Antigens
1988: 31: 5358.
8. Armitage GC. Comparison of the microbiological features
of chronic and aggressive periodontitis. Periodontol 2000
2010: 53: 7088.
9. Ashkenazi M, White RR, Dennison DK. Neutrophil modu-
lation by Actinobacillus actinomycetemcomitans. I. Che-
motaxis, surface receptor expression and F-actin
polymerization. J Periodontal Res 1992: 27: 264273.
10. Ashkenazi M, White RR, Dennison DK. Neutrophil modu-
lation by Actinobacillus actinomycetemcomitans. II. Phago-
cytosis and development of respiratory burst. J Periodontal
Res 1992: 27: 457465.
11. Ay ZY, Yilmaz G, Ozdem M, Kocak H, Sutcu R, Uskun E,
Tonguc MO, Kirzioglu F. The gingival crevicular uid levels
of interleukin-11 and interleukin-17 in patients with
aggressive periodontitis. J Periodontol 2012: 83: 14251431.
12. Baer PN. The case for periodontosis as a clinical entity.
J Periodontol 1971: 42: 516520.
13. Baker PJ, Roopenian DC. Genetic susceptibility to chronic
periodontal disease. Microbes Infect 2002: 4: 11571167.
14. Beaty TH, Boughman JA, Yang P, Astemborski JA, Suzuki
JB. Genetic analysis of juvenile periodontitis in families
ascertained through an affected proband. Am J Hum Genet
1987: 40: 443452.
15. Beaty TH, Colyer CR, Chang YC, Liang KY, Graybeal JC,
Muhammad NK, Levin LS. Familial aggregation of peri-
odontal indices. J Dent Res 1993: 72: 544551.
16. Boughman JA, Halloran SL, Roulston D, Schwartz S, Suzuki
JB, Weitkamp LR, Wenk RE, Wooten R, Cohen MM. An
autosomal-dominant form of juvenile periodontitis: its
localization to chromosome 4 and linkage to dentinogene-
sis imperfecta and Gc. J Craniofac Genet Dev Biol 1986: 6:
341350.
17. Boughman JA, Beaty TH, Yang P, Goodman SB, Wooten
RK, Suzuki JB. Problems of genetic model testing in early
onset periodontitis. J Periodontol 1988: 59: 332337.
18. Brubaker JO, Montaner LJ. Role of interleukin-13 in innate
and adaptive immunity. Cell Mol Biol (Noisy-le-grand)
2001: 47: 637651.
19. Butler JH. A familial pattern of juvenile periodontitis (peri-
odontosis). J Periodontol 1969: 40: 115118.
20. Cainciola LJ, Genco RJ, Patters MR, McKenna J, van Oss
CJ. Defective polymorphonuclear leukocyte function in a
human periodontal disease. Nature 1977: 265: 445447.
21. Carvalho FM, Tinoco EM, Deeley K, Duarte PM, Faveri M,
Marques MR, Mendonca AC, Wang X, Cuenco K, Menezes
R, Garlet GP, Vieira AR. FAM5C contributes to aggressive
periodontitis. PLoS ONE 2010: 5: e10053.
22. Chen L, Li H, Zhang P, Wang S. Association between vita-
min D receptor polymorphisms and periodontitis: a meta-
analysis. J Periodontol 2011: 83: 10951103.
23. Clark RA, Page RC, Wilde G. Defective neutrophil chemo-
taxis in juvenile periodontitis. Infect Immun 1977: 18: 694
700.
24. Corey LA, Nance WE, Hofstede P, Schenkein HA. Self-
reported periodontal disease in a Virginia twin population.
J Periodontol 1993: 64: 12051208.
25. Costa JE, Gomes CC, Cota LO, Pataro AL, Silva JF, Gomez
RS, Costa FO. Polymorphism in the promoter region of the
gene for 5-HTT in individuals with aggressive periodonti-
tis. J Oral Sci 2008: 50: 193198.
26. Dalgic B, Bukulmez A, Sari S. Eponym: Papillon-Lefevre
syndrome. Eur J Pediatr 2011: 170: 689691.
27. de Carvalho FM, Tinoco EM, Govil M, Marazita ML, Vieira
AR. Aggressive periodontitis is likely inuenced by a few
small effect genes. J Clin Periodontol 2009: 36: 468473.
28. De Nardin E, Radel SJ, Lewis N, Genco RJ, Hammarskjold
M. Identication of a gene encoding for the human formyl
peptide receptor. Biochem Int 1992: 26: 381387.
29. Deng H, Liu F, Pan Y, Jin X, Wang H, Cao J. BsmI, TaqI,
ApaI, and FokI polymorphisms in the vitamin D receptor
gene and periodontitis: a meta-analysis of 15 studies
including 1338 cases and 1302 controls. J Clin Periodontol
2011: 38: 199207.
30. Dickinson DP. Cysteine peptidases of mammals: their bio-
logical roles and potential effects in the oral cavity and
other tissues in health and disease. Crit Rev Oral Biol Med
2002: 13: 238275.
31. Diehl SR, Wu T, Michalowicz BS, Brooks CN, Califano JV,
Burmeister JA, Schenkein HA. Quantitative measures of
aggressive periodontitis show substantial heritability and
consistency with traditional diagnoses. J Periodontol 2005:
76: 279288.
32. Dimou NL, Nikolopoulos GK, Hamodrakas SJ, Bagos PG.
Fcc receptor polymorphisms and their association with
periodontal disease: a meta-analysis. J Clin Periodontol
2010: 37: 255265.
33. Emingil G, Berdeli A, Baylas H, Saygan BH, Gurkan A, Kose
T, Atilla G. Toll-like receptor 2 and 4 gene polymorphisms
in generalized aggressive periodontitis. J Periodontol 2007:
78: 19681977.
34. Fiebig A, Jepsen S, Loos BG, Scholz C, Schafer C, Ruhling
A, Nothnagel M, Eickholz P, van der Velden U, Schenck K,
Schreiber S, Grossner-Schreiber B. Polymorphisms in the
interleukin-1 (IL1) gene cluster are not associated with
aggressive periodontitis in a large Caucasian population.
Genomics 2008: 92: 309315.
35. Gonzales JR, Kobayashi T, Michel J, Mann M, Yoshie H,
Meyle J. Interleukin-4 gene polymorphisms in Japanese
and Caucasian patients with aggressive periodontitis.
J Clin Periodontol 2004: 31: 384389.
36. Gonzales JR, Groger S, Haley G, Bodeker RH, Meyle J.
The interleukin-4 34TT and 590TT genotype is corre-
lated with increased expression and protein production
in aggressive periodontitis. Mol Immunol 2010: 47: 701
705.
Vieira & Albandar
102
37. Gonzales JR, Groger S, Haley G, Bodeker RH, Meyle J. Pro-
duction of interleukin-13 is inuenced by the interleukin-4
34TT and 590TT genotype in patients with aggressive
periodontitis. Scand J Immunol 2011: 73: 128134.
38. Grigoriadou ME, Koutayas SO, Madianos PN, Strub JR.
Interleukin-1 as a genetic marker for periodontitis: review
of the literature. Quintessence Int 2010: 41: 517525.
39. Gunji T, Onouchi Y, Nagasawa T, Katagiri S, Watanabe H,
Kobayashi H, Arakawa S, Noguchi K, Hata A, Izumi Y, Is-
hikawa I. Functional polymorphisms of the FPR1 gene and
aggressive periodontitis in Japanese. Biochem Biophys Res
Commun 2007: 364: 713.
40. Guzeldemir E, Gunhan M, Ozcelik O, Tastan H. Interleu-
kin-1 and tumor necrosis factor-alpha gene polymor-
phisms in Turkish patients with localized aggressive
periodontitis. J Oral Sci 2008: 50: 151159.
41. Gwinn MR, Sharma A, De Nardin E. Single nucleotide
polymorphisms of the N-formyl peptide receptor in
localized juvenile periodontitis. J Periodontol 1999: 70:
11941201.
42. Haroon M, Fitzgerald O. Vitamin D and its emerging role
in immunopathology. Clin Rheumatol 2012: 31: 199202.
43. Hart GT, Shaffer DJ, Akilesh S, Brown AC, Moran L, Roope-
nian DC, Baker PJ. Quantitative gene expression proling
implicates genes for susceptibility and resistance to alveo-
lar bone loss. Infect Immun 2004: 72: 44714479.
44. Hart TC, Marazita ML, Schenkein HA, Brooks CN, Gunsol-
ley JG, Diehl SR. No female preponderance in juvenile
periodontitis after correction for ascertainment bias. J Pe-
riodontol 1991: 62: 745749.
45. Hart TC, Marazita ML, Schenkein HA, Diehl SR. Re-inter-
pretation of the evidence for X-linked dominant
inheritance of juvenile periodontitis. J Periodontol 1992:
63: 169173.
46. Hart TC, Marazita ML, McCanna KM, Schenkein HA, Diehl
SR. Reevaluation of the chromosome 4q candidate region
for early onset periodontitis. Hum Genet 1993: 91: 416422.
47. Hart TC, Hart PS, Michalec MD, Zhang Y, Marazita ML,
Cooper M, Yassin OM, Nusier M, Walker S. Localisation of
a gene for prepubertal periodontitis to chromosome 11q14
and identication of a cathepsin C gene mutation. J Med
Genet 2000: 37: 95101.
48. Hart TC, Atkinson JC. Mendelian forms of periodontitis.
Periodontol 2000 2007: 45: 95112.
49. Heaney RP. Functional indices of vitamin D status and
ramications of vitamin D deciency. Am J Clin Nutr 2004:
80: 1706S1709S.
50. Heller D, Silva-Boghossian CM, do Souto RM, Colombo
AP. Subgingival microbial proles of generalized aggres-
sive and chronic periodontal diseases. Arch Oral Biol 2012:
57: 973980.
51. Hennig BJ, Parkhill JM, Chapple IL, Heasman PA, Taylor JJ.
Association of a vitamin D receptor gene polymorphism
with localized early-onset periodontal diseases. J Periodon-
tol 1999: 70: 10321038.
52. Hewitt C, McCormick D, Linden G, Turk D, Stern I, Wal-
lace I, Southern L, Zhang L, Howard R, Bullon P, Wong M,
Widmer R, Gaffar KA, Awawdeh L, Briggs J, Yaghmai R,
Jabs EW, Hoeger P, Bleck O, R udiger SG, Petersilka G, Bat-
tino M, Brett P, Hattab F, Al-Hamed M, Sloan P, Toomes
C, Dixon M, James J, Read AP, Thakker N. The role of
cathepsin C in Papillon-Lefevre syndrome, prepubertal
periodontitis, and aggressive periodontitis. Hum Mutat
2004: 23: 222228.
53. Ho YP, Yang YH, Ho KY, Wu YM, Tsai CC. The association
of Fcc receptor IIIb genetic polymorphism and susceptibil-
ity to periodontitis in Taiwanese individuals. J Clin Period-
ontol 2010: 37: 145151.
54. Hodge PJ, Teague PW, Wright AF, Kinane DF. Clinical and
genetic analysis of a large North European Caucasian fam-
ily affected by early-onset periodontitis. J Dent Res 2000:
79: 857863.
55. Hodge PJ, Riggio MP, Kinane DF. Failure to detect an asso-
ciation with IL1 genotypes in European Caucasians with
generalised early onset periodontitis. J Clin Periodontol
2001: 28: 430436.
56. Hoffman ID. Familial occurrence of juvenile periodontitis
with varied treatment of one of the siblings with ve-year
follow-up. Case report. J Periodontol 1983: 54: 4449.
57. Hu KF, Huang KC, Ho YP, Lin YC, Ho KY, Wu YM, Yang
YH, Tsai CC. Interleukin-10 (592 C/A) and interleukin-
12B (+16974 A/C) gene polymorphisms and the interleu-
kin-10 ATA haplotype are associated with periodontitis in
a Taiwanese population. J Periodontal Res 2009: 44: 378
385.
58. Ioannidis JP, Ntzani EE, Trikalinos TA, Contopoulos-Ioan-
nidis DG. Replication validity of genetic association stud-
ies. Nat Genet 2001: 29: 306309.
59. James JA, Poulton KV, Haworth SE, Payne D, McKay IJ,
Clarke FM, Hughes FJ, Linden GJ. Polymorphisms of TLR4
but not CD14 are associated with a decreased risk of
aggressive periodontitis. J Clin Periodontol 2007: 34: 111
117.
60. Jaradat SM, Ababneh KT, Jaradat SA, Abbadi MS, Taha AH,
Karasneh JA, Haddad HI. Association of interleukin-10
gene promoter polymorphisms with chronic and aggres-
sive periodontitis. Oral Dis 2012: 18: 271279.
61. Kaneko S, Kobayashi T, Yamamoto K, Jansen MD, van de
Winkel JG, Yoshie H. A novel polymorphism of FcaRI
(CD89) associated with aggressive periodontitis. Tissue
Antigens 2004: 63: 572577.
62. Kantarci A, Oyaizu K, Van Dyke TE. Neutrophil-mediated
tissue injury in periodontal disease pathogenesis: ndings
from localized aggressive periodontitis. J Periodontol 2003:
74: 6675.
63. Kaplan J, De Domenico I, Ward DM. Chediak-Higashi syn-
drome. Curr Opin Hematol 2008: 15: 2229.
64. Khocht A, Viera-Negron YE, Ameri A, Abdelsayed R. Peri-
odontitis associated with Chediak-Higashi syndrome in a
young African American male. J Int Acad Periodontol 2010:
12: 4955.
65. Khocht A, Albandar JM. Aggressive forms of periodontitis
secondary to systemic disorders. Periodontol 2000 2014:
65: 134148.
66. Khoury MJ, Yang Q. The future of genetic studies of com-
plex human diseases: an epidemiologic perspective. Epide-
miology 1998: 9: 350354.
67. Kinane DF, Hodge P, Eskdale J, Ellis R, Gallagher G. Analy-
sis of genetic polymorphisms at the interleukin-10 and
tumour necrosis factor loci in early-onset periodontitis.
J Periodontal Res 1999: 34: 379386.
68. Kinane DF, Hart TC. Genes and gene polymorphisms asso-
ciated with periodontal disease. Crit Rev Oral Biol Med
2003: 14: 430449.
Genetic factors in aggressive periodontitis
103
69. Klempner MS, Noring R, Mier JW, Atkins MB. An acquired
chemotactic defect in neutrophils from patients receiving
interleukin-2 immunotherapy. N Engl J Med 1990: 322:
959965.
70. Kobayashi SD, Voyich JM, Burlak C, DeLeo FR. Neutrophils
in the innate immune response. Arch Immunol Ther Exp
(Warsz) 2005: 53: 505517.
71. Kobayashi T, Yamamoto K, Sugita N, van Spriel AB, Kane-
ko S, van de Winkel JG, Yoshie H. Effective in vitro clear-
ance of Porphyromonas gingivalis by Fc alpha receptor I
(CD89) on gingival crevicular neutrophils. Infect Immun
2001: 69: 29352942.
72. Kornman KS, Crane A, Wang HY, di Giovine FS, Newman
MG, Pirk FW, Wilson TG Jr, Higginbottom FL, Duff GW.
The interleukin-1 genotype as a severity factor in adult
periodontal disease. J Clin Periodontol 1997: 24: 7277.
73. Kulkarni C, Kinane DF. Host response in aggressive peri-
odontitis. Periodontol 2000 2014: 65: 7991.
74. Laine ML, Crielaard W, Loos BG. Genetic susceptibility to
periodontitis. Periodontol 2000 2012: 58: 3768.
75. Li QY, Zhao HS, Meng HX, Zhang L, Xu L, Chen ZB, Shi D,
Feng XH, Zhu XL. Association analysis between interleu-
kin-1 family polymorphisms and generalized aggressive
periodontitis in a Chinese population. J Periodontol 2004:
75: 16271635.
76. Li S, Yang MH, Zeng CA, Wu WL, Huang XF, Ji Y, Zeng JQ.
Association of vitamin D receptor gene polymorphisms in
Chinese patients with generalized aggressive periodontitis.
J Periodontal Res 2008: 43: 360363.
77. Li Y, Xu L, Hasturk H, Kantarci A, DePalma SR, Van Dyke
TE. Localized aggressive periodontitis is linked to human
chromosome 1q25. Hum Genet 2004: 114: 291297.
78. Liu K, Meng H, Tang X, Xu L, Zhang L, Chen Z, Shi D,
Feng X, Lu R. Elevated plasma calcifediol is associated
with aggressive periodontitis. J Periodontol 2009: 80:
11141120.
79. Long JC, Nance WE, Waring P, Burmeister JA, Ranney RR.
Early onset periodontitis: a comparison and evaluation of
two proposed modes of inheritance. Genet Epidemiol
1987: 4: 1324.
80. Makariou S, Liberopoulos EN, Elisaf M, Challa A. Novel
roles of vitamin D in disease: what is new in 2011? Eur J
Intern Med 2011: 22: 355362.
81. Maney P, Emecen P, Mills JS, Walters JD. Neutrophil form-
ylpeptide receptor single nucleotide polymorphism
348T>C in aggressive periodontitis. J Periodontol 2009: 80:
492498.
82. Marazita ML, Burmeister JA, Gunsolley JC, Koertge TE,
Lake K, Schenkein HA. Evidence for autosomal dominant
inheritance and race-specic heterogeneity in early-onset
periodontitis. J Periodontol 1994: 65: 623630.
83. Martelli FS, Mengoni A, Martelli M, Rosati C, Fanti E. VDR
TaqI polymorphism is associated with chronic periodonti-
tis in Italian population. Arch Oral Biol 2011: 56: 1494
1498.
84. McKenzie AN. Regulation of T helper type 2 cell immunity
by interleukin-4 and interleukin-13. Pharmacol Ther 2000:
88: 143151.
85. Mellati E, Arab HR, Tavakkol-Afshari J, Ebadian AR, Radvar
M. Analysis of 1082 IL-10 gene polymorphism in Iranian
patients with generalized aggressive periodontitis. Med Sci
Monit 2007: 13: CR510CR514.
86. Melnick M, Shields ED, Bixler D. Periodontosis: a pheno-
typic and genetic analysis. Oral Surg Oral Med Oral Pathol
1976: 42: 3241.
87. Meng H, Xu L, Li Q, Han J, Zhao Y. Determinants of host
susceptibility in aggressive periodontitis. Periodontol 2000
2007: 43: 133159.
88. Michalowicz BS, Aeppli D, Virag JG, Klump DG, Hinrichs
JE, Segal NL, Bouchard TJ Jr, Pihlstrom BL. Periodontal
ndings in adult twins. J Periodontol 1991: 62: 293299.
89. Michalowicz BS, Aeppli DP, Kuba RK, Bereuter JE, Conry
JP, Segal NL, Bouchard TJ Jr, Pihlstrom BL. A twin study of
genetic variation in proportional radiographic alveolar
bone height. J Dent Res 1991: 70: 14311435.
90. Michalowicz BS, Diehl SR, Gunsolley JC, Sparks BS, Brooks
CN, Koertge TE, Califano JV, Burmeister JA, Schenkein HA.
Evidence of a substantial genetic basis for risk of adult
periodontitis. J Periodontol 2000: 71: 16991707.
91. Modlin RL. Innate immunity: ignored for decades, but not
forgotten. J Invest Dermatol 2012: 132: 882886.
92. Moore JH. The ubiquitous nature of epistasis in determin-
ing susceptibility to common human diseases. Hum Hered
2003: 56: 7382.
93. Morton HC, Brandtzaeg P. CD89: the human myeloid IgA
Fc receptor. Arch Immunol Ther Exp (Warsz) 2001: 49:
217229.
94. Morton RS, Dongari-Bagtzoglou AI. Cyclooxygenase-2 is
upregulated in inamed gingival tissues. J Periodontol
2001: 72: 461469.
95. Mucci LA, Bjorkman L, Douglass CW, Pedersen NL. Envi-
ronmental and heritable factors in the etiology of oral dis-
easesa population-based study of Swedish twins. J Dent
Res 2005: 84: 800805.
96. Murphy PM, Tiffany HL, McDermott D, Ahuja SK.
Sequence and organization of the human N-formyl
peptide receptor-encoding gene. Gene 1993: 133: 285
290.
97. Nibali L, Parkar M, Brett P, Knight J, Tonetti MS, Grifths
GS. NADPH oxidase (CYBA) and FcgammaR polymor-
phisms as risk factors for aggressive periodontitis: a case
control association study. J Clin Periodontol 2006: 33: 529
539.
98. Nibali L, Ready DR, Parkar M, Brett PM, Wilson M, Tonetti
MS, Grifths GS. Gene polymorphisms and the prevalence
of key periodontal pathogens. J Dent Res 2007: 86: 416
420.
99. Nibali L, Grifths GS, Donos N, Parkar M, DAiuto F, To-
netti MS, Brett PM. Association between interleukin-6 pro-
moter haplotypes and aggressive periodontitis. J Clin
Periodontol 2008: 35: 193198.
100. Nibali L, Parkar M, DAiuto F, Suvan JE, Brett PM, Grifths
GS, Rosin M, Schwahn C, Tonetti MS. Vitamin D receptor
polymorphism (1056 Taq-I) interacts with smoking for
the presence and progression of periodontitis. J Clin Peri-
odontol 2008: 35: 561567.
101. Nibali L, Tonetti MS, Ready D, Parkar M, Brett PM, Donos
N, DAiuto F. Interleukin-6 polymorphisms are associated
with pathogenic bacteria in subjects with periodontitis.
J Periodontol 2008: 79: 677683.
102. Nibali L, DAiuto F, Donos N, Grifths GS, Parkar M, To-
netti MS, Humphries SE, Brett PM. Association between
periodontitis and common variants in the promoter of the
interleukin-6 gene. Cytokine 2009: 45: 5054.
Vieira & Albandar
104
103. Nibali L, ODea M, Bouma G, Parkar M, Thrasher AJ, Burns
S, Donos N. Genetic variants associated with neutrophil
function in aggressive periodontitis and healthy controls.
J Periodontol 2010: 81: 527534.
104. Nikolopoulos GK, Dimou NL, Hamodrakas SJ, Bagos PG.
Cytokine gene polymorphisms in periodontal disease: a
meta-analysis of 53 studies including 4178 cases and 4590
controls. J Clin Periodontol 2008: 35: 754767.
105. Noack B, G orgens H, Hoffmann T, Fanghanel J, Kocher T,
Eickholz P, Schackert HK. Novel mutations in the cathep-
sin C gene in patients with pre-pubertal aggressive peri-
odontitis and Papillon-Lefvre syndrome. J Dent Res 2004:
83: 368370.
106. Noack B, Gorgens H, Lorenz K, Ziegler A, Hoffmann T,
Schackert HK. TLR4 and IL-18 gene variants in aggressive
periodontitis. J Clin Periodontol 2008: 35: 10201026.
107. Noack B, G orgens H, Schacher B, Puklo M, Eickholz P,
Hoffmann T, Schackert HK. Functional Cathepsin C muta-
tions cause different Papillon-Lefvre syndrome pheno-
types. J Clin Periodontol 2008: 35: 311316.
108. Noguchi K, Ishikawa I. The roles of cyclooxygenase-2 and
prostaglandin E2 in periodontal disease. Periodontol 2000
2007: 43: 85101.
109. Nowzari H, Jorgensen MG, Ta TT, Contreras A, Slots J.
Aggressive periodontitis associated with Fanconis anemia.
A case report. J Periodontol 2001: 72: 16011606.
110. Ohtonen S, Kontturi-Narhi V, Markkanen H, Syrjanen S.
Juvenile periodontitis a clinical and radiological familial
study. J Pedod 1983: 8: 2833.
111. Onishi RM, Gaffen SL. Interleukin-17 and its target genes:
mechanisms of interleukin-17 function in disease. Immu-
nology 2010: 129: 311321.
112. Ozturk A, Vieira AR. TLR4 as a risk factor for periodontal
disease: a reappraisal. J Clin Periodontol 2009: 36: 279286.
113. Park KS, Nam JH, Choi J. The short vitamin D receptor is
associated with increased risk for generalized aggressive
periodontitis. J Clin Periodontol 2006: 33: 524528.
114. Perez HD, Kelly E, Elfman F, Armitage G, Winkler J. Defec-
tive polymorphonuclear leukocyte formyl peptide recep-
tor(s) in juvenile periodontitis. J Clin Invest 1991: 87: 971
976.
115. Pontes CC, Gonzales JR, Novaes AB Jr, Taba Junior M, Grisi
MF, Michel J, Meyle J, de Souza SL. Interleukin-4 gene
polymorphism and its relation to periodontal disease in a
Brazilian population of African heritage. J Dent 2004: 32:
241246.
116. Ramos RG, Olden K. Gene-environment interactions in
the development of complex disease phenotypes. Int J
Environ Res Public Health 2008: 5: 411.
117. Reichert S, Machulla HK, Klapproth J, Zimmermann U,
Reichert Y, Glaser CH, Schaller HG, Stein J, Schulz S. The
interleukin-10 promoter haplotype ATA is a putative risk
factor for aggressive periodontitis. J Periodontal Res 2008:
43: 4047.
118. Ren XY, Xu L, Meng HX, Zhao HS, Lu RF, Chen ZB, Feng
XH, Shi D, Zhang L, Tian Y. Family-based association anal-
ysis of S100A8 genetic polymorphisms with aggressive
periodontitis. J Periodontal Res 2009: 44: 184192.
119. Renz H, von Mutius E, Brandtzaeg P, Cookson WO,
Autenrieth IB, Haller D. Gene-environment interactions in
chronic inammatory disease. Nat Immunol 2011: 12:
273277.
120. Richter GM, Graetz C, Pohler P, Nothnagel M, Dommisch
H, Laine ML, Folwaczny M, Noack B, Eickholz P, Groess-
ner-Schreiber B, Jepsen S, Loos BG, Schreiber S, Schaefer
AS. Common genetic risk variants of TLR2 are not associ-
ated with periodontitis in large European case-control
populations. J Clin Periodontol 2012: 39: 315322.
121. Risch N, Merikangas K. The future of genetic studies of
complex human diseases. Science 1996: 273: 15161517.
122. Ryder MI. Comparison of neutrophil functions in aggres-
sive and chronic periodontitis. Periodontol 2000 2010: 53:
124137.
123. Saxn L, Nevanlinna HR. Autosomal recessive inheritance
of juvenile periodontitis: test of a hypothesis. Clin Genet
1984: 25: 332335.
124. Sax en L. Heredity of juvenile periodontitis. J Clin Period-
ontol 1980: 7: 276288.
125. Scapoli C, Borzani I, Guarnelli ME, Mamolini E, Annunzi-
ata M, Guida L, Trombelli L. IL-1 gene cluster is not linked
to aggressive periodontitis. J Dent Res 2010: 89: 457461.
126. Scapoli C, Mamolini E, Carrieri A, Guarnelli ME, Annunzi-
ata M, Guida L, Romano F, Aimetti M, Trombelli L. Gene
gene interaction among cytokine polymorphisms inu-
ence susceptibility to aggressive periodontitis. Genes Im-
mun 2011: 12: 473480.
127. Sch aefer AS, Richter GM, Nothnagel M, Manke T, Dom-
misch H, Jacobs G, Arlt A, Rosenstiel P, Noack B, Groess-
ner-Schreiber B, Jepsen S, Loos BG, Schreiber S. A
genome-wide association study identies GLT6D1 as a
susceptibility locus for periodontitis. Hum Mol Genet 2010:
19: 553562.
128. Sch afer AS, Jepsen S, Loos BG. Periodontal genetics: a dec-
ade of genetic association studies mandates better study
designs. J Clin Periodontol 2011: 38: 103107.
129. Schenkein HA, Barbour SE, Tew JG. Cytokines and inam-
matory factors regulating immunoglobulin production in
aggressive periodontitis. Periodontol 2000 2007: 45: 113
127.
130. Schenkein HA, Koertge TE, Brooks CN, Sabatini R, Purkall
DE, Tew JG. IL-17 in sera from patients with aggressive
periodontitis. J Dent Res 2010: 89: 943947.
131. Schutt C. Fighting infection: the role of lipopolysaccharide
binding proteins CD14 and LBP. Pathobiology 1999: 67:
227229.
132. Shao MY, Huang P, Cheng R, Hu T. Interleukin-6 polymor-
phisms modify the risk of periodontitis: a systematic
review and meta-analysis. J Zhejiang Univ Sci B 2009: 10:
920927.
133. Stabholz A, Soskolne WA, Shapira L. Genetic and environ-
mental risk factors for chronic periodontitis and aggressive
periodontitis. Periodontol 2000 2010: 53: 138153.
134. Sun JL, Meng HX, Cao CF, Tachi Y, Shinohara M, Ueda M,
Imai H, Ohura K. Relationship between vitamin D receptor
gene polymorphism and periodontitis. J Periodontal Res
2002: 37: 263267.
135. Sun X, Meng H, Shi D, Xu L, Zhang L, Chen Z, Feng X, Lu
R. Analysis of plasma calprotectin and polymorphisms of
S100A8 in patients with aggressive periodontitis. J Peri-
odontal Res 2011: 46: 354360.
136. Suzuki JB, Collison BC, Falkler WA Jr. Nauman RK. Immu-
nologic prole of juvenile periodontitis. II. Neutrophil
chemotaxis, phagocytosis andspore germination. J Periodontol
1984: 55: 461467.
Genetic factors in aggressive periodontitis
105
137. Takeuchi-Hatanaka K, Ohyama H, Nishimura F, Kato-Ko-
goe N, Soga Y, Matsushita S, Nakasho K, Yamanegi K, Ya-
mada N, Terada N, Takashiba S. Polymorphisms in the 5
anking region of IL12RB2 are associated with susceptibil-
ity to periodontal diseases in the Japanese population.
J Clin Periodontol 2008: 35: 317323.
138. Toomes C, James J, Wood AJ, Wu CL, McCormick D, Lench
N, Hewitt C, Moynihan L, Roberts E, Woods CG, Markham
A, Wong M, Widmer R, Ghaffar KA, Pemberton M, Hussein
IR, Temtamy SA, Davies R, Read AP, Sloan P, Dixon MJ,
Thakker NS. Loss-of-function mutations in the cathepsin
C gene result in periodontal disease and palmoplantar ker-
atosis. Nat Genet 1999: 23: 421424.
139. Tozum TF, Berker E, Akincibay H, Ozer O, Aktas D, Tezcan
I, Sekerci SC, El H, Eratalay K, Tuncbilek E. Tetraploid/dip-
loid mosaicism with generalized aggressive periodontitis.
J Periodontol 2005: 76: 15671571.
140. Van Dyke TE, Kornman KS. Inammation and factors that
may regulate inammatory response. J Periodontol 2008:
79: 15031507.
141. van Leeuwen JP, van Driel M, van den Bemd GJ, Pols HA.
Vitamin D control of osteoblast function and bone extra-
cellular matrix mineralization. Crit Rev Eukaryot Gene Expr
2001: 11: 199226.
142. Vandesteen GE, Williams BL, Ebersole JL, Altman LC, Page
RC. Clinical, microbiological and immunological studies of
a family with a high prevalence of early-onset periodonti-
tis. J Periodontol 1984: 55: 159169.
143. Vogel RI, Deasy MJ. Familial occurrence of juvenile peri-
odontitis. Ann Dent 1980: 39: 3136.
144. Wu YM, Chuang HL, Ho YP, Ho KY, Tsai CC. Investigation
of interleukin-13 gene polymorphisms in individuals with
chronic and generalized aggressive periodontitis in a
Taiwanese (Chinese) population. J Periodontal Res 2010:
45: 695701.
145. Yagi M, Kantarci A, Iwata T, Omori K, Ayilavarapu S, Ito K,
Hasturk H, Van Dyke TE. PDK1 regulates chemotaxis in
human neutrophils. J Dent Res 2009: 88: 11191124.
146. Yang IV, Wade CM, Kang HM, Alper S, Rutledge H, Lack-
ford B, Eskin E, Daly MJ, Schwartz DA. Identication of
novel genes that mediate innate immunity using inbred
mice. Genetics 2009: 183: 15351544.
147. Yu JJ, Ruddy MJ, Wong GC, Sntescu C, Baker PJ, Smith
JB, Evans RT, Gaffen SL. An essential role for IL-17 in pre-
venting pathogen-initiated bone destruction: recruitment
of neutrophils to inamed bone requires IL-17 receptor-
dependent signals. Blood 2007: 109: 37943802.
148. Yu JJ, Gaffen SL. Interleukin-17: a novel inammatory
cytokine that bridges innate and adaptive immunity. Front
Biosci 2008: 13: 170177.
149. Zanoni I, Ostuni R, Marek LR, Barresi S, Barbalat R, Bar-
ton GM, Granucci F, Kagan JC. CD14 controls the LPS-
induced endocytosis of Toll-like receptor 4. Cell 2011:
147: 868880.
150. Zhang Y, Syed R, Uygar C, Pallos D, Gorry MC, Firatli E,
Cortelli JR, VanDyke TE, Hart PS, Feingold E, Hart TC.
Evaluation of human leukocyte N-formylpeptide receptor
(FPR1) SNPs in aggressive periodontitis patients. Genes
Immun 2003: 4: 2229.
151. Zhu G, Li C, Cao Z, Corbet EF, Jin L. Toll-like receptors 2
and 4 gene polymorphisms in a Chinese population with
periodontitis. Quintessence Int 2008: 39: 217226.
152. Zhu XL, Meng HX, Xu L, Zhang L, Chen ZB, Shi D, Feng
XH. Combined association of CCR2-V64I and MCP-1-
2518A/G polymorphisms with generalised aggressive peri-
odontitis in Chinese. Chin J Dent Res 2010: 13: 109114.
Vieira & Albandar
106
Das könnte Ihnen auch gefallen
- SM1 3Dokument15 SeitenSM1 3Smitha Kapani gowdaNoch keine Bewertungen
- SM1 3Dokument15 SeitenSM1 3Smitha Kapani gowdaNoch keine Bewertungen
- SM1 3Dokument15 SeitenSM1 3Smitha Kapani gowdaNoch keine Bewertungen
- SM 4Dokument12 SeitenSM 4Smitha Kapani gowdaNoch keine Bewertungen
- Maternal Periodontitis and Risk of Preterm Low Birth Weight Infants-Case Control Study Inindian PopulationDokument9 SeitenMaternal Periodontitis and Risk of Preterm Low Birth Weight Infants-Case Control Study Inindian PopulationSmitha Kapani gowdaNoch keine Bewertungen
- SM1 3Dokument15 SeitenSM1 3Smitha Kapani gowdaNoch keine Bewertungen
- SM1 3Dokument15 SeitenSM1 3Smitha Kapani gowdaNoch keine Bewertungen
- SM 32Dokument33 SeitenSM 32Smitha Kapani gowdaNoch keine Bewertungen
- SM 5Dokument13 SeitenSM 5Smitha Kapani gowdaNoch keine Bewertungen
- Cap 2012 110026 PDFDokument8 SeitenCap 2012 110026 PDFSmitha Kapani gowdaNoch keine Bewertungen
- Classification of P - PRP To L - PRFDokument10 SeitenClassification of P - PRP To L - PRFSmitha Kapani gowdaNoch keine Bewertungen
- Periodontology 2000, 56 TH VolumeDokument11 SeitenPeriodontology 2000, 56 TH VolumeSmitha Kapani gowdaNoch keine Bewertungen
- Eula Microsoft Visual StudioDokument3 SeitenEula Microsoft Visual StudioqwwerttyyNoch keine Bewertungen
- Periodontal Literature ReviewDokument70 SeitenPeriodontal Literature ReviewSmitha Kapani gowdaNoch keine Bewertungen
- Health Research MethodologyDokument245 SeitenHealth Research MethodologyApollo Institute of Hospital Administration100% (1)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- No Nanda Diagnosis (ICD X) (BUKU) Nanda Code Sequence NoDokument132 SeitenNo Nanda Diagnosis (ICD X) (BUKU) Nanda Code Sequence NonataliaNoch keine Bewertungen
- School Health Services (3126135)Dokument129 SeitenSchool Health Services (3126135)Prabhjeet100% (2)
- Bds SyllabusDokument67 SeitenBds Syllabusabdulbasitejaz100% (2)
- Epidemiology Lecture NotesDokument178 SeitenEpidemiology Lecture NotesImtiaz Husain83% (6)
- TB LAM Training MaterialsDokument24 SeitenTB LAM Training MaterialsBenedict OkotNoch keine Bewertungen
- Flow Chart Showng Evalution in Community Medicine: Mbbs Third ProfessionalDokument9 SeitenFlow Chart Showng Evalution in Community Medicine: Mbbs Third ProfessionalusamaNoch keine Bewertungen
- Handouts CD Prof. RojasDokument6 SeitenHandouts CD Prof. RojasChallen CulturaNoch keine Bewertungen
- HE Lesson Plan (Diseases - Vaccines)Dokument7 SeitenHE Lesson Plan (Diseases - Vaccines)Ky HydeNoch keine Bewertungen
- Disease Transmission DynamicsDokument30 SeitenDisease Transmission DynamicsSyed Sanan shahNoch keine Bewertungen
- Worksheet - Formal & Informal Definition - Remedial ClassDokument1 SeiteWorksheet - Formal & Informal Definition - Remedial ClassEvelyn CanoneraNoch keine Bewertungen
- Endodontics in Systemically Compromised PatientsDokument30 SeitenEndodontics in Systemically Compromised Patientscarolina pavezNoch keine Bewertungen
- Numerical Solution of SIR Model For Transmission oDokument9 SeitenNumerical Solution of SIR Model For Transmission oYoussef YousryNoch keine Bewertungen
- Community Health Nursing Doh Related Programs: Epi - Types of VaccinesDokument32 SeitenCommunity Health Nursing Doh Related Programs: Epi - Types of VaccinesAngelaNoch keine Bewertungen
- Ozone TherapyDokument42 SeitenOzone Therapyonyak100% (1)
- Klinoski Rachael L 200709 MSCDokument128 SeitenKlinoski Rachael L 200709 MSCDrashua AshuaNoch keine Bewertungen
- Unit 2 Final DraftDokument2 SeitenUnit 2 Final Draftapi-252269185Noch keine Bewertungen
- CDC 5435DS1 PDFDokument211 SeitenCDC 5435DS1 PDFbodeadumitru9261Noch keine Bewertungen
- 5 FOI Webpage Jan 4 2022Dokument119 Seiten5 FOI Webpage Jan 4 2022Luis ricardo Véjar felixNoch keine Bewertungen
- CHN ReviewerDokument36 SeitenCHN ReviewerRezideh75% (4)
- Viii. Nursing Care Plan: Asessment Diagnosis Planning Intervention Rationale EvaluationDokument3 SeitenViii. Nursing Care Plan: Asessment Diagnosis Planning Intervention Rationale Evaluationhehehe29Noch keine Bewertungen
- Parental Opinions and Attitudes About Children's Vaccination Safety in Silesian Voivodeship, PolandDokument8 SeitenParental Opinions and Attitudes About Children's Vaccination Safety in Silesian Voivodeship, PolandkrishnasreeNoch keine Bewertungen
- Systemic MycosisDokument15 SeitenSystemic Mycosisapi-19969058Noch keine Bewertungen
- DOT Transporting Infectious SubstancesDokument48 SeitenDOT Transporting Infectious SubstancesPremiumJust4U Admin v111222336677228888Noch keine Bewertungen
- Medical Importance BacteriaDokument11 SeitenMedical Importance BacteriaveeramaniNoch keine Bewertungen
- Protective Clothing: Standard Terminology Relating ToDokument9 SeitenProtective Clothing: Standard Terminology Relating ToSuryateja MerguNoch keine Bewertungen
- Abstracts For 32nd Congrass of ZoologyDokument350 SeitenAbstracts For 32nd Congrass of ZoologySaima WaseemNoch keine Bewertungen
- Sirwan Ali Enterohemorrhagic-Escherichia-coliDokument8 SeitenSirwan Ali Enterohemorrhagic-Escherichia-coliDlzar AbubakrNoch keine Bewertungen
- Online Test SyllabusDokument8 SeitenOnline Test SyllabusSHRIKANTNoch keine Bewertungen
- Tools and Techniques For Severe Acute Respiratory Syndrome Coronavirus 2 (Sars-Cov-2) /covid-19 DetectionDokument63 SeitenTools and Techniques For Severe Acute Respiratory Syndrome Coronavirus 2 (Sars-Cov-2) /covid-19 DetectionEdo RezaprasgaNoch keine Bewertungen
- ATB Oral Vs EV en Infecciones de Articulaciones y OseasDokument12 SeitenATB Oral Vs EV en Infecciones de Articulaciones y OseasSMIBA MedicinaNoch keine Bewertungen