Das könnte Ihnen auch gefallen
- P1 Chp12 DifferentiationDokument56 SeitenP1 Chp12 DifferentiationbobNoch keine Bewertungen
- Parts Manual: Generator SetDokument118 SeitenParts Manual: Generator SetAhmed Kamal100% (2)
- Chapter 24 - The Solar SystemDokument36 SeitenChapter 24 - The Solar SystemHeather Blackwell100% (1)
- Neurofibroma, Schwannoma or A Hybrid Tumor of The Peripheral Nerve Sheath?Dokument4 SeitenNeurofibroma, Schwannoma or A Hybrid Tumor of The Peripheral Nerve Sheath?As AsNoch keine Bewertungen
- Primary Intracranial Leiomyoma: A Case Report and Literature ReviewDokument3 SeitenPrimary Intracranial Leiomyoma: A Case Report and Literature ReviewcandiddreamsNoch keine Bewertungen
- Pigmented Neurofibroma of The SkinDokument6 SeitenPigmented Neurofibroma of The SkinDeba P SarmaNoch keine Bewertungen
- 1009 Case 2Dokument4 Seiten1009 Case 2willygopeNoch keine Bewertungen
- E - Uniform Round Tumour Cells With Small Nucleus and Clear Vacuolated CytoplasmDokument16 SeitenE - Uniform Round Tumour Cells With Small Nucleus and Clear Vacuolated CytoplasmAien LeeNoch keine Bewertungen
- Oligodendroglioma in The Cervical Spinal Cord of A Dog: T. M, A. M - L, M. H - T, W. BDokument3 SeitenOligodendroglioma in The Cervical Spinal Cord of A Dog: T. M, A. M - L, M. H - T, W. BSamir BazanNoch keine Bewertungen
- Malignant Myopericytoma: Report of A New Case and Review of The LiteratureDokument6 SeitenMalignant Myopericytoma: Report of A New Case and Review of The LiteratureRachel AutranNoch keine Bewertungen
- M 35, Left Upper Eyelid Nodule: Deba P Sarma, MD OmahaDokument4 SeitenM 35, Left Upper Eyelid Nodule: Deba P Sarma, MD OmahaDeba P SarmaNoch keine Bewertungen
- Vol-1, Issue-1 Prospective Study of Peripheral Nerve Tumors Over A Period of 2 YearsDokument4 SeitenVol-1, Issue-1 Prospective Study of Peripheral Nerve Tumors Over A Period of 2 YearsijhrmimsNoch keine Bewertungen
- Pilo Matri Coma PosterDokument1 SeitePilo Matri Coma Posterkjv5gxdw4fNoch keine Bewertungen
- Segmental Neurofibromatosis: Report of A Rare EntityDokument3 SeitenSegmental Neurofibromatosis: Report of A Rare EntityDwi Wahyu AprianiNoch keine Bewertungen
- Case Report 2022Dokument5 SeitenCase Report 2022Reyes Ivan García CuevasNoch keine Bewertungen
- 5 5 5 Pontine Atypical Neurocytoma Case Report 副本Dokument8 Seiten5 5 5 Pontine Atypical Neurocytoma Case Report 副本singhNoch keine Bewertungen
- Case Report MM 33 Years Old MaleDokument4 SeitenCase Report MM 33 Years Old MalealicemelsNoch keine Bewertungen
- Follicular Carcinoma of Thyroid Presenting As Brain MetastasisDokument3 SeitenFollicular Carcinoma of Thyroid Presenting As Brain MetastasisArif Susilo RahadiNoch keine Bewertungen
- Desmoplastic MelanomaDokument3 SeitenDesmoplastic MelanomamakhanmdNoch keine Bewertungen
- Herlina Eka ShintaDokument1 SeiteHerlina Eka ShintaBayu SetiaNoch keine Bewertungen
- Cerebellopontine Angle Epidermoid CYST: Case ReportDokument3 SeitenCerebellopontine Angle Epidermoid CYST: Case ReportTamajyoti GhoshNoch keine Bewertungen
- Multiple Dermatofibromas in An Adult FemaleDokument3 SeitenMultiple Dermatofibromas in An Adult FemaleDeba P SarmaNoch keine Bewertungen
- DR SARMA'S DERMPATH: Chondroma Cutis, The Internet Journal of Dermatology 2007: Volume 6 NumberDokument3 SeitenDR SARMA'S DERMPATH: Chondroma Cutis, The Internet Journal of Dermatology 2007: Volume 6 NumberDeba P SarmaNoch keine Bewertungen
- EN + EosinofiliaDokument3 SeitenEN + EosinofiliaAna Flavia BaptistaNoch keine Bewertungen
- The Hair Follicle Barrier To Involvement by Malignant MelanomaDokument9 SeitenThe Hair Follicle Barrier To Involvement by Malignant MelanomaSaifuddin HaswareNoch keine Bewertungen
- M: Elaine Crystine Vieira de Paiva Rua Pedro I, 1.033 Centro 60035-101 - Fortaleza - CE - BrazilDokument2 SeitenM: Elaine Crystine Vieira de Paiva Rua Pedro I, 1.033 Centro 60035-101 - Fortaleza - CE - Brazilpruebaprueba321765Noch keine Bewertungen
- tmpEDB0 TMPDokument5 SeitentmpEDB0 TMPFrontiersNoch keine Bewertungen
- Laryngeal Plasmacytoma in Kahlers Disease: A Case ReportDokument6 SeitenLaryngeal Plasmacytoma in Kahlers Disease: A Case ReportIJAR JOURNALNoch keine Bewertungen
- Pleomorphic Sarcoma in Paratesticular Region: Case Report Open AccessDokument5 SeitenPleomorphic Sarcoma in Paratesticular Region: Case Report Open AccessNurulDiniaPutriNoch keine Bewertungen
- 2005-Pigmentary Mosaicism and MosaicDokument2 Seiten2005-Pigmentary Mosaicism and MosaicANoch keine Bewertungen
- Mekanisme PDFDokument9 SeitenMekanisme PDFAndyk Strapilococus AureusNoch keine Bewertungen
- Forefoot Myopericytoma: A Case Reportand Review of The LiteratureDokument4 SeitenForefoot Myopericytoma: A Case Reportand Review of The LiteratureIJAR JOURNALNoch keine Bewertungen
- Colreavy 2000Dokument6 SeitenColreavy 2000Yi-Hung SungNoch keine Bewertungen
- Komatsu 2020Dokument5 SeitenKomatsu 2020Felipe RohamNoch keine Bewertungen
- Case Report Reference Article (Published)Dokument3 SeitenCase Report Reference Article (Published)manojananthappanNoch keine Bewertungen
- Pathophysiology of Meningiomas 2003Dokument18 SeitenPathophysiology of Meningiomas 2003Klinik medan DeliNoch keine Bewertungen
- Bpa 12504Dokument31 SeitenBpa 12504Sergeat18BNoch keine Bewertungen
- Jkms 20 687 PDFDokument4 SeitenJkms 20 687 PDFDamodara KumaranNoch keine Bewertungen
- Keywords: Pilomatrixoma, Skin Nodule, Fine Needle Aspiration CytologyDokument4 SeitenKeywords: Pilomatrixoma, Skin Nodule, Fine Needle Aspiration CytologyachmadaNoch keine Bewertungen
- Complex Adnexal TumorDokument2 SeitenComplex Adnexal TumorFaduahSalazarNoch keine Bewertungen
- Miller DiekerDokument8 SeitenMiller DiekerJucsy JuxyNoch keine Bewertungen
- Cerebellar Hemangioblastoma-A Rare EntityDokument10 SeitenCerebellar Hemangioblastoma-A Rare EntityJay LeheriNoch keine Bewertungen
- 0046 8177 (93) 90013 7Dokument12 Seiten0046 8177 (93) 90013 7Carmen Gomez MuñozNoch keine Bewertungen
- Buka Folder JURNALDokument11 SeitenBuka Folder JURNAL57z8crwcfjNoch keine Bewertungen
- Endolymphatic Sac TumorDokument2 SeitenEndolymphatic Sac TumorMads TandocNoch keine Bewertungen
- Neurocytoma/rhabdomyoma (Myoneurocytoma) of The CerebellumDokument6 SeitenNeurocytoma/rhabdomyoma (Myoneurocytoma) of The CerebellumRafael Mujica OreNoch keine Bewertungen
- Abstract: Kimura Disease Is A Rare Form of Chronic Inflammatory Disorder InvolvingDokument4 SeitenAbstract: Kimura Disease Is A Rare Form of Chronic Inflammatory Disorder InvolvingpriyokNoch keine Bewertungen
- Articulo de Serie de CasoDokument8 SeitenArticulo de Serie de CasoJairo Lino BNoch keine Bewertungen
- Small Round Cells of Head and NeckDokument10 SeitenSmall Round Cells of Head and NeckBlazxy EyreNoch keine Bewertungen
- Cancer-5 (HSS 2305) - F2022Dokument10 SeitenCancer-5 (HSS 2305) - F2022zahra.lalani14Noch keine Bewertungen
- Epithelioid Hemangioendothelioma of The Infundibular-Hypothalamic Region: Case Report and Literature ReviewDokument6 SeitenEpithelioid Hemangioendothelioma of The Infundibular-Hypothalamic Region: Case Report and Literature ReviewcarlosNoch keine Bewertungen
- NeuroblastomaDokument19 SeitenNeuroblastomaTri Andhika Dessy WahyuniNoch keine Bewertungen
- Desdierencia Entre TFS y Glandula ParotidaDokument7 SeitenDesdierencia Entre TFS y Glandula ParotidaReyes Ivan García CuevasNoch keine Bewertungen
- 1208 Case 2Dokument4 Seiten1208 Case 2willygopeNoch keine Bewertungen
- Myxofibrosarcoma: Christina L. Roland,, Wei-Lien Wang,, Alexander J. Lazar,, Keila E. TorresDokument14 SeitenMyxofibrosarcoma: Christina L. Roland,, Wei-Lien Wang,, Alexander J. Lazar,, Keila E. TorresMarina GorelikNoch keine Bewertungen
- Net Cu Meta in HipofizaDokument6 SeitenNet Cu Meta in HipofizaLaura PredescuNoch keine Bewertungen
- RPB14150079015Dokument5 SeitenRPB14150079015Ijupbs IjupbsNoch keine Bewertungen
- Brain Immunology and Immunotherapy in Brain TumoursDokument14 SeitenBrain Immunology and Immunotherapy in Brain TumoursAnonymous QLadTClydkNoch keine Bewertungen
- Spindle Cell Lipoma: Franz Enzinger, A. HarveyDokument8 SeitenSpindle Cell Lipoma: Franz Enzinger, A. HarveyAdjhy Aji AchmadNoch keine Bewertungen
- BreastDokument3 SeitenBreastcandiddreamsNoch keine Bewertungen
- LP Brain TumorDokument20 SeitenLP Brain TumorMuhammad PanduNoch keine Bewertungen
- Neuroendocrine Tumors: Surgical Evaluation and ManagementVon EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNoch keine Bewertungen
- Accessory TragusDokument3 SeitenAccessory TragusDeba P SarmaNoch keine Bewertungen
- Acantholytic Solar Keratosis, M 67, Forehead PDFDokument6 SeitenAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNoch keine Bewertungen
- Pilar Cyst With CrystalsDokument2 SeitenPilar Cyst With CrystalsDeba P SarmaNoch keine Bewertungen
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Dokument3 SeitenAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNoch keine Bewertungen
- Acantholytic Actinic KeratosisDokument4 SeitenAcantholytic Actinic KeratosisDeba P SarmaNoch keine Bewertungen
- Acantholytic Dermatosis With DyskeratosisDokument11 SeitenAcantholytic Dermatosis With DyskeratosisDeba P SarmaNoch keine Bewertungen
- Acantholytic Bullous DiseaseDokument4 SeitenAcantholytic Bullous DiseaseDeba P SarmaNoch keine Bewertungen
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDokument7 SeitenXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNoch keine Bewertungen
- Acantholytic Acanthoma. M 60, ScrotumDokument8 SeitenAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNoch keine Bewertungen
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Dokument6 SeitenBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNoch keine Bewertungen
- Xanthogranuloma, M 30, Right ElbowDokument4 SeitenXanthogranuloma, M 30, Right ElbowDeba P SarmaNoch keine Bewertungen
- Results of Search in Google Scholar On 'Deba P Sarma'Dokument28 SeitenResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNoch keine Bewertungen
- Xanthogranuloma PPT DSDokument9 SeitenXanthogranuloma PPT DSDeba P SarmaNoch keine Bewertungen
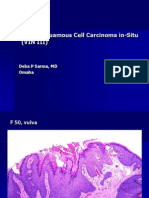
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDokument6 SeitenVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNoch keine Bewertungen
- Verrucous Carcinoma of The Foot, M 63, Left FootDokument8 SeitenVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
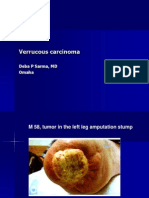
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDokument7 SeitenVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNoch keine Bewertungen
- Verrucous Epidermal Nevus. F 43, ScalpDokument4 SeitenVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNoch keine Bewertungen
- Verruca Vulgaris., M 22.,PPTDokument2 SeitenVerruca Vulgaris., M 22.,PPTDeba P SarmaNoch keine Bewertungen
- Junos ErrorsDokument2 SeitenJunos ErrorsrashidsharafatNoch keine Bewertungen
- FKTDokument32 SeitenFKTNeeraj SharmaNoch keine Bewertungen
- VLSI Implementation of Floating Point AdderDokument46 SeitenVLSI Implementation of Floating Point AdderParamesh Waran100% (1)
- LSL Education Center Final Exam 30 Minutes Full Name - Phone NumberDokument2 SeitenLSL Education Center Final Exam 30 Minutes Full Name - Phone NumberDilzoda Boytumanova.Noch keine Bewertungen
- Windows System Shortcut CommandsDokument2 SeitenWindows System Shortcut CommandsVenkatesh YerraNoch keine Bewertungen
- Inspection Report For Apartment Building at 1080 93rd St. in Bay Harbor IslandsDokument13 SeitenInspection Report For Apartment Building at 1080 93rd St. in Bay Harbor IslandsAmanda RojasNoch keine Bewertungen
- Zigbee Technology:19-3-2010: Seminor Title DateDokument21 SeitenZigbee Technology:19-3-2010: Seminor Title Dateitdep_gpcet7225Noch keine Bewertungen
- PNGRB - Electrical Safety Audit ChecklistDokument4 SeitenPNGRB - Electrical Safety Audit ChecklistKritarth SrivastavNoch keine Bewertungen
- Phy Mock SolDokument17 SeitenPhy Mock SolA PersonNoch keine Bewertungen
- Sample Interview Questions For Planning EngineersDokument16 SeitenSample Interview Questions For Planning EngineersPooja PawarNoch keine Bewertungen
- 2001 Ford F150 ManualDokument296 Seiten2001 Ford F150 Manualerjenkins1100% (2)
- Bin Adam Group of CompaniesDokument8 SeitenBin Adam Group of CompaniesSheema AhmadNoch keine Bewertungen
- Exam First Grading 2nd Semester - ReadingDokument3 SeitenExam First Grading 2nd Semester - ReadingArleneRamosNoch keine Bewertungen
- April 2021 BDA Case Study - GroupDokument4 SeitenApril 2021 BDA Case Study - GroupTinashe Chirume1Noch keine Bewertungen
- Guidelines For Plenipotentiary - 1Dokument6 SeitenGuidelines For Plenipotentiary - 1Oladimeji Ibukun IjaodolaNoch keine Bewertungen
- Fluoride - Wide Range of Serious Health Problems"Dokument29 SeitenFluoride - Wide Range of Serious Health Problems"zataullah100% (2)
- Weg CFW500 Enc PDFDokument32 SeitenWeg CFW500 Enc PDFFabio Pedroso de Morais100% (1)
- Catalogue of Archaeological Finds FromDokument67 SeitenCatalogue of Archaeological Finds FromAdrinaNoch keine Bewertungen
- Community Resource MobilizationDokument17 SeitenCommunity Resource Mobilizationerikka june forosueloNoch keine Bewertungen
- ProbDokument10 SeitenProbKashif JawaidNoch keine Bewertungen
- Reference by John BatchelorDokument1 SeiteReference by John Batchelorapi-276994844Noch keine Bewertungen
- Design Practical Eden Swithenbank Graded PeDokument7 SeitenDesign Practical Eden Swithenbank Graded Peapi-429329398Noch keine Bewertungen
- R15 Understanding Business CyclesDokument33 SeitenR15 Understanding Business CyclesUmar FarooqNoch keine Bewertungen
- DevOps Reference CardDokument2 SeitenDevOps Reference CardIntizarchauhanNoch keine Bewertungen
- Navi-Planner User ManualDokument331 SeitenNavi-Planner User ManualRichard KershawNoch keine Bewertungen
- MQXUSBDEVAPIDokument32 SeitenMQXUSBDEVAPIwonderxNoch keine Bewertungen
- Negative Feedback AmplifierDokument31 SeitenNegative Feedback AmplifierPepNoch keine Bewertungen