Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Proofreading: Basic Guide (Research)Dokument34 SeitenProofreading: Basic Guide (Research)Mary Christelle100% (1)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Agne Vs Director of LandsDokument7 SeitenAgne Vs Director of LandsLee SomarNoch keine Bewertungen
- Learning Module 4 - BARTENDINGDokument34 SeitenLearning Module 4 - BARTENDINGivy mae flores67% (3)
- The Magical Diaries of Ethel ArcherDokument7 SeitenThe Magical Diaries of Ethel Archerleeghancock100% (1)
- Libi Vs IACDokument1 SeiteLibi Vs IACBingoheartNoch keine Bewertungen
- Peter Zumthor - Thinking Architecture PDFDokument33 SeitenPeter Zumthor - Thinking Architecture PDFDiana Sterian73% (11)
- Demand, Elasticity of Demand and Demand ForecastingDokument16 SeitenDemand, Elasticity of Demand and Demand Forecastingankit thapliyal100% (1)
- Lesson Plan 4Dokument6 SeitenLesson Plan 4Lilay Barambangan100% (3)
- NMC CBT Sample Q&a Part 3 AcDokument14 SeitenNMC CBT Sample Q&a Part 3 AcJoane FranciscoNoch keine Bewertungen
- Pilar Cyst With CrystalsDokument2 SeitenPilar Cyst With CrystalsDeba P SarmaNoch keine Bewertungen
- Acantholytic Solar Keratosis, M 67, Forehead PDFDokument6 SeitenAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNoch keine Bewertungen
- Acantholytic Dermatosis With DyskeratosisDokument11 SeitenAcantholytic Dermatosis With DyskeratosisDeba P SarmaNoch keine Bewertungen
- Accessory TragusDokument3 SeitenAccessory TragusDeba P SarmaNoch keine Bewertungen
- Acantholytic Bullous DiseaseDokument4 SeitenAcantholytic Bullous DiseaseDeba P SarmaNoch keine Bewertungen
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Dokument3 SeitenAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNoch keine Bewertungen
- Acantholytic Actinic KeratosisDokument4 SeitenAcantholytic Actinic KeratosisDeba P SarmaNoch keine Bewertungen
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDokument7 SeitenXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNoch keine Bewertungen
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Dokument6 SeitenBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNoch keine Bewertungen
- Results of Search in Google Scholar On 'Deba P Sarma'Dokument28 SeitenResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNoch keine Bewertungen
- Verrucous Carcinoma of The Foot, M 63, Left FootDokument8 SeitenVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Acantholytic Acanthoma. M 60, ScrotumDokument8 SeitenAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNoch keine Bewertungen
- Xanthogranuloma, M 30, Right ElbowDokument4 SeitenXanthogranuloma, M 30, Right ElbowDeba P SarmaNoch keine Bewertungen
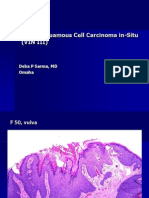
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDokument6 SeitenVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNoch keine Bewertungen
- Xanthogranuloma PPT DSDokument9 SeitenXanthogranuloma PPT DSDeba P SarmaNoch keine Bewertungen
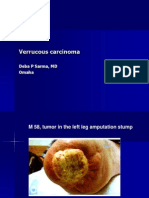
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDokument7 SeitenVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNoch keine Bewertungen
- Verrucous Epidermal Nevus. F 43, ScalpDokument4 SeitenVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNoch keine Bewertungen
- Verruca Vulgaris., M 22.,PPTDokument2 SeitenVerruca Vulgaris., M 22.,PPTDeba P SarmaNoch keine Bewertungen
- Cry, The Beloved CountryDokument36 SeitenCry, The Beloved CountryMariela RomeroNoch keine Bewertungen
- A Feasibility/Project Study OnDokument14 SeitenA Feasibility/Project Study OnWilson Domingo LazarteNoch keine Bewertungen
- DSC User GuidelinesDokument64 SeitenDSC User Guidelineslinus200Noch keine Bewertungen
- Agmt - Spa Schedule HDokument20 SeitenAgmt - Spa Schedule Hapi-340431954Noch keine Bewertungen
- Clause: Extra Element + Independent Clause Dependent ClauseDokument1 SeiteClause: Extra Element + Independent Clause Dependent ClauseTieng HuangNoch keine Bewertungen
- OCTOBER 2016: Nur Amira Nadia Binti Azizi 2018404898 BA1185FDokument4 SeitenOCTOBER 2016: Nur Amira Nadia Binti Azizi 2018404898 BA1185FNur Amira NadiaNoch keine Bewertungen
- Content Kartilya NG Katipunan: Kataastaasan, Kagalanggalangang Katipunan NG Mga Anak NG Bayan)Dokument6 SeitenContent Kartilya NG Katipunan: Kataastaasan, Kagalanggalangang Katipunan NG Mga Anak NG Bayan)AngelaNoch keine Bewertungen
- Contractions 29.01Dokument1 SeiteContractions 29.01Katita la OriginalNoch keine Bewertungen
- A Crude Awakening Video NotesDokument3 SeitenA Crude Awakening Video NotesTai NguyenNoch keine Bewertungen
- STAS 111 - Information AgeDokument20 SeitenSTAS 111 - Information AgeMayeee GayosoNoch keine Bewertungen
- 1.4 Creating Graphic OrganizerDokument1 Seite1.4 Creating Graphic OrganizerTrixie Roselle Y. MesiasNoch keine Bewertungen
- Antibullying Presentation 1Dokument23 SeitenAntibullying Presentation 1Martin Ceazar HermocillaNoch keine Bewertungen
- Catalogue Mega EnglishDokument40 SeitenCatalogue Mega EnglishInotech Outillage Nouvelle CalédonieNoch keine Bewertungen
- Sticker BookDokument66 SeitenSticker BookIvan SutlovicNoch keine Bewertungen
- Police OrgDokument70 SeitenPolice OrgSeagal UmarNoch keine Bewertungen
- Chapter 3 ContDokument12 SeitenChapter 3 ContVenus Frias-AntonioNoch keine Bewertungen
- Irm PDFDokument27 SeitenIrm PDFerraticNoch keine Bewertungen
- Reflection PseudoscienceDokument3 SeitenReflection PseudoscienceSuganthi RamasamyNoch keine Bewertungen
- October 2014 1413376166 06 PDFDokument3 SeitenOctober 2014 1413376166 06 PDFDineshNoch keine Bewertungen
- AtharvasheershamDokument5 SeitenAtharvasheershamforthegroupsNoch keine Bewertungen
- Detailed Lesson Plan in HousekeepingDokument6 SeitenDetailed Lesson Plan in HousekeepingreyNoch keine Bewertungen