Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Pilar Cyst With CrystalsDokument2 SeitenPilar Cyst With CrystalsDeba P SarmaNoch keine Bewertungen
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Dokument3 SeitenAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNoch keine Bewertungen
- Accessory TragusDokument3 SeitenAccessory TragusDeba P SarmaNoch keine Bewertungen
- Acantholytic Dermatosis With DyskeratosisDokument11 SeitenAcantholytic Dermatosis With DyskeratosisDeba P SarmaNoch keine Bewertungen
- Acantholytic Solar Keratosis, M 67, Forehead PDFDokument6 SeitenAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNoch keine Bewertungen
- Results of Search in Google Scholar On 'Deba P Sarma'Dokument28 SeitenResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNoch keine Bewertungen
- Acantholytic Actinic KeratosisDokument4 SeitenAcantholytic Actinic KeratosisDeba P SarmaNoch keine Bewertungen
- Acantholytic Bullous DiseaseDokument4 SeitenAcantholytic Bullous DiseaseDeba P SarmaNoch keine Bewertungen
- Acantholytic Acanthoma. M 60, ScrotumDokument8 SeitenAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNoch keine Bewertungen
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Dokument6 SeitenBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNoch keine Bewertungen
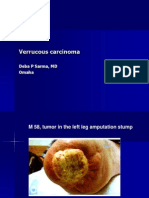
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDokument7 SeitenVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNoch keine Bewertungen
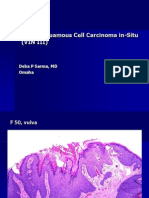
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDokument6 SeitenVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNoch keine Bewertungen
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDokument7 SeitenXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNoch keine Bewertungen
- Xanthogranuloma, M 30, Right ElbowDokument4 SeitenXanthogranuloma, M 30, Right ElbowDeba P SarmaNoch keine Bewertungen
- Verrucous Epidermal Nevus. F 43, ScalpDokument4 SeitenVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNoch keine Bewertungen
- Xanthogranuloma PPT DSDokument9 SeitenXanthogranuloma PPT DSDeba P SarmaNoch keine Bewertungen
- Verrucous Carcinoma of The Foot, M 63, Left FootDokument8 SeitenVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Verruca Vulgaris., M 22.,PPTDokument2 SeitenVerruca Vulgaris., M 22.,PPTDeba P SarmaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Load Distribution Flow Chart For Bridge DesignDokument1 SeiteLoad Distribution Flow Chart For Bridge DesignBunkun15Noch keine Bewertungen
- Bsi MD Ivdr Conformity Assessment Routes Booklet Uk enDokument15 SeitenBsi MD Ivdr Conformity Assessment Routes Booklet Uk enGuillaumeNoch keine Bewertungen
- E Numbers Are Number Codes ForDokument3 SeitenE Numbers Are Number Codes ForaradhyaNoch keine Bewertungen
- Pelton2014 Para-Equilibrium Phase DiagramsDokument7 SeitenPelton2014 Para-Equilibrium Phase DiagramsAbraham Becerra AranedaNoch keine Bewertungen
- Dwnload Full Psychology Core Concepts 7th Edition Zimbardo Test Bank PDFDokument13 SeitenDwnload Full Psychology Core Concepts 7th Edition Zimbardo Test Bank PDFcomfortdehm1350100% (7)
- Campa Cola - WikipediaDokument10 SeitenCampa Cola - WikipediaPradeep KumarNoch keine Bewertungen
- Wet Chemical Pre E PresentationDokument310 SeitenWet Chemical Pre E PresentationEdwardAlexanderGarciaNoch keine Bewertungen
- Onitsuka Tiger PDFDokument67 SeitenOnitsuka Tiger PDFAhmad Bilal MawardiNoch keine Bewertungen
- UntitledDokument413 SeitenUntitledjgj38j90Noch keine Bewertungen
- Aesa Based Pechay Production - AbdulwahidDokument17 SeitenAesa Based Pechay Production - AbdulwahidAnne Xx100% (1)
- Thermobaric Effects Formed by Aluminum Foils Enveloping Cylindrical ChargesDokument10 SeitenThermobaric Effects Formed by Aluminum Foils Enveloping Cylindrical ChargesAnonymous QFUEsUAnNoch keine Bewertungen
- Pediatric Gynecology BaruDokument79 SeitenPediatric Gynecology BaruJosephine Irena100% (2)
- HACH LANGE Amino Acid F Reagent Powder (2353255)Dokument6 SeitenHACH LANGE Amino Acid F Reagent Powder (2353255)kerem__22Noch keine Bewertungen
- DLL - Mapeh 6 - Q2 - W8Dokument6 SeitenDLL - Mapeh 6 - Q2 - W8Joe Marie FloresNoch keine Bewertungen
- A Collection of Ideas For The Chemistry Classroom by Jeff HepburnDokument14 SeitenA Collection of Ideas For The Chemistry Classroom by Jeff HepburnPaul SchumannNoch keine Bewertungen
- North Central Mindanao College: Maranding, Lala, Lanao Del NorteDokument8 SeitenNorth Central Mindanao College: Maranding, Lala, Lanao Del NorteAnalyn FielNoch keine Bewertungen
- T 1246784488 17108574 Street Lighting Control Based On LonWorks Power Line CommunicationDokument3 SeitenT 1246784488 17108574 Street Lighting Control Based On LonWorks Power Line CommunicationsryogaaNoch keine Bewertungen
- CFD Analysis of Flow Through Compressor CascadeDokument10 SeitenCFD Analysis of Flow Through Compressor CascadeKhalid KhalilNoch keine Bewertungen
- BRASS Introduction 2012Dokument23 SeitenBRASS Introduction 20121234scr5678Noch keine Bewertungen
- South Valley University Faculty of Science Geology Department Dr. Mohamed Youssef AliDokument29 SeitenSouth Valley University Faculty of Science Geology Department Dr. Mohamed Youssef AliHari Dante Cry100% (1)
- 114 The Letter S: M 'TafontDokument9 Seiten114 The Letter S: M 'TafontHarry TLNoch keine Bewertungen
- Module 02 Connect Hardware Peripherals EndaleDokument49 SeitenModule 02 Connect Hardware Peripherals EndaleSoli Mondo100% (1)
- Knowledge /28 Application / 22 Thinking / 12 Communication / 9Dokument8 SeitenKnowledge /28 Application / 22 Thinking / 12 Communication / 9NmNoch keine Bewertungen
- Etl 213-1208.10 enDokument1 SeiteEtl 213-1208.10 enhossamNoch keine Bewertungen
- Psalm151 160Dokument3 SeitenPsalm151 160Gina KristenNoch keine Bewertungen
- Nema MG10 PDFDokument27 SeitenNema MG10 PDFManuel Antonio Santos VargasNoch keine Bewertungen
- Sikagrout®-214 Ae: Product Data SheetDokument3 SeitenSikagrout®-214 Ae: Product Data Sheetmohammed rinshinNoch keine Bewertungen
- ForewordDokument96 SeitenForewordkkcmNoch keine Bewertungen
- 4th Semester Electrical Engg.Dokument19 Seiten4th Semester Electrical Engg.Bhojpuri entertainmentNoch keine Bewertungen
- Safety Procedures For Vertical Formwork PDFDokument17 SeitenSafety Procedures For Vertical Formwork PDFbalya7Noch keine Bewertungen