Das könnte Ihnen auch gefallen
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionVon EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionNoch keine Bewertungen
- Indications For All Ceramic RestorationsDokument6 SeitenIndications For All Ceramic RestorationsNaji Z. ArandiNoch keine Bewertungen
- PEAK Restoration of The Endodontically Treated Tooth PDFDokument20 SeitenPEAK Restoration of The Endodontically Treated Tooth PDFana9025100% (1)
- Essential Tissue Healing of the Face and NeckVon EverandEssential Tissue Healing of the Face and NeckBewertung: 5 von 5 Sternen5/5 (2)
- Maciej Zarow Metal Post and Core How To Improve Aesthetics Via WWW Styleitaliano OrgDokument27 SeitenMaciej Zarow Metal Post and Core How To Improve Aesthetics Via WWW Styleitaliano OrgghfhfdghNoch keine Bewertungen
- Class IV Composite Repair for Heavily Textured Central IncisorDokument8 SeitenClass IV Composite Repair for Heavily Textured Central IncisorventynataliaNoch keine Bewertungen
- Cosmetic Dentistry CSD 2013Dokument3 SeitenCosmetic Dentistry CSD 2013Rodrigo Daniel Vela RiveraNoch keine Bewertungen
- Fiber-Reinforced Onlay Composite (Unlocked by WWW - Freemypdf.com)Dokument7 SeitenFiber-Reinforced Onlay Composite (Unlocked by WWW - Freemypdf.com)Adrian DjohanNoch keine Bewertungen
- Post-and-Core Restorations: A Historical ReviewDokument6 SeitenPost-and-Core Restorations: A Historical Reviewdr parveen bathlaNoch keine Bewertungen
- Restoration of Endodontically Treated TeethDokument7 SeitenRestoration of Endodontically Treated TeethSuaeni Kurnia WirdaNoch keine Bewertungen
- Nanohybrid Versus Nano LL Composite in Class I CavitiesDokument5 SeitenNanohybrid Versus Nano LL Composite in Class I CavitiessonygabrielNoch keine Bewertungen
- Castingprocedure 141012113403 Conversion Gate01Dokument103 SeitenCastingprocedure 141012113403 Conversion Gate01joephinNoch keine Bewertungen
- ISSN: 0975-833X: Research ArticleDokument9 SeitenISSN: 0975-833X: Research ArticleSuryo HannaNoch keine Bewertungen
- Additive Contour of Porcelain Veneers A Key Element in Enamel PreservationDokument13 SeitenAdditive Contour of Porcelain Veneers A Key Element in Enamel PreservationPablo BenitezNoch keine Bewertungen
- Removable Partial Dentures: The Clinical Need For InnovationDokument8 SeitenRemovable Partial Dentures: The Clinical Need For InnovationNetra TaleleNoch keine Bewertungen
- Etched Cast RestorationsDokument41 SeitenEtched Cast Restorationssharanya chekkarrajNoch keine Bewertungen
- Composite Resin Core BuildupsDokument12 SeitenComposite Resin Core BuildupsERIKA BLANQUETNoch keine Bewertungen
- Dan Lazar Workflow Composite Veneering On Non Vital Teeth ViaDokument12 SeitenDan Lazar Workflow Composite Veneering On Non Vital Teeth Viaclaudia360Noch keine Bewertungen
- Rethinking FerruleDokument10 SeitenRethinking FerruleteodudeNoch keine Bewertungen
- Color and Shade Management in Esthetic DentistryDokument9 SeitenColor and Shade Management in Esthetic DentistryPaula Francisca MoragaNoch keine Bewertungen
- The Dahl Concept Past Present and FutureDokument9 SeitenThe Dahl Concept Past Present and FuturevivigaitanNoch keine Bewertungen
- Principles of Cavity PreparationDokument5 SeitenPrinciples of Cavity Preparationمعاذ العسافNoch keine Bewertungen
- Biomimetic (Latest)Dokument127 SeitenBiomimetic (Latest)Pawee PiyasowanNoch keine Bewertungen
- Speeds in DentistryDokument38 SeitenSpeeds in DentistryRiya Jain100% (1)
- Microbrush Stamp Technique To Achieve Occlusal Topography For Composite Resin Restorations - A Technical ReportDokument7 SeitenMicrobrush Stamp Technique To Achieve Occlusal Topography For Composite Resin Restorations - A Technical ReportabulzNoch keine Bewertungen
- Biologic Interfaces in Esthetic Dentistry. Part I: The Perio/restorative InterfaceDokument21 SeitenBiologic Interfaces in Esthetic Dentistry. Part I: The Perio/restorative InterfaceRoopa BabannavarNoch keine Bewertungen
- Review Peek PDFDokument11 SeitenReview Peek PDFAlexandra Dumitrache100% (1)
- J Esthet Restor Dent - 2020 - Vargas - A Systematic Approach To Contouring and Polishing Anterior Resin CompositeDokument7 SeitenJ Esthet Restor Dent - 2020 - Vargas - A Systematic Approach To Contouring and Polishing Anterior Resin CompositeScarleth Stephania Perez CastilloNoch keine Bewertungen
- Challenges in dentin bondingDokument11 SeitenChallenges in dentin bondingDanish SattarNoch keine Bewertungen
- Colour Matching A Review of Conventional PDFDokument7 SeitenColour Matching A Review of Conventional PDFAndreea StaicuNoch keine Bewertungen
- Dental Casting Alloys / Orthodontic Courses by Indian Dental AcademyDokument57 SeitenDental Casting Alloys / Orthodontic Courses by Indian Dental Academyindian dental academyNoch keine Bewertungen
- Cobalt-Chromium Alloys in Dentistry An Evaluation of Metal Ion ReleaseDokument7 SeitenCobalt-Chromium Alloys in Dentistry An Evaluation of Metal Ion ReleaseFrank LucariniNoch keine Bewertungen
- AB Dental 2012Dokument62 SeitenAB Dental 2012Charles ElbazNoch keine Bewertungen
- Direct Cuspal-Coverage Posterior Resin Composite Restorations: A Case ReportDokument8 SeitenDirect Cuspal-Coverage Posterior Resin Composite Restorations: A Case ReportDinar ArdhananeswariNoch keine Bewertungen
- Post and CoreDokument11 SeitenPost and CoreAxelJaraNoch keine Bewertungen
- MagnificationDokument52 SeitenMagnificationSiva KumarNoch keine Bewertungen
- 20 2003 - Magne - Anatomic Crown Width LengthDokument9 Seiten20 2003 - Magne - Anatomic Crown Width LengthSilvia KriNoch keine Bewertungen
- Direct Cuspal CoverageDokument8 SeitenDirect Cuspal CoverageLuLu NikhlaturNoch keine Bewertungen
- Volumetric Shrinkage and Film THDokument8 SeitenVolumetric Shrinkage and Film THcalebleon101113Noch keine Bewertungen
- Deliperi S - PPAD - 2005 PDFDokument9 SeitenDeliperi S - PPAD - 2005 PDFAlfredo PortocarreroNoch keine Bewertungen
- Starb Urst BevelDokument4 SeitenStarb Urst BevelventynataliaNoch keine Bewertungen
- 1 Cbct-Evaluation of Remaining Dentin Thickness and Fracture Resistance of Conventional and Conservative Access and Biomechanical Preparation in Molars Using Cone-beam Computed Tomography- An in Vitro StudyDokument4 Seiten1 Cbct-Evaluation of Remaining Dentin Thickness and Fracture Resistance of Conventional and Conservative Access and Biomechanical Preparation in Molars Using Cone-beam Computed Tomography- An in Vitro StudyalbertaugustineNoch keine Bewertungen
- Class II Composite Preparation & RestorationDokument12 SeitenClass II Composite Preparation & RestorationDavid ColonNoch keine Bewertungen
- Treating The Mother of Black Triangles With Bioclear VeneersDokument4 SeitenTreating The Mother of Black Triangles With Bioclear VeneersThe Bioclear ClinicNoch keine Bewertungen
- Newer Advances in Glass Ionomer Cement A Review PDFDokument5 SeitenNewer Advances in Glass Ionomer Cement A Review PDFانس سامي عوادNoch keine Bewertungen
- Posterior Composite Restoration UpdateDokument10 SeitenPosterior Composite Restoration UpdateBianca IovoaiaNoch keine Bewertungen
- Factores Macroesteticos en El Diseño de SonrisaDokument7 SeitenFactores Macroesteticos en El Diseño de SonrisaJassel DurdenNoch keine Bewertungen
- Inlay Onlay Parte 222 PDFDokument23 SeitenInlay Onlay Parte 222 PDFKhenny Jhynmir Paucar VillegasNoch keine Bewertungen
- 16 Access Related Endodontic Mishaps.20170115064301Dokument8 Seiten16 Access Related Endodontic Mishaps.20170115064301Amrutha DasariNoch keine Bewertungen
- Maciej Zarow Composite Veneers Vs Porcelain Veneers Which One To Choose Via WWW Styleitaliano OrgDokument29 SeitenMaciej Zarow Composite Veneers Vs Porcelain Veneers Which One To Choose Via WWW Styleitaliano OrgghfhfdghNoch keine Bewertungen
- Clinical Evaluation of Abutment Teeth of Removable PartialDokument7 SeitenClinical Evaluation of Abutment Teeth of Removable PartialAlex KwokNoch keine Bewertungen
- Advance in MaterialsDokument10 SeitenAdvance in Materialssami robalinoNoch keine Bewertungen
- 8 - Resin BondedDokument14 Seiten8 - Resin BondedÃmøĺã Hûśśiêñ100% (1)
- Clinical techniques for composite restoration placementDokument4 SeitenClinical techniques for composite restoration placementRizta RiztiaNoch keine Bewertungen
- Ceramics in Dentistry-Part I: Classes of MaterialsDokument6 SeitenCeramics in Dentistry-Part I: Classes of MaterialsDilesh PradhanNoch keine Bewertungen
- BY Dr. Fahd Bangash: PresentationDokument32 SeitenBY Dr. Fahd Bangash: PresentationJawad Ahmad0% (1)
- Recent Advances in Materials For All-Ceramic RestorationsDokument19 SeitenRecent Advances in Materials For All-Ceramic RestorationsManishak YessayanNoch keine Bewertungen
- Tooth ColoredDokument11 SeitenTooth Coloredmekit_13Noch keine Bewertungen
- Bio Emulation Edinburgh EventsDokument8 SeitenBio Emulation Edinburgh EventsAing MaungNoch keine Bewertungen
- Recording Centric Jaw Relation - Review ArticleDokument7 SeitenRecording Centric Jaw Relation - Review ArticleDilesh PradhanNoch keine Bewertungen
- BDS Curriculum - Rguhs PDFDokument177 SeitenBDS Curriculum - Rguhs PDFDilesh PradhanNoch keine Bewertungen
- A Brief Overview of CellularDokument5 SeitenA Brief Overview of CellularDilesh PradhanNoch keine Bewertungen
- Crowns Revision ToolDokument36 SeitenCrowns Revision ToolDilesh PradhanNoch keine Bewertungen
- The Glossary of Prosthodontics Terms 9 Edition GPT9Dokument105 SeitenThe Glossary of Prosthodontics Terms 9 Edition GPT9juan85% (13)
- Impression Guide AlginatesDokument28 SeitenImpression Guide AlginatesNadira EhsanNoch keine Bewertungen
- Biology of Implant OsseointegrationDokument11 SeitenBiology of Implant OsseointegrationAmIrNoch keine Bewertungen
- BDS Curriculum - Rguhs PDFDokument177 SeitenBDS Curriculum - Rguhs PDFDilesh PradhanNoch keine Bewertungen
- Effect of Titanium TopographyDokument14 SeitenEffect of Titanium TopographyDilesh PradhanNoch keine Bewertungen
- Osseointegration - A ReviewDokument7 SeitenOsseointegration - A ReviewDilesh PradhanNoch keine Bewertungen
- Arrangemant of Anterior Artificial TeethDokument18 SeitenArrangemant of Anterior Artificial TeethShallini SumbriaNoch keine Bewertungen
- Impression C DDokument48 SeitenImpression C DZaid KhameesNoch keine Bewertungen
- Muscle DeprogrammerDokument17 SeitenMuscle DeprogrammerDilesh PradhanNoch keine Bewertungen
- Ceramic in DentistryDokument6 SeitenCeramic in DentistryDilesh PradhanNoch keine Bewertungen
- Animal Models For Implant Biomaterial Research in BoneDokument10 SeitenAnimal Models For Implant Biomaterial Research in BoneDilesh PradhanNoch keine Bewertungen
- M. S. ChaarDokument15 SeitenM. S. ChaarDilesh PradhanNoch keine Bewertungen
- Omi 14 2 Dubruil13Dokument7 SeitenOmi 14 2 Dubruil13Dilesh PradhanNoch keine Bewertungen
- 4-Cement Retained Vs - HebelDokument8 Seiten4-Cement Retained Vs - HebelDilesh PradhanNoch keine Bewertungen
- Orthodontic Management OF Uncrowded Class Ii Division I Malocclusion IN ChildrenDokument2 SeitenOrthodontic Management OF Uncrowded Class Ii Division I Malocclusion IN ChildrenDilesh PradhanNoch keine Bewertungen
- Ethical: MomentDokument2 SeitenEthical: MomentDilesh PradhanNoch keine Bewertungen
- Full TextDokument5 SeitenFull TextDilesh PradhanNoch keine Bewertungen
- Ceramics in Dentistry-Part I: Classes of MaterialsDokument6 SeitenCeramics in Dentistry-Part I: Classes of MaterialsDilesh PradhanNoch keine Bewertungen
- Media Web Server 4Dokument20 SeitenMedia Web Server 4Dilesh PradhanNoch keine Bewertungen
- CochranDokument11 SeitenCochranDilesh PradhanNoch keine Bewertungen
- SplintingDokument8 SeitenSplintingDilesh PradhanNoch keine Bewertungen
- Effects of Activator and High Pull Headgear Combination Therapy PDFDokument9 SeitenEffects of Activator and High Pull Headgear Combination Therapy PDFDilesh PradhanNoch keine Bewertungen
- Alveolar Rigde AugmentationDokument6 SeitenAlveolar Rigde AugmentationDilesh PradhanNoch keine Bewertungen
- NBDE Resource GuideDokument23 SeitenNBDE Resource GuideAnonymous k8rDEsJsU1Noch keine Bewertungen
- Third Molar Agenesis and Craniofacial Morphology PDFDokument6 SeitenThird Molar Agenesis and Craniofacial Morphology PDFDilesh PradhanNoch keine Bewertungen
- 3-11-8 - Pressure Vessel Cs - UopDokument31 Seiten3-11-8 - Pressure Vessel Cs - UopSean Davis100% (1)
- Equilibrium Calculation For DMEDokument8 SeitenEquilibrium Calculation For DMEAbhishek KumarNoch keine Bewertungen
- Lab Rules Q and ADokument18 SeitenLab Rules Q and Ana-chanNoch keine Bewertungen
- Introduction To Aspen Plus 2013 Tutorial VDokument77 SeitenIntroduction To Aspen Plus 2013 Tutorial VsyafieqNoch keine Bewertungen
- 5018.optical Networking Best Practices HandbookDokument3 Seiten5018.optical Networking Best Practices HandbookashithaprNoch keine Bewertungen
- CH CH CH - CH CL CL N N: PolymerizationDokument40 SeitenCH CH CH - CH CL CL N N: PolymerizationAkash YadavNoch keine Bewertungen
- Kharagpur Vision Academy: Chemistry ProjectDokument14 SeitenKharagpur Vision Academy: Chemistry ProjectSuraj MishraNoch keine Bewertungen
- Mahatma Jyotirao Govindrao PhuleDokument12 SeitenMahatma Jyotirao Govindrao PhuleSagar V. ThakkarNoch keine Bewertungen
- An114 Hand Soldering Tutorial For The Fine Pitch QFP DevicesDokument22 SeitenAn114 Hand Soldering Tutorial For The Fine Pitch QFP DevicesPat Jojo SadavongvivadNoch keine Bewertungen
- PPT1 Plastics Product DesignDokument7 SeitenPPT1 Plastics Product DesignLalitya KrishnanNoch keine Bewertungen
- Carbon Steel Flanges - Pressure and Temperature Ratings - Group 1.1 - Carbon SteelDokument7 SeitenCarbon Steel Flanges - Pressure and Temperature Ratings - Group 1.1 - Carbon Steelnoha azamaliNoch keine Bewertungen
- Spray Nozzles Total STDDokument3 SeitenSpray Nozzles Total STDDylan RamasamyNoch keine Bewertungen
- Niobium and Heat Affected Zone MythologyDokument42 SeitenNiobium and Heat Affected Zone MythologyLayzza TardinNoch keine Bewertungen
- Performance Task 2 Melting and Boiling PointsDokument1 SeitePerformance Task 2 Melting and Boiling PointsVannie MonderoNoch keine Bewertungen
- NEET-2021 (Paper Analysis) FinalDokument32 SeitenNEET-2021 (Paper Analysis) FinalMahasina BegumNoch keine Bewertungen
- Coil SelectionDokument5 SeitenCoil SelectionMohsin Shaikh100% (1)
- Nutritive Evaluation of Ammoniated Benggala GrassDokument2 SeitenNutritive Evaluation of Ammoniated Benggala GrassRolan TuturoongNoch keine Bewertungen
- Global Warming TextsDokument3 SeitenGlobal Warming TextsAnonymous NbKeZIGDVMNoch keine Bewertungen
- Ammonia: Latent Heat of OFDokument34 SeitenAmmonia: Latent Heat of OFCastoriadisNoch keine Bewertungen
- Deep Cryogenic Treatment of A D2 Cold-Work Tool Steel PDFDokument4 SeitenDeep Cryogenic Treatment of A D2 Cold-Work Tool Steel PDFBinh Thanh LeNoch keine Bewertungen
- Tool Makers MicroscopeDokument13 SeitenTool Makers MicroscopeLokesh LokiNoch keine Bewertungen
- Everything About Alkynes - Q&ADokument22 SeitenEverything About Alkynes - Q&AJoostGoNoch keine Bewertungen
- Luminell Datasheet English Version2.0Dokument4 SeitenLuminell Datasheet English Version2.0marius_brkt6284Noch keine Bewertungen
- Fuel Oil AnalysisDokument6 SeitenFuel Oil AnalysisPawan BeniwalNoch keine Bewertungen
- 1 DNA Structure and ReplicationDokument96 Seiten1 DNA Structure and ReplicationmattMd100% (1)
- Proposed NFPA 1851 Decision TreeDokument2 SeitenProposed NFPA 1851 Decision Treeepraetorian100% (1)
- Redken Color HandbookDokument40 SeitenRedken Color HandbookVane Vane100% (3)
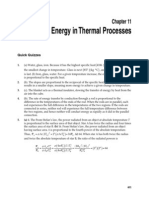
- College Physics 7th Ed Serway Chapter 11Dokument30 SeitenCollege Physics 7th Ed Serway Chapter 11Jorge GomezNoch keine Bewertungen
- 2.1.1 Temperature Programmed Reduction/Oxidation/Desorption (TPR/O/D)Dokument4 Seiten2.1.1 Temperature Programmed Reduction/Oxidation/Desorption (TPR/O/D)AnnafiNoch keine Bewertungen
- To Engineer Is Human: The Role of Failure in Successful DesignVon EverandTo Engineer Is Human: The Role of Failure in Successful DesignBewertung: 4 von 5 Sternen4/5 (137)
- Advanced Modelling Techniques in Structural DesignVon EverandAdvanced Modelling Techniques in Structural DesignBewertung: 5 von 5 Sternen5/5 (3)
- Structural Steel Design to Eurocode 3 and AISC SpecificationsVon EverandStructural Steel Design to Eurocode 3 and AISC SpecificationsNoch keine Bewertungen
- Green Roofs, Facades, and Vegetative Systems: Safety Aspects in the StandardsVon EverandGreen Roofs, Facades, and Vegetative Systems: Safety Aspects in the StandardsNoch keine Bewertungen
- Pocket Guide to Flanges, Fittings, and Piping DataVon EverandPocket Guide to Flanges, Fittings, and Piping DataBewertung: 3.5 von 5 Sternen3.5/5 (22)
- Marine Structural Design CalculationsVon EverandMarine Structural Design CalculationsBewertung: 4.5 von 5 Sternen4.5/5 (13)
- Transmission Pipeline Calculations and Simulations ManualVon EverandTransmission Pipeline Calculations and Simulations ManualBewertung: 4.5 von 5 Sternen4.5/5 (10)
- Built: The Hidden Stories Behind Our StructuresVon EverandBuilt: The Hidden Stories Behind Our StructuresBewertung: 4 von 5 Sternen4/5 (27)
- Design and Construction of Soil Anchor PlatesVon EverandDesign and Construction of Soil Anchor PlatesBewertung: 5 von 5 Sternen5/5 (1)
- Pile Design and Construction Rules of ThumbVon EverandPile Design and Construction Rules of ThumbBewertung: 4.5 von 5 Sternen4.5/5 (15)
- Climate Adaptation Engineering: Risks and Economics for Infrastructure Decision-MakingVon EverandClimate Adaptation Engineering: Risks and Economics for Infrastructure Decision-MakingNoch keine Bewertungen
- Piezocone and Cone Penetration Test (CPTu and CPT) Applications in Foundation EngineeringVon EverandPiezocone and Cone Penetration Test (CPTu and CPT) Applications in Foundation EngineeringNoch keine Bewertungen
- Advanced Design Examples of Seismic Retrofit of StructuresVon EverandAdvanced Design Examples of Seismic Retrofit of StructuresBewertung: 1 von 5 Sternen1/5 (1)
- Carpentry Made Easy - The Science and Art of Framing - With Specific Instructions for Building Balloon Frames, Barn Frames, Mill Frames, Warehouses, Church SpiresVon EverandCarpentry Made Easy - The Science and Art of Framing - With Specific Instructions for Building Balloon Frames, Barn Frames, Mill Frames, Warehouses, Church SpiresBewertung: 1 von 5 Sternen1/5 (2)
- Bridge Engineering: Classifications, Design Loading, and Analysis MethodsVon EverandBridge Engineering: Classifications, Design Loading, and Analysis MethodsBewertung: 4 von 5 Sternen4/5 (16)
- 3D Concrete Printing Technology: Construction and Building ApplicationsVon Everand3D Concrete Printing Technology: Construction and Building ApplicationsNoch keine Bewertungen
- Matrix Methods for Advanced Structural AnalysisVon EverandMatrix Methods for Advanced Structural AnalysisBewertung: 5 von 5 Sternen5/5 (1)
- Offshore Pipelines: Design, Installation, and MaintenanceVon EverandOffshore Pipelines: Design, Installation, and MaintenanceBewertung: 4.5 von 5 Sternen4.5/5 (2)
- Pipeline Planning and Construction Field ManualVon EverandPipeline Planning and Construction Field ManualBewertung: 5 von 5 Sternen5/5 (3)
- Experiment and Calculation of Reinforced Concrete at Elevated TemperaturesVon EverandExperiment and Calculation of Reinforced Concrete at Elevated TemperaturesBewertung: 5 von 5 Sternen5/5 (2)