Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Perawatan Ortodonti Dengan Menggunakan Sistem Damon: (Orthodontic Treatment With Damon System)Dokument1 SeitePerawatan Ortodonti Dengan Menggunakan Sistem Damon: (Orthodontic Treatment With Damon System)Alfonsius JeriNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Restoring Proximal Caries Lesions Conservatively With Tunnel RestorationsDokument8 SeitenRestoring Proximal Caries Lesions Conservatively With Tunnel RestorationsAlfonsius JeriNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Jurnal-4-Naskah 5 JURNAL PDGI Vol 59 No 3Dokument5 SeitenJurnal-4-Naskah 5 JURNAL PDGI Vol 59 No 3Alfonsius JeriNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Dentj 38 2 02Dokument4 SeitenDentj 38 2 02Alfonsius JeriNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Case Report: DiscussionDokument2 SeitenCase Report: DiscussionAlfonsius JeriNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Practice: Syphilitic Chancre of The MouthDokument1 SeitePractice: Syphilitic Chancre of The MouthAlfonsius JeriNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- EAPD Guidelines For The Use of Pit and Fissure Sealants: R. Welbury, M. Raadal, N.A. LygidakisDokument6 SeitenEAPD Guidelines For The Use of Pit and Fissure Sealants: R. Welbury, M. Raadal, N.A. LygidakisAlfonsius JeriNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Pen TingDokument32 SeitenPen TingAlfonsius JeriNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Third Molar ControversyDokument8 SeitenThird Molar ControversyAlfonsius JeriNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Fissure SealantDokument2 SeitenFissure SealantAlfonsius JeriNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
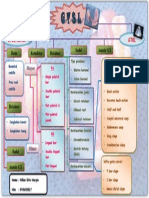
- GTSL Akrilik GTKL: Basis Konektor Retainer Sadel Anasir GTDokument1 SeiteGTSL Akrilik GTKL: Basis Konektor Retainer Sadel Anasir GTAlfonsius JeriNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Oral Candidiasis:: Clinical Manifestations, Diagnosis, and TreatmentDokument0 SeitenOral Candidiasis:: Clinical Manifestations, Diagnosis, and TreatmenttristiarinaNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Research Paper - Celiac DiseaseDokument5 SeitenResearch Paper - Celiac Diseaseapi-316625517100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- 99 Symptoms One Root CauseDokument74 Seiten99 Symptoms One Root CauseIONUT GRIGOROVNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Comparison Between Prone and Supine Position Imrt For Endometrial Cancer (2007)Dokument5 SeitenComparison Between Prone and Supine Position Imrt For Endometrial Cancer (2007)Michelle LEINoch keine Bewertungen
- Drug StudyDokument3 SeitenDrug StudyArra Cristine SeraficaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Assessment of Knowledge, Attitude and Awareness Regarding Cone Beam Computed Tomography Among Dental Graduates in Pune City, IndiaDokument5 SeitenAssessment of Knowledge, Attitude and Awareness Regarding Cone Beam Computed Tomography Among Dental Graduates in Pune City, IndiaSakina JigarNoch keine Bewertungen
- The Role of Acute Phase Proteins in Diagnosis and ManagementDokument6 SeitenThe Role of Acute Phase Proteins in Diagnosis and ManagementCabinet VeterinarNoch keine Bewertungen
- Drug Study FluimucilDokument2 SeitenDrug Study FluimucilJemina Rafanan Racadio0% (1)
- GUIAS UCI para La Alimentación de Paciente CriticoDokument33 SeitenGUIAS UCI para La Alimentación de Paciente CriticoFredy UmbarilaNoch keine Bewertungen
- Marc A. Levitt: AuthorDokument16 SeitenMarc A. Levitt: AuthorAlonso Rodriguez EscobedoNoch keine Bewertungen
- MICP211 Midterm ReviewerDokument39 SeitenMICP211 Midterm ReviewerKrista CruzNoch keine Bewertungen
- Hospital MarketingDokument10 SeitenHospital MarketingYogesh Parchani100% (1)
- Presentation On Health AssessmentDokument12 SeitenPresentation On Health AssessmentSimran ChauhanNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Test Bank For Medical Terminology Simplified A Programmed Learning Approach by Body System 5th Edition Barbara A Gylys Regina M Masters IsDokument15 SeitenTest Bank For Medical Terminology Simplified A Programmed Learning Approach by Body System 5th Edition Barbara A Gylys Regina M Masters Isuntoldvasculumcj4e5cNoch keine Bewertungen
- Patient NursingDokument7 SeitenPatient Nursingsahilchaudhary7Noch keine Bewertungen
- Excel PenelitianDokument8 SeitenExcel PenelitianNisak HumairokNoch keine Bewertungen
- D Dimer Test in VTEDokument35 SeitenD Dimer Test in VTEscribmedNoch keine Bewertungen
- 03 NCP 5 Pulmonary Tuberculosis LalitDokument17 Seiten03 NCP 5 Pulmonary Tuberculosis Lalitamit100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Practical Guide To Insulin Therapy in Type 2 Diabetes: January 2011Dokument91 SeitenPractical Guide To Insulin Therapy in Type 2 Diabetes: January 2011leeyie22Noch keine Bewertungen
- TWSTRS Severity ScaleDokument2 SeitenTWSTRS Severity ScaleErri PratamaNoch keine Bewertungen
- Drug Study (Amiodarone)Dokument8 SeitenDrug Study (Amiodarone)Justine Conui100% (1)
- NSG ProcessDokument6 SeitenNSG ProcessJay-Dee Evangelista PacionNoch keine Bewertungen
- Lab Report 15438869 20231127064225Dokument1 SeiteLab Report 15438869 20231127064225carilloabhe21Noch keine Bewertungen
- Greene & Manfredini 2023 - Overtreatment Successes - 230709 - 135204Dokument11 SeitenGreene & Manfredini 2023 - Overtreatment Successes - 230709 - 135204Abigail HernándezNoch keine Bewertungen
- Virani Et Al 2021 Heart Disease and Stroke Statistics 2021 UpdateDokument490 SeitenVirani Et Al 2021 Heart Disease and Stroke Statistics 2021 UpdatehendridunantikoNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- HistologyDokument15 SeitenHistologySara ŠvedekNoch keine Bewertungen
- Test Sas 16, 17 & 18 Nur 151 Cooa A4: Questions 1 To 10Dokument2 SeitenTest Sas 16, 17 & 18 Nur 151 Cooa A4: Questions 1 To 10Sistine Rose LabajoNoch keine Bewertungen
- STD Facts - Syphilis (Detailed)Dokument4 SeitenSTD Facts - Syphilis (Detailed)Dorothy Pearl Loyola PalabricaNoch keine Bewertungen
- Patient PositioningDokument35 SeitenPatient PositioningMona DoriaNoch keine Bewertungen
- Revised PCCP Spiro Consensus PDFDokument93 SeitenRevised PCCP Spiro Consensus PDFPatriciaDionelaNoch keine Bewertungen
- AsplDokument9 SeitenAsplCristinaNoch keine Bewertungen