Beruflich Dokumente
Kultur Dokumente
1 s2.0 S0300571201000215 Main
Hochgeladen von
udinsyarif0 Bewertungen0% fanden dieses Dokument nützlich (0 Abstimmungen)
19 Ansichten10 Seitenjurnal
Originaltitel
1-s2.0-S0300571201000215-main
Copyright
© © All Rights Reserved
Verfügbare Formate
PDF, TXT oder online auf Scribd lesen
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenjurnal
Copyright:
© All Rights Reserved
Verfügbare Formate
Als PDF, TXT herunterladen oder online auf Scribd lesen
0 Bewertungen0% fanden dieses Dokument nützlich (0 Abstimmungen)
19 Ansichten10 Seiten1 s2.0 S0300571201000215 Main
Hochgeladen von
udinsyarifjurnal
Copyright:
© All Rights Reserved
Verfügbare Formate
Als PDF, TXT herunterladen oder online auf Scribd lesen
Sie sind auf Seite 1von 10
Conference report
Direct adhesive materials: current perceptions and evidence
future solutions
N.H.F. Wilson
*
Department of Restorative Dentistry, University Dental Hospital of Manchester, Higher Cambridge Street, Manchester M15 6FH, UK
Received 10 November 2000; revised 1 March 2001; accepted 23 March 2001
Abstract
This paper reports the proceedings, including the consensus views of an Australasian expert group convened to consider current percep-
tions, evidence and future solutions in the eld of direct adhesive materials. This group, in anticipating a trend to preservative dentistry,
formed the view that caries risk assessment should increasingly inuence the selection of restorative materials. In low caries risk patients,
aesthetic demands typically favour the use of resin-based composites. Interactive (biomimetic) materials based on glass-ionomer chemistry
have particular application in high caries risk patients. Teaching in dental schools, continuing education programmes and research, both in
the laboratory and in the clinical environment should be more attuned to the ever-increasing use of tooth-coloured restorative materials in
everyday clinical practice. Linked to this trend are changes in patientdentist relationships, whereby patients should be encouraged to
become more involved in treatment decision-making. Expert group meetings are suggested to be of value in addressing some of the shortfall
between the need for good evidence and the relentless challenge of the introduction of new products and concepts in the eld of direct
adhesive materials. q 2001 Elsevier Science Ltd. All rights reserved.
Keywords: Composites; Adhesives; Glass-ionomer cements; Resin-modied glass-ionomer cements; Caries; Risk management; Preservative dentistry
1. Introduction
The development of a diversity of adhesive materials has
transformed everyday clinical practice. The ever-expanding
choice of materials has, however, given rise to uncertainties
as to `when', `where' and `how' to use different materials to
best possible advantage. Such uncertainties are exacerbated
by dental schools including different materials and techni-
ques to varying extents in their teaching: journals, miscel-
laneous dental periodicals and continuing education
programmes tending to promote different approaches, and
the manufacturers of materials and associated systems striv-
ing constantly for uniqueness in the marketplace.
Evidence-based practice is increasingly recognised as:
` the conscientious, explicit and judicious use of current
best evidence in making decisions about the care of indivi-
dual patients' [1]; however, the rate at which good
evidence on the efcacy of dental materials can be gener-
ated falls well behind the rate of introduction of materials
and new concepts in operative dentistry. To help address
this shortfall, it is suggested that expert groups serve a valu-
able purpose in meeting to share knowledge and experience
and, through debate, to reach consensus views based on the
collective interpretation of contemporary literature and best
practice. Such activity, while not a systematic evidence-
based approach, highlights areas of strong agreement,
denes areas of variation in thinking and, in turn, provides
pointers for future research.
The purpose of this communication is to report the
proceedings and outcome of a recent Australasian expert
group meeting convened to consider current perceptions,
evidence and future solutions in the eld of direct adhesive
materials.
2. The meeting
The meeting was held in Perth, Western Australia on 12
July 2000. The group comprised the contributing authors to
this report, technical experts (Drs J. Palazzotto, R. Randall,
M. Vrijhoef and Ms J. Pitt) of the sponsoring company (3M
Dental) and the principal author of the report as Chairman.
The programme comprised brief (1015 min) presentations
on selected issues, followed by discussion periods during
which the group was encouraged to thoroughly debate the
issues included in, and arising from the presentations. Inevi-
tably, some of the debate returned to common themes and,
Journal of Dentistry 29 (2001) 307316
Journal
of
Dentistry
0300-5712/01/$ - see front matter q 2001 Elsevier Science Ltd. All rights reserved.
PII: S0300-5712(01)00021-5
www.elsevier.com/locate/jdent
* Tel.: 144-161-275-6660; fax: 144-161-275-6710.
E-mail address: nairn.h.f.wilson@man.ac.uk (N.H.F. Wilson).
as a result, it was concluded that the outcome of the meeting
would be best presented as a summary statement.
3. Abstracts
Each presenter was asked to provide an abstract of his/her
presentation. These are reproduced, as follows, to provide a
backdrop to the summary statement.
3.1. Disease patterns and dental materials in relation to
adult, elderly and special needs patients. G. J. Mount,
University of Adelaide, Adelaide, Australia
The pattern of dental caries is changing throughout the
world, but the sum total is not declining. In the Western
world there is extensive use of uoride, leading to a genera-
tion that is relatively caries free. However, there remains a
small segment of any generation that continues to be highly
susceptible. The problem group is now the aging patient [2]
whose oral environment is affected by increasing reliance on
pharmaceutical drugs for disease control, decreasing physi-
cal capacity and declining mental exibility. These
problems lead rapidly to reinfection with dental caries and
an increase in root surface caries [3] in particular.
In developing countries there is a rapid uptake of Western
dietary routines with an abandonment of traditional foods
and drinks. There is also a serious lack of dental manpower
so that the disease is becoming rampant, as it was in Austra-
lia 50 years ago.
It has now become apparent that operative dentistry
should be divided into two phases [46]. The rst is the
management of new lesions. It is suggested that these should
be approached from a different perspective aimed at conser-
vation of natural tooth structure. The physical requirements
for the restorative material will then be minimal. But for
replacement dentistry, the second phase which currently
occupies the majority of a dentist's time, material require-
ments are much more demanding.
The plastic materials currently in use for operative dentis-
try are amalgam, glass-ionomer and composite resin. Amal-
gam is not aesthetic but it is forgiving of poor handling
techniques and has the best physical properties. It should
not normally be used for the restoration of a new lesion but
retained for extensive load bearing restorations.
Glass-ionomer should be the primary choice for all new
lesions to be laminated if subjected to occlusal load [7]. Its
advantages include ion transport both waysboth in and
outduring its lifetime. There is an ion exchange adhesion
[8], an increase in surface strength over time [9] and possi-
ble remineralisation under a restoration (H. Ngo, personal
communication).
Composite resin is the most aesthetic material and has
wide application. However, there are limitations in wear
resistance and exibility [10]. It adheres well to enamel,
but there is doubt about long-term adhesion to dentine. It
is a very demanding material to place properly, particularly
as the restoration becomes larger.
Developments in the future should be toward increases in
the physical properties of both the glass-ionomers and
composite resins. Improved fracture resistance is desirable
in the glass-ionomers through a decrease in porosity [11]
and improved adaptation to the cavity oor. There is also a
need to improve our understanding of its biocompatibility.
For composite resin there is a need to reduce the exibil-
ity and the wear factor. There should be less emphasis on the
need to develop direct bonding to dentine because glass-
ionomer will already achieve this but the adhesion to enamel
should be subject to further study.
In conclusion, the caries pattern may be changing but
caries rates throughout the world remain high. In the
Western world the emphasis will shift to the aged and
aging patient. The three plastic materials currently available
will remain in general use with the emphasis on amalgam
reducing and on glass-ionomer and composite resin increas-
ing. There is a need to improve the physical properties of
both of the latter because longevity of a restoration has to be
paramount.
3.2. Paediatric dentistry. N. Kilpatrick, Royal Children's
Hospital, Melbourne, Australia
Just over 60% of 5-year old Australians are caries free,
however of the remaining 40%, 15% have at least three
carious teeth [12]. Furthermore, there appears to be a
large amount of untreated decay with up to 40% of all
lesions in 5 year olds untreated [13]. Ignoring the issues
related to accessing dental care, the aetiology of this appar-
ent neglect may include factors related to both the child and
the tooth. Problems associated with cooperation, motivation
and limited intra-oral access make long, complex, techni-
que-sensitive procedures requiring a dry operating eld
inappropriate. Furthermore, primary molars have different
anatomy with large pulp chambers and broad contact areas
increasing the risk of early pulpal involvement and compli-
cated cavity design. A combination of these factors places
huge demands on a restorative technique to be aesthetic,
adhesive and preventive yet simple, fast, technique-insensi-
tive and still be adequately durable.
Current materials and techniques should be benchmarked
against amalgam with its survival time in excess of 7.5 years
[14]. Studies over the last 15 years showgradual improvement
in durability from62%failure for composite after 6 years [15]
to 33% failure after 5 years for Ketac Fil (Espe GmbH,
Seefeld/Oberbay Germany) [16]down to only 6.7% failure
after 4 years for Cheml Superior (DeTrey, Dentsply,
Weybridge, UK) [17]. Resin modied GICs and compomers
show promise with a reported 3-year failure rate for Vitremer
(3M, St Paul, MN, USA) of 19.8%[18] compared with that of
between 1.7 and 3.0% for Dyract (DeTrey, Dentsply,
Weybridge, UK) [17,19]. Ignoring those studies related to
the Atraumatic Restorative Technique (in which assessment
N.H.F. Wilson / Journal of Dentistry 29 (2001) 307316 308
criteria are variable) there is no study longer than 12 months
published on the high density GICs such as Ketac Molar
(Espe) or Fuji IX (GC Int. Corp., Tokyo, Japan).
The above gures hide a detailed analysis of the mechan-
isms of failure from which future research and development
should be guided. Closer inspection of the available studies
plus clinical experience suggests the following unmet
needs: adhesion remains a problem with chemically cured
GICs still prone to be lost from the cavity, whereas the
compomers appear to bond adequately. Fracture occurs at
the isthmus of conventionally designed approximal cavities
[20] and round the margins of smaller box-only aesthetic
restorations implying that brittleness remains a problem.
Signicant debate concerning uoride release exists with
both GICs and to a lesser extent compomers apparently
associated with reduced recurrent caries. Wear resistance
is almost never mentioned although there is some evidence
that resin modied GICs suffer excessive wear when placed
in load bearing areas [21]. A major deciency exists in our
current knowledge in that most studies concentrate on the
restoration of relatively small approximal lesions. The suit-
ability of any of the contemporary adhesive, aesthetic
restorative materials in larger cavities, such as those tradi-
tionally restored using preformed crowns, is unknown. In
summary, it is likely that contemporary adhesive materials
are adequate for the restoration of small approximal lesions
in older children, however, the challenge remains to develop
a material/technique that is appropriate for use in large load
bearing cavities in the younger, often behaviourally challen-
ging, high caries risk child.
3.3. What inuences the general dental practitioner in his
choice of materials. B. M. Bishop, University of Western
Australia, Perth, Australia
The purpose of this presentation is to discuss the factors
that inuence the practising dentist in the choice of direct
restorative materials, the information sources available, the
motivation behind using these information services, and
what other inuences are present to determine the choice
of material.
Dentists have different ideas, aspirations and considera-
tions, and cannot therefore be viewed as one homogenous
group. They choose materials according to their aims and
circumstances.
Dentists may be arranged into three broad groups:
1. Those that are conservative in their choice of materials.
One example of this group would be the recently quali-
ed dentist. Once the young dentist has graduated, there
is a feeling that he or she is trained, and therefore the
whole idea of educational training changes dramatically.
The move into practice often means that the day-to-day
activities are paramount, and learning becomes of
secondary importance for a time. Economic factors
such as income or salary assume a high priority. There-
fore, for a time, the young dentist relies heavily on the
materials he/she has been taught to use at dental school.
There is also the dentist near retirement age, who might
decide that new ideas are of little interest, and therefore
choosing new methods and materials is of little, if any,
signicance to such individuals.
2. Those that are basically business-orientated, and are very
interested in practice management, viewing the practice
primarily as a business rather than a health care unit. This
group looks for efcient, cost effective materials.
3. Those that are primarily patient-orientated and are eter-
nal students. This group will have read journals, attended
courses, seek peer review, and are continually receptive
to new ideas and materials.
None of these groups are mutually exclusive, and a
dentist may from time to time belong to more than one
group. Dentists will also move from one group to another
because of altered circumstances.
There has been a rapid increase in the amount of informa-
tion available to the dentist in recent years. The use of these
sources can be valuable in the continuing education of the
dentist, but some of the sources must be viewed with
caution, in that they may give information, which is unsub-
stantiated, irrelevant or damaging to patient and practi-
tioner.
The information sources available include the practitio-
ner's dental school experience and their mentors at the
school, recommendation from colleagues, suppliers' repre-
sentatives, continuing education programs, hands-on
courses, visiting lecturers sponsored by a variety of sources,
trade shows and conferences, journal articles, textbooks and
advertisements, local study groups, customised educational
packages in the form of video tapes, audio tapes, and
compact discs, and internet and email [22,23].
Dentists use information sources to stay up-to-date, to
access courses which could be difcult to attend as a result
of working in remote regions, to obtain information perti-
nent to the physical area in which they work, to minimize
the chance of litigation, to have a convenient reference
system outside operating time, and to maintain an excel-
lence in the treatment of patients [24].
There are other inuences, besides information sources,
which determine the choice of direct restorative materials
by the general dental practitioner and these include the prop-
erties and performance of the material, the price, the avail-
ability, the effectiveness of usage and coercive bulk buying
as a result of joining a cooperative group.
In summary, the ability to be able to access so much
information in a variety of ways means that the dentist has
a choice of a plethora of materials and techniques. What is
chosen will be a result of the stage of professional develop-
ment, the type of dentist, the use of the information services
and the ability to discern which material will suit the prac-
titioner's purpose.
The perceived trends in the use of the information
N.H.F. Wilson / Journal of Dentistry 29 (2001) 307316 309
services would suggest that the use of electronic information
in its various forms appears to be becoming a major inu-
ence in disseminating knowledge because of the ease of
access and the convenience of use [25].
3.4. Anticariogenic aspects of glass-ionomer cement. M. J.
Tyas, University of Melbourne, Melbourne, Australia
Numerous laboratory studies have investigated the effect
of uoride from glass-ionomer cements (GIC) on the caries
process, including the release of uoride, its uptake by tooth
structure, its effect on bacteria and the performance of GIC
in articial caries models. These data suggest an anticario-
genic effect of GIC in the mouth, and are supplemented by
clinical model studies, which include the effect of GIC on
salivary uoride, bacteria and the bacteria in plaque. An
unequivocal demonstration of prevention of secondary
caries requires evidence from one or more of randomised
controlled trials (RCTs), retrospective and prospective clin-
ical studies or cross-sectional studies, in order of decreasing
validity. However, there are few RCTs in permanent teeth,
and some of these are probably of too short a duration to
demonstrate an effect of GIC [26,27]. Others have compared
amalgam and GIC in deciduous teeth [16,28], and reported
about half the incidence of secondary caries associated with
GIC compared to amalgam. In contrast, Donly et al. [29] did
not nd any clinical difference over 3 years, but polarised
light studies of the exfoliated teeth showed less deminera-
lisation of the cavity walls associated with GIC. Qvist et al.
[28] also found about half the incidence of caries on the
adjacent approximal tooth surface, when GIC was used
compared to amalgam. A similar result was reported by
Svanberg [30] when comparing amalgam and GIC over 3
years in `tunnel' preparations. A retrospective study of 1283
GIC restorations up to 8 years old reported an incidence of
0% secondary caries [31]. However, a cross-sectional study
of the reasons for replacement of 412 glass-ionomer restora-
tions of up to 5 year old [32] reported that half of the repla-
cements were because of secondary caries. Although there
are therefore strong indications from laboratory and clinical
model studies that GIC may have an anticariogenic effect,
unequivocal evidence from randomised controlled trials
remains lacking.
3.5. Laboratory and clinical performance of glass ionomer
cement. M. F. Burrow, University of Melbourne,
Melbourne, Australia
The evaluation of a new, or comparison of currently
available glass ionomer cements (GIC) is initially
completed by a laboratory study and often followed with a
clinical trial. Laboratory investigations are important as
they allow materials to be tested under strictly controlled
conditions. In addition, individual variables can be exam-
ined which have the potential to provide a clue to the
success or failure of a material used in the clinical setting.
Such variables may be comparisons of bonding to normal
vs. carious vs. sclerotic dentine, primary vs. permanent
tooth structure, marginal leakage, the placement environ-
ment (humidity, etc), wear characteristics, and comparison
among material types (conventional vs. resin-modied vs.
reinforced GIC). In the clinical setting such variables can be
very difcult to control, and patient factors may have a
signicant inuence on outcomes; thus making it quite dif-
cult to determine the factors causing loss or poor perfor-
mance of a material. However, a clinical trial whether it is
retrospective or prospective is essential for determining the
long-term success or failure of a material. Laboratory bond
tests have shown that resin-modied GICs have bond
strengths that approach those of resin-based dentine bonding
systems, but the great problem of these studies has been that
the GIC fails cohesively within itself. Therefore these
studies fail to determine the `true' adhesive potential of
GICs [33,34]. A marginal gap study indicated RM-GIC
and conventional GIC to be little different [35] but a micro-
leakage study favoured RM-GIC [36]. However, clinical
studies do not distinguish so distinctly between RM-GIC
and conventional GIC, showing excellent retention rates
and a high quality of restorations up to 10 years [37,38].
Van Dijken [39] compared resin-based systems with a RM-
GIC over 3 years showing the RM-GIC performed best,
even though it is generally the case that RM-GIC bonds
less well to dentine. To date there is very little information
correlating laboratory studies to clinical studies. Platt et al.
[40] concluded that `popular laboratory studies may not be a
good means of predicting superior clinical performance of
Class V materials'. It would seem that we need to reconsider
the extrapolations, which are too often made from labora-
tory data as to how a material may perform clinically. The
interpretation of clinical data on GIC also needs to be
regarded cautiously, as most studies have used sclerosed
non-carious cervical dentine that may not be appropriate
for other parts of the tooth. Perhaps it is time to consider
new tests in the laboratory and new clinical study models.
3.6. Resin discussions. E. S. Duke, Indiana University,
Indianapolis, USA
An increased use of `tooth-coloured' (aesthetic) restora-
tive materials has taken place throughout the world. This use
will continue to increase as public awareness is enhanced,
educational programs are directed more towards the use of
such materials, and continued innovations emerge from
industry. The composite resins of yesterday are quite differ-
ent from the composite resins of today. Mechanical, physi-
cal and handling properties have been improved over
previous generations of materials. When selected for appro-
priate indications, placed with proper techniques, and there-
after maintained, there is no reason to believe that the newer
formulations of composite resins cannot provide a valuable
service to the public in restoring damaged or lost tooth
structure.
Studies have clearly demonstrated that factors unique to
N.H.F. Wilson / Journal of Dentistry 29 (2001) 307316 310
specic patients can often contribute to the behaviour of
restorations of composite resin materials. In addition, the
clinician and his/her specic placement techniques may
also contribute to the ultimate restorative outcome when
using composite resins. To gain long-term survival, in
excess of 10 years, will likely require some form of refurb-
ishment or adjunctive intervention by the clinician. The
repair of a stained margin, an area of chipped composite
replaced, or removal of stain accumulations are examples
of such intervention. Yet, with the focus of tooth longevity
as an outcome such approaches are consistent and seem
logical. Previous patterns of total removal of partially
damaged restorations should be avoided in favour of tooth
conservation. Finally, efforts for educational reform within
dental institutions are vastly needed. Concepts supported by
evidence should be incorporated within dental school curri-
culae in place of long held concepts, often lacking in scien-
tic evidence.
This should further be followed up by programs of conti-
nuing education to the practising profession in the proper
use of composite restorative materials.
3.7. Restorative failure modalities and MI treatment
planning. H. Ngo, University of Adelaide, Adelaide,
Australia
The main objective of a restoration is to restore the physi-
cal and biological integrity of the tooth to allow it to regain
its functional role within the dentition. Too often, practi-
tioners equate the placement of restorations with the treat-
ment of caries and many treatment planning decisions are
made without assessing the patients' caries risk. No cavity
design or restorative material will cure caries.
From a review of the literature, it is apparent that amal-
gam restorations are frequently replaced for various reasons.
Caries has been cited as the main reason for replacement,
accounting for 5060% of all replaced restorations. Other
reasons for replacement include restoration fracture, tooth
fracture, overhangs, poor contour and poor marginal adap-
tation. Compared with caries, each of these other reasons
account for only a small percentage (112%) of replaced
restorations.
The quality of dental restorations is extremely difcult to
dene. Its denition can depend on many factors, including
function, marginal integrity, aesthetics, tissue compatibility,
recurrent caries, pulp status and durability. Failure to
achieve and maintain acceptable levels of quality within
any one of these categories can be considered as the basis
for replacement. Extensive cavity design was used to ensure
complete removal of the diseased portion, to obtain reten-
tion of the restoration and to accommodate the shortcoming
of the restorative material.
All materials are subjected to a process of degradation.
Nothing placed in the oral environment remains unchanged.
At some period during the process of degradation the practi-
tioner makes a decision regarding the need to replace a
given restoration. All too often, the rationale behind the
decision to replace or to retain is subjective. Consequently,
in the absence of obvious failures such as frank secondary
caries and bulk fracture the practitioner uses his intuition as
the principal criterion for replacement.
Like all health professionals, dentists are inherently
cautious about overlooking disease. Elderton [41] warned
the profession against the unwritten principle, `if in doubt,
ll or rell'. Many remuneration systems encourage this
approach. Restorations with their built-in potential for life
long series of repeats, certainly keeps practitioners busy.
The time is right for change of emphasis from reparative
to preventive dentistry. With the widespread availability of
uoride, better understanding of the disease process, possi-
bilities of remineralisation and surface sealing as a thera-
peutic measure: the practitioners should be encouraged to
limit surgical intervention to the absolute minimum and
give prevention the opportunity to work.
3.8. The bonding interface. E. S. Duke, Indiana University,
Indianapolis, USA
Adhesion to tooth structure is essential to provide long-
evity of restorative procedures involving `tooth-coloured'
restorative materials. The glass-ionomer based materials
have rmly established a durable adhesion, that is princi-
pally chemical in nature, to various tooth substrates.
However, most glass-ionomer based materials have not
been shown to possess the long-term durability necessary
to replace damaged tooth structure in the numerous applica-
tions needed in a dental practice.
The literature has shown that most restorations will be
classied as a failure due a defect along the interface
between the remaining tooth structure and the restorative
material. Whether in the form of recurrent caries or
marginal staining, the interface has been identied as the
weak link in most restorative procedures. This defect will
often result in he replacement of a restoration premature of
its potential as a restoration, and is often associated with the
removal of sound tooth structure during this process. Thus,
the long-term prospects for an individual tooth's survival
may be jeopardised.
With the use of composite resins being utilised with
greater frequency in restorative practices, the issue of adhe-
sion and this interface becomes extremely important. Resin
bonding systems have improved slowly over the past 50
years. While adhesion to enamel surfaces has been reason-
ably successful, durable adhesion to dentin and cementum
surfaces has not been as successful. The complexity of
dentin and the continuous changes that accompany the
aging of patients and this substrate have contributed to the
difculty in developing a durable long-lasting seal at inter-
faces.
There have been some recent developments that may
show promise in this area. These involve the use of multi-
phase adhesive systems, combining glass ionomer adhesion
N.H.F. Wilson / Journal of Dentistry 29 (2001) 307316 311
with composite resin techniques and the recent innovation
of new self-etching adhesive systems. Yet, because of the
complexity of the numerous restorative procedures of dental
practice, a single adhesive strategy may not be a reality at
the present time. Rather, selective systems may be more
appropriate at one time over other systems.
3.9. Adhesive dentistry, materials development and
reliability. M. V. Swain, University of Sydney, Sydney,
Australia
Adhesive dentistry and minimal invasive dentistry are
two major factors inuencing both the dental practitioner
and the dental materials manufacturer today. They both
reect developments in the elds of tooth conservation
and adhesive chemistry of the past 100 years. However,
there is still the question as to how these advances in mate-
rials development are related to clinical reliability. There
currently exists a major problem between the areas of mate-
rials development and clinical reliability that is impeding
advances in dental materials, namely the quantication of
adhesion. Two approaches are suggested to overcome this
problem: (i) a classic brittle materials reliability methodol-
ogy (Weibull statistics); and (ii) interfacial fracture
mechanics. The basic assumptions underlying these sugges-
tions are as follows: (a) that engineering concepts which
have proved successful in others areas (from aeronautical
to micro-electronic materials) may be applied to this dental
materials problem; (b) marginal failure and the onset of
recurrent caries is often the outcome of adhesion or interface
fatigue fracture; and (c) the oral environment with its range
of pH and temperature uctuations plus the choice of mate-
rial with its curing strains and in-service stressing contribute
to failure of the interface adhesive bond.
The current means of quantifying adhesion in dentistry
are primarily shear or microtensile strength tests [42,43].
These tests exhibit classic brittle fracture behaviour and
measure the critical stress to initiate failure usually from
some defect. They are characterised by considerable scatter
and interlaboratory reproduceability problems. The Weibull
statistical approach, which considers the probability of frac-
ture at a particular stress, provides a better means of utilising
these results [44]. This approach has been widely embraced
in the eld of ceramics design and enables the inuence of
change in specimen size, shape and time under stress to be
incorporated into the probability of failure at a particular
stress or loading condition. The methodology may be
applied to interface bonding with some caution and enables
an insight into the inuence of curing strain, thermal
cycling, expansion mismatch strains and contact strains on
the probability of failure.
Whilst the Weibull approach enables a means of quanti-
fying failure initiation, it does not satisfactorily assist with
the development of better adhesives or typify the gradual
clinical marginal failure. Furthermore there appears to be
little correlation between adhesive shear or tensile strengths
to tooth structure and clinical performance [45]. In the past
two decades there have been tremendous advances in the
eld of interface fracture mechanics driven especially by the
micro-electronic industry and laminar composite develop-
ments for the aeronautical industry [46]. This approach may
be applied to adhesive dentistry to quantify the (bonding)
energy to peel the dental restorative from the tooth structure.
These tests differ from strength tests in that one attempts to
achieve stable interfacial crack growth over areas represen-
tative of the structure. This approach is only just beginning
to be applied to dental systems such as porcelain and resin to
metal, and is associated with far less scatter than strength
testing [45,47,48]. It provides a method for quantifying
adhesion to enamel and dentine and also to explore the
inuence of the oral environment (pH and temperature) on
the interfacial toughness. In particular, it should allow char-
acterisation of interfacial stress corrosion fatigue cracking
in realistic oral environments. This approach should enable
the manufacturers of dental restoratives and adhesives to
develop more reliable products and perhaps smarter materi-
als that can mitigate acidic challenges in the oral cavity. It
should also enable the dental practitioner to make a more
informed choice of the appropriate restorative material for
specic patients.
4. Summary statement
The discussion sessions were lively, interactive and wide-
ranging. Despite many diverse views having been
expressed, it was possible to identify a number of strongly
supported emerging themes. Within each theme, the group
formed consensus on a number of issues. The themes were
as follows.
4.1. The changing scene
The group had little difculty in concurring with existing
evidence and clinical experience that the demographics of
patient populations are changing rapidly, with a swing
towards older age groups. This, together with an acceptance
that many more teeth are being preserved well into old age,
lent support to the view that the effects of benets to
younger patients of developments in preventive dentistry
are being countered by, for example, an increase in root
caries in the expanding cohorts of older patients. The pattern
and presentation of caries was therefore seen to be changing
with new diagnostic and decision-making challenges facing
practitioners and teachers. The full impact on dentistry of
societal changes in developed countries and, possibly more
importantly, the further development of emerging countries,
notably China in the Asian-Pacic Region, remained dif-
cult to predict. Despite the changing scene, it was antici-
pated that it would continue to be the case that a minority of
people would suffer the bulk of dental disease.
N.H.F. Wilson / Journal of Dentistry 29 (2001) 307316 312
4.2. Patientdentist relationships
There was uniformity of view that patients have increas-
ing expectations of oral health care; are becoming more
discerning, and are showing a strong trend towards wishing
to be involved in decision-making, notably in relation to the
use of tooth-coloured rather than traditional restorative
materials. This trend was thought to be particularly strong
amongst patients in relation to the treatment of their
children.
The `empowered patient' with knowledge of dentistry
through the media and increasingly the internet was identi-
ed as an emerging concept. While the prospect of increased
patient involvement in treatment decision-making was
viewed as something to be welcomed, it was thought to be
important that dentists do not lose control over clinical
matters through patients coming to expect to dictate the
treatment to be provided.
The patientdentist relationship was an area, which the
group considered ought to receive more attention in the
undergraduate curriculum.
4.3. Preservative dentistry
The group's view echoed the perceived groundswell of
international opinion that the `predict and prevent' of
preservative dentistry should replace the traditional `drill
and ll' approach to everyday dental care. Risk assessment
was a conference key word. It was considered that caries
risk assessment and attempts to effect remineralisation of
early lesions of primary caries should precede any operative
intervention, and where intervention was justied, it ought
to be the minimum necessary to ensure a favourable
outcome. In this regard, the importance of limiting the
preparation and taking advantage of adhesive materials in
the placement of initial restorations could not be overem-
phasised. In agreeing that all initial restorations, with the
possible exception of extensive load bearing restorations,
should be of one or more tooth-coloured materials, the
group expressed regret that the teaching of many dental
students, let alone therapists, had been slow to reect such
good practice.
Other concepts, which carried the consensus of the group,
included the discontinuation of the term `permanent restora-
tion', the increasing use of transitional restorations and
having repairs and the refurbishment of existing restorations
accepted as desirable elements of routine care. It was
thought that the dental profession still failed to fully realise
the long-term consequence of many operative interventions.
In breaking away from systems of remuneration, which
favour the now outdated `drill and ll' approach, much
more emphasis must be placed on cost-benet analyses to
provide an evidence-base for alternative forms of treatment.
In such an initiative, it was considered important to embrace
investigations on the life-long consequence of certain forms
of aesthetic dentistry, which involve the repeated bleaching
and bonding of remaining tooth tissues. Such dentistry,
colloquially referred to in certain circles as `bondology',
could, it was suggested, be found to have many varied
long-term consequences if rst applied in young adults
and in a way that was not reversible, as in the case with,
for example, multiple veneers.
In making the much-needed move to preservative dentis-
try, the group identied problems in relation to remunera-
tion and the early diagnosis of disease. Effective
preservative dentistry would also require an acceptance of
the need for routine recall reviews for the monitoring and
maintenance of restored dentitions. Other areas to be
addressed included work to minimise the iatrogenic effects
of existing tooth preparation techniques, the need to develop
new instrumentation and procedures for minimally invasive
procedures, and having dentists develop a much better
understanding of the biomechanics of the effects of tooth
preparation and the polymerisation shrinkage of resin-based
materials.
4.4. Education and training
It was agreed that there is a need for education and train-
ing at all levels to become much more evidence-based.
Similarly it was considered that education and training
should increasingly include instruction in new materials
and techniques and take advantage of fast-moving develop-
ments in the eld of IT. Problem-based, patient-centred and
self-directed learning were all identied as methodologies
with unrealised potential. The potential of the internet was,
however, viewed as the overwhelming force in the eld,
assuming some means may be found to peer review and
otherwise ensure the quality of educational material avail-
able within this rich resource.
Other issues which the group had little difculty agreeing
on spanned the need for the global pooling of resources to
maximise the benets of computer-assisted learning, the
reluctance of schools to restructure to develop, for example,
academic departments of aesthetic dentistry, and the detri-
mental effects that certain forms of advertising are having
on the dissemination of commonality of understanding in
relation to new materials and procedures.
The group was less clear on how manufacturers should
best help clinicians learn to use new materials. Despite
adjuncts to learning including detailed directions for use,
prompt cards, educational videos, sponsored meetings, one
to one familiarisation sessions between clinical personnel
and company representatives and various other educational
activities, it was thought that many dentists continue to have
fundamental misunderstandings in relation to bonding
procedures, let alone techniques for the placement of
tooth-coloured restorative materials in posterior teeth.
With the rate of introduction of new concept materials
anticipated to increase in future years, the problems of
having, in particular, existing practitioners use new restora-
tive systems to best meet patients' needs and expectations
N.H.F. Wilson / Journal of Dentistry 29 (2001) 307316 313
will be an ongoing issue. At the same time, it was noted that
groups such as therapists must have opportunity to have
their style of clinical practice evolve to include the applica-
tion of new materials and techniques. Custom and practice,
let alone limitations on practice, should not frustrate the
adoption of an evidence-based approach to patient care.
4.5. Research
The need for new thinking in relation to research on direct
adhesive materials was considered to be substantial. It was
considered that industry, academia and practitioners should
nd new ways to work together to develop laboratory tests
to predict the clinical handling and performance of materials
and, in turn, materials to meet the changing needs and
expectations of patients. Little merit was seen in, for exam-
ple, endlessly undertaking bond strength measurements and
investigating microleakage unless the clinical relevance of
the ndings of such work can be demonstrated, possibly
through the application of risk assessment techniques, as
occurs in certain other elds of (bio)engineering.
In relation to clinical testing, the group recognised the
need for more commonality in protocol design with greater
compliance with CONSORT guidelines [49]. At one and the
same time, the group formed the view that highly controlled
trials do not give insight into how a material may perform in
the `real world' environment of general dental practice.
Hybrid studies involving practitioners running randomised
controlled trials in their practices were seen to be one of a
number of ways forward. However, any such studies would
still suffer the limitations of the need for long-term reviews
and, as a consequence, a linked priority should remain the
development of laboratory studies capable of predicting
clinical success.
On other aspects of research in the eld of direct adhesive
materials, the group considered the priorities to lie in relation
to the development of less technique-sensitive systems and
smart materials. Early opportunity may exist to combine
glass ionomer and resin-based technologies in one molecule
and thereby create a new class of materials with potentially
favourable clinical properties. Concurrently, research should
focus on specic needs for new materials to meet the needs
of paediatric patients and dentists. At present there would
appear to be an expectation that materials developed for
use in adults will nd application and be successful in
paediatric patients.
4.6. Application and performance of existing materials
The increasing use of tooth-coloured restorative materi-
als, with the concurrent demise of dental amalgam was
viewed as an irreversible trend of gathering momentum.
While indirect tooth-coloured systems were considered to
have certain advantages and specic applications, notably in
prosthodontics and certain forms of aesthetic dentistry, for
everyday use in routine dental care, the practitioner will
continue to rely heavily on direct materials. This approach
was considered to apply to both `replacement dentistry' in
the ongoing management of restored dentitions and in the
management of new lesions, typically in younger patients
who have beneted from developments in preventive
dentistry.
In children, great store would appear to be being placed
on the further development of compomer-type materials for
the treatment of deciduous molars. The lack of a tooth-
coloured alternative to preformed stainless steel crowns is
frustrating and may, in certain situations, be encouraging the
inappropriate extended application of certain direct tooth-
coloured restoratives. Bonded amalgam procedures were
not considered to have a future role in paediatric dentistry.
In adult patients, caries risk assessment may develop a
more recognised role in the selection of materials. In low
caries risk patients in which materials with and without
anticariogenic potential may be used with substantial
success, the practitioner may select the materials best able
to meet the patients' expectations. In contrast, in high caries
risk individuals, selection may be best limited to biomimetic
(smart) materials with the capacity to self-repair and at least
inhibit recurrent and secondary disease. Biomimetic materi-
als should be compatible with more inert materials to allow
combined applications, such as is currently practised in
sandwich (bonded-base) restorations.
Regarding existing materials, the group was unanimous
in the view that no one material is ideal and may only be as
good as the technique with which it is placed. Glass-iono-
mers and resin-modied glass-ionomer cements, despite the
absence of objective clinical data were recognised to have a
polyfunctional anticariogenic/antibacterial action possibly
involving zinc and, in certain materials, strontium as well
as uoride. These materials were viewed as having good
ease of use and tooth/restoration interfacial properties, but
less than desirable fracture and wear resistance. However,
there was something of a tendency to oversimplify the use of
glass ionomers, which, like all other materials require meti-
culous handling. Composites, although highly aesthetic and
greatly improved in recent years in terms of mechanical,
physical and handling properties, are dependent on adhe-
sives to form a bond with dentine. Such bonding is highly
technique-sensitive and less reliable than that formed with a
glass ionomer material, albeit that glass ionomer cements
also suffer certain technique sensitivities. Composites,
however, are viewed by many as the material of choice in
low caries risk patients where the cavosurface margins of
the preparation are of enamel and the restoration is to be
load bearing and/or incorporated in the patient's smile.
Notwithstanding the widespread use of composites, much
remains to be researched in relation to minimising the
effects of polymerisation shrinkage, alternative placement
techniques and instrumentation, and the monitoring and
maintenance of restorations of such materials in clinical
service.
The group's views on the use of compomers in adults
were decidedly mixed. It was considered that further
N.H.F. Wilson / Journal of Dentistry 29 (2001) 307316 314
evidence is required to clarify the role of such materials in
the life-long management of permanent teeth. In the mean-
time, however, members of the group recognised compo-
mers as having certain advantages in the restoration of
deciduous teeth.
Bonded amalgam procedures were considered to have
limited application except possibly in relation to large
compound restorations in situations where the use of an
adhesive may be an alternative to the use of dentine pins.
5. Concluding remarks
In hindsight, the expert group meeting reported in this
paper was considered to have exceeded expectations. The
debate within the group and, as a consequence, the resultant
consensus view went beyond the immediate subject area to
provide a backdrop against which the perceived current
perceptions, evidence and proposed future solutions for
direct adhesive materials may be assessed. The multifaceted
outcome of the meeting is considered to lend support to the
view that expert group meetings are of value in addressing
aspects of the shortfall between the need for good evidence
and the challenge of technology transfer to clinical usage in
the eld of dental biomaterials science.
Acknowledgements
Ms J. Pitt is to be thanked for her exemplary planning and
administration of the meeting.
References
[1] Sackett DL, Rosenburg WM, Gray JA, et al. Evidence-based medi-
cine: What it is and what it isn't. (Editorial). British Medical Journal
1996;312:7172.
[2] Mount GJ. The aged in dentistry. Annals of the Royal Australasian
College of Dental Surgery 1991;11:7581.
[3] Mount GJ. Root surface caries: a recurrent dilemma. Australian
Dental Journal 1986;31:28891.
[4] Mount GJ, Ngo H. Minimal intervention: a new concept for operative
dentistry. Quintessence International 2000;31:52733.
[5] Mount GJ, Ngo H. Minimal intervention: early lesions. Quintessence
International 2000;31:53546.
[6] Mount GJ, Ngo H. Minimal intervention: advanced lesions. Quintes-
sence International 2000;31:6219.
[7] Mount GJ. An atlas of glass ionomers: a clinicians guide. 2nd ed.
London: Martin Dunitz, 1994.
[8] Wilson AD, McLean JW. Glass-ionomer cements. London: Quintes-
sence, 1989.
[9] Nicholson JW, Czamecka B, Limanowska-Shaw H. A preliminary
study of the effect of glass ionomer and related dental cements on
the pH of lactic acid storage solutions. Biomaterials 1999;20:1558.
[10] Jordan RE. Esthetic composite bonding: techniques and materials.
2nd ed. Chicago: Mosby Year Book, 1993.
[11] Ngo H, Tran TD, Duong HT, et al. Relationship between porosity and
shear punch strengths of GICs. Journal of Dental Research
1997;76(SI):423.
[12] Davies MJ, Spencer AJ. Australian Institute of Health and Welfare
Dental Statistics and Research Unit, University of Adelaide, 1996.
[13] Slade GD, Spencer AJ, Davies MJ, et al. Intra-oral distribution and
impact on caries experience among South Australian school children.
Australian Dental Journal 1996;41:34350.
[14] Roberts JF, Sherriff M. The fate and survival of amalgam and
preformed restorations placed in a specialist paediatric dental prac-
tice. British Dental Journal 1990;169:23744.
[15] Varpio M. Proximal composite restorations in primary molars: a 6
year follow-up. Journal of Dentistry in Children 1985;52:43540.
[16] Welbury RR, Walls AW, Murray JJ, et al. The ve-year results of a
clinical trial comparing a glass polyalkenoate (ionomer) cement
restoration with an amalgam restoration. British Dental Journal
1991;170:17781.
[17] Welbury RR, Shaw AJ, Murray JJ, et al. Clinical evaluation of paired
compomer and GIC restorations in primary teeth. International Jour-
nal of Paediatric Dentistry 1999;9 Suppl 1:60.
[18] Folkesson UH, Andersson-Wenckert IE, van Dijken JW. Resin-modi-
ed glass ionomer cement restorations in primary molars. Swedish
Dental Journal 1999;23:19.
[19] Marks LA, Weerheijm KL, van Amerongen WE, et al. Dyract versus
Tytin Class II restorations in primary molars: 35 months evaluation.
Caries Research 1999;33:38792.
[20] Anderssen Wenckert I, van Dijken JWV, Stenberg R. Effect of cavity
formon the durability of glass ionomer cement restorations in primary
molars. Journal of Dentistry in Children 1995;62:197200.
[21] Kilpatrick N, Russell D. Journal of Dental Research 2001 (in press).
[22] Anusavice KJ. Quality evaluation of dental restorations. Criteria for
placement and replacement. Chicago: Quintessence Publishing Co.
Inc, 1989.
[23] Tan A. Survey of continuing dental education attendance in Western
Australia. Australian Dental Journal 1992;37:2969.
[24] Brennan B. Introduction. In: Continuing professional education.
Promise and performance Australian Educational Review No. 30,
Australian Council for Educational Research Limited, 1999; p. 15.
[25] Simonsen RJ. `When life knocks at the door no one can wait'. Quin-
tessence International 1996;27:723.
[26] Tyas MJ. Cariostatic effect of glass ionomer cement: a ve year
clinical study. Australian Dental Journal 1991;36:2369.
[27] Abdalla AI, Alhadainy HA, Garcia-Godoy F. Clinical evaluation of
glass ionomers and compomers in Class I carious lesions. American
Journal of Dentistry 1997;10:1820.
[28] Qvist V, Laurberg L, Poulsen A, et al. Longevity and cariostatic
effects of everyday conventional glass ionomer and amalgam restora-
tions in primary teeth: 3 year results. Journal of Dental Research
1997;76:138796.
[29] Donly KJ, Segura A, Kanellis M, et al. Clinical performance and
caries inhibition of resin-modied glass ionomer cement and amal-
gam restorations. Journal of the American Dental Association
1999;130:145966.
[30] Svanberg M. Class II amalgam restorations, glass ionomer tunnel
restorations and caries development on adjacent tooth surfaces: a
three year clinical study. Caries Research 1992;26:3158.
[31] Mount GJ. Longevity of glass ionomer cements. Journal of Prosthetic
Dentistry 1986;55:6825.
[32] Mjor IA. Glass ionomer cement restorations and secondary caries: a
preliminary report. Quintessence International 1996;27:1714.
[33] Tanumiharja M, Burrow MF, Tyas MJ. The microtensive bond
strength of glass ionomer (polyalkenoate) cements to dentine using
four different conditions. Journal of Dentistry. 2000;28:3616.
[34] Thean HP, Mok BY, Chew CL. Bond strengths of glass ionomer
restoratives to primary vs. permanent dentin. Journal of Dentistry in
Children 2000;67:1126.
[35] Irie M, Suzuki K. Water storage effect on the marginal seal of resin
modied glass ionomer restorations. Operative Dentistry
1999;24:2728.
[36] Wilder A, Swift EJ, May KN, et al. Effect of nishing technique on
the microleakage and surface texture of resin-modied glass ionomer
restorative materials. Journal of Dentistry 2000;28:36773.
N.H.F. Wilson / Journal of Dentistry 29 (2001) 307316 315
[37] Matis B, Cochran M, Carlson T. Longevity of glass ionomer restora-
tive materials: results of a 10 year evaluation. Quintessence Interna-
tional 1996;27:37382.
[38] Brackett WW, Gilpatrick RO, Browning WD, et al. Two-year clinical
performance of a resin-modied glass ionomer restorative material.
Operative Dentistry 1999;24:913.
[39] Van Dijken J. Clinical evaluation of three adhesive systems in Class V
non-carious lesions. Dental Materials 2000;16:28591.
[40] Platt JA, Winkler MM, Matis BA, et al. Correlation of dentin adhesive
laboratory and clinical performance at two years. Journal of Dental
Research 1997;76:184.
[41] Elderton RJ. Quality evaluation of dental restorations. Criteria for
placement and replacement. Chicago: Quintessence Publishing
Co.Inc, 1989.
[42] Hammad IA, Talic YF. Designs of bond strength tests for metal-
ceramic complexes, Review of the literature. Journal of Prosthetic
Dentistry 1996;75:6028.
[43] Burrow M, Tagami J, Negishi T, et al. Early tensile bond strengths of
several enamel and dentin bonding systems. Journal of Dental
Research 1994;73:5228.
[44] McCabe JF, Carrick TE. A statistical approach to the mechanical
testing of dental materials. Dental Materials 1986;2:13942.
[45] Tantbirojn D, Cheng YS, Versluis A, et al. Nominal shear or fracture
mechanics in the assessment of composite-dentin adhesion. Journal of
Dental Research 2000;79:4148.
[46] Mencik J. Mechanics of components with treated and coated surfaces.
Kluwer Academic Press, 1996.
[47] Suansuwan N, Swain MV. New approach for evaluating metal-porce-
lain interfacial bonding. International Journal of Prosthodontics
1999;12:54752.
[48] Sun R, Suansuwan N, Kilpatrick N, et al. Characterisation of tribo-
chemically assisted bonding of composite resin to porcelain and
metal. Journal of Dentistry 2000;28:4415.
[49] Begg C, Cho M, Eastwood S, et al. Improving the quality of reporting
of randomised controlled trials: the CONSORT statement. Journal of
the American Medical Association 1996;276:6379.
N.H.F. Wilson / Journal of Dentistry 29 (2001) 307316 316
Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Digital Signal Processing Lab ManualDokument61 SeitenDigital Signal Processing Lab ManualOmer Sheikh100% (6)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Post War TheatreDokument11 SeitenPost War TheatrePaulPogba77Noch keine Bewertungen
- SCM 2011 PDFDokument4 SeitenSCM 2011 PDFAakash KumarNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- IPE SakibBhaiMagicChothaDokument55 SeitenIPE SakibBhaiMagicChothaTousif SadmanNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Module 6 - Using and Evaluating Instructional MaterialsDokument5 SeitenModule 6 - Using and Evaluating Instructional MaterialsMaria Victoria Padro100% (4)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- IMG - 0009 Thermodynamic Lecture MRCDokument1 SeiteIMG - 0009 Thermodynamic Lecture MRCBugoy2023Noch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Blockchain Disruption in The Forex Trading MarketDokument64 SeitenBlockchain Disruption in The Forex Trading MarketVijayKhareNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Advanced Office Add-In DevelopmentDokument40 SeitenAdvanced Office Add-In DevelopmentReadoneNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- History of Computer ReviewerDokument10 SeitenHistory of Computer ReviewerNeil Andrew Aliazas78% (9)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Generic StructureDokument6 SeitenGeneric StructureAndre AlvarezNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- An Introduction To EFTDokument24 SeitenAn Introduction To EFTkunjammuNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Research Problem: The Key Steps in Choosing A TopicDokument5 SeitenThe Research Problem: The Key Steps in Choosing A TopicJoachim San JuanNoch keine Bewertungen
- Permeability Estimation PDFDokument10 SeitenPermeability Estimation PDFEdison Javier Acevedo ArismendiNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Anatomy & Physiology MCQsDokument26 SeitenAnatomy & Physiology MCQsMuskan warisNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
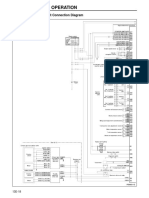
- Structure and Operation: 3. Electronic Control Unit Connection DiagramDokument16 SeitenStructure and Operation: 3. Electronic Control Unit Connection DiagramAung Hlaing Min MyanmarNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Evolis User ManualDokument28 SeitenEvolis User ManualIonmadalin1000Noch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Review. Applications of Ecogeography and Geographic Information Systems in Conservation and Utilization of Plant Genetic ResourcesDokument11 SeitenReview. Applications of Ecogeography and Geographic Information Systems in Conservation and Utilization of Plant Genetic ResourcesEmilio Patané SpataroNoch keine Bewertungen
- BFISDokument1 SeiteBFISEverestNoch keine Bewertungen
- Samsung Galaxy Watch 5 Pro User ManualDokument131 SeitenSamsung Galaxy Watch 5 Pro User Manualzyron100% (1)
- Vitalis 2000Dokument26 SeitenVitalis 2000ARLNoch keine Bewertungen
- Budget of Work Inquiries Investigations and Immersion 19 20Dokument1 SeiteBudget of Work Inquiries Investigations and Immersion 19 20alma florNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Ut 621024Dokument14 SeitenUt 621024DarleiDuarteNoch keine Bewertungen
- Century Vemap PDFDokument5 SeitenCentury Vemap PDFMaster MirrorNoch keine Bewertungen
- Lubricants - McMaster-CarrDokument8 SeitenLubricants - McMaster-CarrjeanyoperNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Chess AI: Competing Paradigms For Machine Intelligence: Shiva Maharaj Nick Polson Alex TurkDokument15 SeitenChess AI: Competing Paradigms For Machine Intelligence: Shiva Maharaj Nick Polson Alex TurkDomingo IslasNoch keine Bewertungen
- C7 On-Highway Engine Electrical System: Harness and Wire Electrical Schematic SymbolsDokument2 SeitenC7 On-Highway Engine Electrical System: Harness and Wire Electrical Schematic SymbolsFeDe Aavina Glez100% (3)
- FMS 427 BusinessPolicy1Dokument279 SeitenFMS 427 BusinessPolicy1Adeniyi Adedolapo OLanrewajuNoch keine Bewertungen
- SOL-Logarithm, Surds and IndicesDokument12 SeitenSOL-Logarithm, Surds and Indicesdevli falduNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)