Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Dental Referral FormDokument1 SeiteDental Referral FormJade M. LolongNoch keine Bewertungen
- K20 Engine Control Module X3 (Lt4) Document ID# 4739106Dokument3 SeitenK20 Engine Control Module X3 (Lt4) Document ID# 4739106Data TécnicaNoch keine Bewertungen
- Nomad Pro Operator ManualDokument36 SeitenNomad Pro Operator Manualdavid_stephens_29Noch keine Bewertungen
- Rotary Valve Functions BookletDokument17 SeitenRotary Valve Functions Bookletamahmoud3Noch keine Bewertungen
- JournalDokument5 SeitenJournalJade M. LolongNoch keine Bewertungen
- Managing Carious LesionsDokument1 SeiteManaging Carious LesionsJade M. LolongNoch keine Bewertungen
- Association of Environmental Tobacco Smoke and Snacking Habits With The Risk of Early Childhood Caries Among 3-Year-Old Japanese ChildrenDokument6 SeitenAssociation of Environmental Tobacco Smoke and Snacking Habits With The Risk of Early Childhood Caries Among 3-Year-Old Japanese ChildrenJade M. LolongNoch keine Bewertungen
- Observed Child and Parent Tooth Brushing Behaviors and Child Oral HealthDokument9 SeitenObserved Child and Parent Tooth Brushing Behaviors and Child Oral HealthJade M. LolongNoch keine Bewertungen
- Ghazal Factors Associated With Early Childhood Caries Incidence Among High Caries-Risk ChildrenDokument9 SeitenGhazal Factors Associated With Early Childhood Caries Incidence Among High Caries-Risk ChildrenJade M. LolongNoch keine Bewertungen
- S2 2013 323973 BibliographyDokument6 SeitenS2 2013 323973 BibliographyJade M. LolongNoch keine Bewertungen
- Evaluation of Fractured Condylar Head Along The Sagittal Plane Report of Three CasesDokument4 SeitenEvaluation of Fractured Condylar Head Along The Sagittal Plane Report of Three CasesJade M. LolongNoch keine Bewertungen
- To Pack or Not To Pack: The Current Status of Periodontal DressingsDokument14 SeitenTo Pack or Not To Pack: The Current Status of Periodontal DressingsJade M. LolongNoch keine Bewertungen
- Clinical Evaluation of Root Canal Obturation Methods in Primary TeethDokument9 SeitenClinical Evaluation of Root Canal Obturation Methods in Primary TeethJade M. LolongNoch keine Bewertungen
- Policy On Oral HabitsDokument2 SeitenPolicy On Oral HabitsJade M. LolongNoch keine Bewertungen
- Preparation of Adhesive Inlays and Onlays.Dokument5 SeitenPreparation of Adhesive Inlays and Onlays.Jade M. LolongNoch keine Bewertungen
- Candida-Associated Denture StomatitisDokument5 SeitenCandida-Associated Denture StomatitisJade M. LolongNoch keine Bewertungen
- G PulpDokument9 SeitenG PulpwindhaNoch keine Bewertungen
- Subcutaneous Emphysema During Third Molar Surgery: A Case ReportDokument4 SeitenSubcutaneous Emphysema During Third Molar Surgery: A Case ReportEdric MichaelNoch keine Bewertungen
- Preliminary Impressions in Microstomia Patients An InnovativeDokument4 SeitenPreliminary Impressions in Microstomia Patients An InnovativeJade M. LolongNoch keine Bewertungen
- Osteomyelitis of The Mandible in A Patient With Osteopetrosis Case Report and Review of The LiteratureDokument6 SeitenOsteomyelitis of The Mandible in A Patient With Osteopetrosis Case Report and Review of The LiteratureJade M. LolongNoch keine Bewertungen
- Palatal Perforation Secondary To Tuberculosis A Case ReportDokument3 SeitenPalatal Perforation Secondary To Tuberculosis A Case ReportJade M. LolongNoch keine Bewertungen
- Comparacao Entre TecnicasDokument14 SeitenComparacao Entre TecnicasjoserodrrNoch keine Bewertungen
- Spring-Bite: A New Device For Jaw Motion Rehabilitation. A Case ReportDokument4 SeitenSpring-Bite: A New Device For Jaw Motion Rehabilitation. A Case ReportJade M. LolongNoch keine Bewertungen
- Location and Presence of Permanent Teeth in A Complete Bilateral Cleft Lip and Palate PopulationDokument6 SeitenLocation and Presence of Permanent Teeth in A Complete Bilateral Cleft Lip and Palate PopulationJade M. LolongNoch keine Bewertungen
- Rehabilitation of Atrophic Maxilla A Review of 101 Zygomatic ImplantsDokument8 SeitenRehabilitation of Atrophic Maxilla A Review of 101 Zygomatic ImplantsJade M. LolongNoch keine Bewertungen
- Ceph HandoutDokument18 SeitenCeph Handoutwaheguru13he13Noch keine Bewertungen
- Occlusal Plane Location in Edentulous Patients A ReviewDokument7 SeitenOcclusal Plane Location in Edentulous Patients A ReviewJade M. Lolong50% (2)
- Occlusal Plane Location in Edentulous Patients A ReviewDokument7 SeitenOcclusal Plane Location in Edentulous Patients A ReviewJade M. Lolong50% (2)
- Case Report of Difficult Dental Prosthesis Insertion Due To Severe Gag ReflexDokument7 SeitenCase Report of Difficult Dental Prosthesis Insertion Due To Severe Gag ReflexJade M. LolongNoch keine Bewertungen
- Ceph TracingDokument1 SeiteCeph TracingJade M. LolongNoch keine Bewertungen
- Luxation InjuriesDokument4 SeitenLuxation InjuriesJade M. LolongNoch keine Bewertungen
- Tabel IotnDokument3 SeitenTabel IotnPuspita PutriNoch keine Bewertungen
- Microcontroller Based Vehicle Security SystemDokument67 SeitenMicrocontroller Based Vehicle Security Systemlokesh_045Noch keine Bewertungen
- PDC NitDokument6 SeitenPDC NitrpshvjuNoch keine Bewertungen
- Coek - Info The Fabric of RealityDokument5 SeitenCoek - Info The Fabric of RealityFredioGemparAnarqiNoch keine Bewertungen
- New Features in IbaPDA v7.1.0Dokument39 SeitenNew Features in IbaPDA v7.1.0Miguel Ángel Álvarez VázquezNoch keine Bewertungen
- Fundamentals Writing Prompts: TechnicalDokument25 SeitenFundamentals Writing Prompts: TechnicalFjvhjvgNoch keine Bewertungen
- Pipe Clamp For Sway Bracing TOLCODokument1 SeitePipe Clamp For Sway Bracing TOLCOEdwin G Garcia ChNoch keine Bewertungen
- Science BDokument2 SeitenScience BIyer JuniorNoch keine Bewertungen
- Como Desarmar Sony Vaio VGN-FE PDFDokument14 SeitenComo Desarmar Sony Vaio VGN-FE PDFPeruInalambrico Redes InalambricasNoch keine Bewertungen
- Ex450-5 Technical DrawingDokument12 SeitenEx450-5 Technical DrawingTuan Pham AnhNoch keine Bewertungen
- F3 Chapter 1 (SOALAN) - RespirationDokument2 SeitenF3 Chapter 1 (SOALAN) - Respirationleong cheng liyNoch keine Bewertungen
- Watchgas AirWatch MK1.0 Vs MK1.2Dokument9 SeitenWatchgas AirWatch MK1.0 Vs MK1.2elliotmoralesNoch keine Bewertungen
- Testing, Adjusting, and Balancing - TabDokument19 SeitenTesting, Adjusting, and Balancing - TabAmal Ka100% (1)
- Sentinel Visualizer 6 User GuideDokument227 SeitenSentinel Visualizer 6 User GuideTaniaNoch keine Bewertungen
- Lab Assignment - 2: CodeDokument8 SeitenLab Assignment - 2: CodeKhushal IsraniNoch keine Bewertungen
- CSS Lab ManualDokument32 SeitenCSS Lab ManualQaif AmzNoch keine Bewertungen
- Fiberglass Fire Endurance Testing - 1992Dokument58 SeitenFiberglass Fire Endurance Testing - 1992shafeeqm3086Noch keine Bewertungen
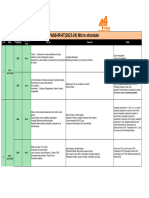
- Narayana Xii Pass Ir Iit (2023 24) PDFDokument16 SeitenNarayana Xii Pass Ir Iit (2023 24) PDFRaghav ChaudharyNoch keine Bewertungen
- Introduction To Java Programming ReviewerDokument90 SeitenIntroduction To Java Programming ReviewerJohn Ryan FranciscoNoch keine Bewertungen
- Zener Barrier: 2002 IS CatalogDokument1 SeiteZener Barrier: 2002 IS CatalogabcNoch keine Bewertungen
- Mbs PartitionwallDokument91 SeitenMbs PartitionwallRamsey RasmeyNoch keine Bewertungen
- Highway Design ProjectDokument70 SeitenHighway Design ProjectmuhammedNoch keine Bewertungen
- How Convert A Document PDF To JpegDokument1 SeiteHow Convert A Document PDF To Jpegblasssm7Noch keine Bewertungen
- ITECH1000 Assignment1 Specification Sem22014Dokument6 SeitenITECH1000 Assignment1 Specification Sem22014Nitin KumarNoch keine Bewertungen
- Solution To QuestionsDokument76 SeitenSolution To QuestionsVipul AggarwalNoch keine Bewertungen
- Tutoriales Mastercam V8 6-11Dokument128 SeitenTutoriales Mastercam V8 6-11Eduardo Felix Ramirez PalaciosNoch keine Bewertungen
- Fitting Fundamentals: For SewersDokument21 SeitenFitting Fundamentals: For SewersLM_S_S60% (5)
- Entropy and The Second Law of Thermodynamics Disorder and The Unavailability of Energy 6Dokument14 SeitenEntropy and The Second Law of Thermodynamics Disorder and The Unavailability of Energy 6HarishChoudharyNoch keine Bewertungen