Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- International Nurse Recruitment in IndiaDokument8 SeitenInternational Nurse Recruitment in IndiaSANANoch keine Bewertungen
- Conditional Performance Plan AgreementDokument5 SeitenConditional Performance Plan AgreementMellie MorcozoNoch keine Bewertungen
- Jhe Document FinalDokument6 SeitenJhe Document FinalSyed Almendras IINoch keine Bewertungen
- Recruitment: Employer Branding - Employer BrandingDokument6 SeitenRecruitment: Employer Branding - Employer BrandingRiley LamNoch keine Bewertungen
- Manpower PlanningDokument42 SeitenManpower Planningr01852009pa33% (3)
- Presented By, Ashita Wilson Neha Lath Kumari Rashmi KuntalDokument27 SeitenPresented By, Ashita Wilson Neha Lath Kumari Rashmi KuntalAshita WilsonNoch keine Bewertungen
- Assignment 6-1 Aggregate PlanningDokument3 SeitenAssignment 6-1 Aggregate PlanningSamson NigusuNoch keine Bewertungen
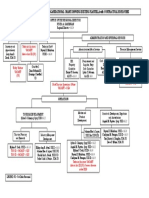
- Dot-Car Organizational ChartDokument1 SeiteDot-Car Organizational ChartRanze Angelique Concepcion BaculloNoch keine Bewertungen
- Chris C Faulkner ResumeDokument3 SeitenChris C Faulkner Resumeapi-307052983Noch keine Bewertungen
- Members' Education Annuity Presentation: BY Insurance Company of East Africa LTDDokument38 SeitenMembers' Education Annuity Presentation: BY Insurance Company of East Africa LTDTusharNoch keine Bewertungen
- Labor Standards Case DigestsDokument111 SeitenLabor Standards Case DigestsNicole SantoallaNoch keine Bewertungen
- U.S. Pastor Council v. EEOCDokument22 SeitenU.S. Pastor Council v. EEOCJohn WrightNoch keine Bewertungen
- BAT Malaysia 2010 Annual ReportDokument227 SeitenBAT Malaysia 2010 Annual ReporthhfahadNoch keine Bewertungen
- Employee Recruitment and Development Process at Maf ShoesDokument32 SeitenEmployee Recruitment and Development Process at Maf Shoesnoureddine ALAHYANENoch keine Bewertungen
- Role of Microfinance in Women EmpowermentDokument10 SeitenRole of Microfinance in Women EmpowermentarcherselevatorsNoch keine Bewertungen
- Unit 2 - Contract of EmploymentDokument22 SeitenUnit 2 - Contract of EmploymentDylan BanksNoch keine Bewertungen
- Nota Staff Perfomance Appraisal 1Dokument24 SeitenNota Staff Perfomance Appraisal 1Nor Hanisah IshakNoch keine Bewertungen
- Guidelines On Labour LawsDokument29 SeitenGuidelines On Labour LawsSARANYAKRISHNAKUMARNoch keine Bewertungen
- Contractor Hse RequirementDokument4 SeitenContractor Hse Requirementelloyd ballesterosNoch keine Bewertungen
- Specimen H1 Econs Paper 1Dokument1 SeiteSpecimen H1 Econs Paper 1tengkahsengNoch keine Bewertungen
- CSC Form 212 Revised 2017Dokument4 SeitenCSC Form 212 Revised 2017Maria Louiesa CadaNoch keine Bewertungen
- Case Delima Solution and AnswersDokument7 SeitenCase Delima Solution and AnswersTeresa M. EimasNoch keine Bewertungen
- AFT Training Agreement - EASA Integrated VER2.6Dokument13 SeitenAFT Training Agreement - EASA Integrated VER2.6Meshari AlrabieNoch keine Bewertungen
- Kristina - MAY 22Dokument1 SeiteKristina - MAY 22bktsuna0201Noch keine Bewertungen
- Topic: Regular Income Tax - Gross Income Aljon J. Roque, CPA, MBADokument3 SeitenTopic: Regular Income Tax - Gross Income Aljon J. Roque, CPA, MBAJhon Ariel JulatonNoch keine Bewertungen
- Republic Act No. 4670 (Wilmar) The Magna Carta For Public School TeachersDokument2 SeitenRepublic Act No. 4670 (Wilmar) The Magna Carta For Public School TeachersShaira LopezNoch keine Bewertungen
- BarricadeDokument13 SeitenBarricadeMonica Isabel Borlagdatan PerezNoch keine Bewertungen
- Planning and Scheduling Operations: Cooper Tire and Rubber CompanyDokument35 SeitenPlanning and Scheduling Operations: Cooper Tire and Rubber CompanyLeycrow RatzingerNoch keine Bewertungen
- Gender Inequality in The Philippine Labor MarketDokument41 SeitenGender Inequality in The Philippine Labor MarketADBGADNoch keine Bewertungen
- 3 P CompansationDokument3 Seiten3 P Compansationpriya srm100% (1)