Das könnte Ihnen auch gefallen
- Functional Rhinoplasty: David W. Kim,, Krista Rodriguez-BrunoDokument17 SeitenFunctional Rhinoplasty: David W. Kim,, Krista Rodriguez-BrunoTarek abo kammerNoch keine Bewertungen
- Jurnal EbmDokument10 SeitenJurnal EbmdeasyNoch keine Bewertungen
- Aijoc 2013 05 043Dokument3 SeitenAijoc 2013 05 043Hussein AhmedNoch keine Bewertungen
- Surgic Al Ma Na Gement Oftheseptal Per Forat Ion: Deborah Watson,, Gregory BarkdullDokument11 SeitenSurgic Al Ma Na Gement Oftheseptal Per Forat Ion: Deborah Watson,, Gregory BarkdullVinoth LakshmikanthNoch keine Bewertungen
- Allergy - 2015 - Ottaviano - Measurements of Nasal Airflow and Patency A Critical Review With Emphasis On The Use of PeakDokument13 SeitenAllergy - 2015 - Ottaviano - Measurements of Nasal Airflow and Patency A Critical Review With Emphasis On The Use of PeakparamopedroNoch keine Bewertungen
- Effect of Non-Surgical Maxillary Expansion On The Nasal Septum Deviation: A Systematic ReviewDokument7 SeitenEffect of Non-Surgical Maxillary Expansion On The Nasal Septum Deviation: A Systematic ReviewsaraNoch keine Bewertungen
- Chronic Rhinosinusitis - An Overview: N.V Deepthi, U.K. Menon, K. MadhumitaDokument6 SeitenChronic Rhinosinusitis - An Overview: N.V Deepthi, U.K. Menon, K. MadhumitaMilanisti22Noch keine Bewertungen
- Most2017 SEPTODokument9 SeitenMost2017 SEPTOJhoel L BenitezNoch keine Bewertungen
- Asian Rhinoplasty1Dokument19 SeitenAsian Rhinoplasty1drbantmNoch keine Bewertungen
- Revision Dacryocystorhinostomy: Adam J. Cohen, F. Campbell Waldrop, and David A. WeinbergDokument11 SeitenRevision Dacryocystorhinostomy: Adam J. Cohen, F. Campbell Waldrop, and David A. WeinbergPrateek SharmaNoch keine Bewertungen
- JR 26 16Dokument5 SeitenJR 26 16ilomurtalaNoch keine Bewertungen
- Preoperative Characteristics of Over 1,300 Functional Septorhinoplasty PatientsDokument7 SeitenPreoperative Characteristics of Over 1,300 Functional Septorhinoplasty PatientsPablo Segales BautistaNoch keine Bewertungen
- Lower Eyelid Complications Associated With Transconjunctival Versus Subciliary Approaches To Orbital Floor FracturesDokument5 SeitenLower Eyelid Complications Associated With Transconjunctival Versus Subciliary Approaches To Orbital Floor Fracturesstoia_sebiNoch keine Bewertungen
- Surgical Treatment of Snoring & Obstructive Sleep Apnoea: Review ArticleDokument10 SeitenSurgical Treatment of Snoring & Obstructive Sleep Apnoea: Review ArticleSiddharth DhanarajNoch keine Bewertungen
- Anaesthesia - September 1992 - Mason - Learning Fibreoptic Intubation Fundamental ProblemsDokument3 SeitenAnaesthesia - September 1992 - Mason - Learning Fibreoptic Intubation Fundamental ProblemsfoolscribdNoch keine Bewertungen
- Contents OcnaDokument4 SeitenContents OcnaGirish SubashNoch keine Bewertungen
- SepDokument7 SeitenSepyuyuNoch keine Bewertungen
- Manuscript 81Dokument7 SeitenManuscript 81Mohit SinhaNoch keine Bewertungen
- Clinical Consensus Statement Diagnosis and Management of Nasal ValveDokument12 SeitenClinical Consensus Statement Diagnosis and Management of Nasal ValveThomasMáximoMancinelliRinaldoNoch keine Bewertungen
- Revision Surgery of The Cleft PalateDokument9 SeitenRevision Surgery of The Cleft PalateMarlon MartinezNoch keine Bewertungen
- The Common Complications After Septoplasty and Septorhinoplasty: A Report in A Series of 127 CasesDokument8 SeitenThe Common Complications After Septoplasty and Septorhinoplasty: A Report in A Series of 127 CasesLeyla M HattaNoch keine Bewertungen
- Nasal Septal PerforationDokument12 SeitenNasal Septal PerforationRini RahmawulandariNoch keine Bewertungen
- 2022 Nasal Pyriform Aperture StenosisDokument2 Seiten2022 Nasal Pyriform Aperture StenosisNicolien van der PoelNoch keine Bewertungen
- Diagnosis and Management of Septal Deviation and Nasal Valve Collapse - A Survey of Canadian OtolaryngologistsDokument6 SeitenDiagnosis and Management of Septal Deviation and Nasal Valve Collapse - A Survey of Canadian OtolaryngologistsruthchristinawibowoNoch keine Bewertungen
- A Comparative Study of Endoscopic Versus Conventional Septoplasty An Analysis of 50 CasesDokument6 SeitenA Comparative Study of Endoscopic Versus Conventional Septoplasty An Analysis of 50 CasesDay LightNoch keine Bewertungen
- Spreaderflapsformiddle Vaultcontourand Stabilization: Milos Kovacevic,, Jochen WurmDokument9 SeitenSpreaderflapsformiddle Vaultcontourand Stabilization: Milos Kovacevic,, Jochen WurmRoberto Cjuno ChaccaNoch keine Bewertungen
- Effect of Cleft Palate Closure Technique On SpeechDokument15 SeitenEffect of Cleft Palate Closure Technique On SpeechLEONARDO ALBERTO CRESPIN ZEPEDANoch keine Bewertungen
- EnsDokument6 SeitenEnsAlwi Qatsir AlyaNoch keine Bewertungen
- 03-Surgical Correction of Nasal ObstructionDokument16 Seiten03-Surgical Correction of Nasal ObstructionGloriaCorredorNoch keine Bewertungen
- Abses SeptumDokument3 SeitenAbses SeptumwitariNoch keine Bewertungen
- Evaluation and Reduction of Nasal TraumaDokument15 SeitenEvaluation and Reduction of Nasal TraumaAnnisa Priscasari DwiyantiNoch keine Bewertungen
- Functional Endoscopic Sinus Surgery - Overview, Preparation, TechniqueDokument10 SeitenFunctional Endoscopic Sinus Surgery - Overview, Preparation, TechniqueHendra SusantoNoch keine Bewertungen
- 2020 Scroll Ligament Nasal TipDokument10 Seiten2020 Scroll Ligament Nasal TipJuliann PedroNoch keine Bewertungen
- Cillo 2019Dokument31 SeitenCillo 2019Marcela GNoch keine Bewertungen
- Bloc de Notas Sin Título 2Dokument1 SeiteBloc de Notas Sin Título 2Jose AriasNoch keine Bewertungen
- J Amjoto 2021 103079Dokument5 SeitenJ Amjoto 2021 103079PUTIGHINANoch keine Bewertungen
- Septum Endoscopico o TraeicionaDokument6 SeitenSeptum Endoscopico o TraeicionavsberraondoNoch keine Bewertungen
- Revision OssiculoplastyDokument14 SeitenRevision Ossiculoplastyapi-19500641Noch keine Bewertungen
- Pediatric Laryngotracheal Stenosis and Airway Reconstruction: A Review of Voice Outcomes, Assessment, and Treatment IssuesDokument11 SeitenPediatric Laryngotracheal Stenosis and Airway Reconstruction: A Review of Voice Outcomes, Assessment, and Treatment Issuescanndy202Noch keine Bewertungen
- VacioDokument17 SeitenVacioKaren HolguinNoch keine Bewertungen
- What's New in Reducing The Impact of Tracheostomy On Communication and Swallowing in The ICUDokument4 SeitenWhat's New in Reducing The Impact of Tracheostomy On Communication and Swallowing in The ICUMarisol BecerraNoch keine Bewertungen
- Diagnosis and Management Crooked Nose EbcrDokument12 SeitenDiagnosis and Management Crooked Nose EbcrnewdewiNoch keine Bewertungen
- 1574-Article Text-2641-1-10-20181107Dokument5 Seiten1574-Article Text-2641-1-10-20181107Faraz HaiderNoch keine Bewertungen
- Stewart 2004Dokument8 SeitenStewart 2004César VidezNoch keine Bewertungen
- Radiological and Endoscopic Ndings in Patients Undergoing Revision Endoscopic Sinus SurgeryDokument10 SeitenRadiological and Endoscopic Ndings in Patients Undergoing Revision Endoscopic Sinus SurgerySanooj SeyedNoch keine Bewertungen
- Adenoidectomy Anatomical Variables As Predic - 2021 - International Journal ofDokument5 SeitenAdenoidectomy Anatomical Variables As Predic - 2021 - International Journal ofHung Son TaNoch keine Bewertungen
- PARS Reader's Digest - Apr 2013Dokument12 SeitenPARS Reader's Digest - Apr 2013info8673Noch keine Bewertungen
- Chapter 5 - Adenoidectomy: Suman GollaDokument7 SeitenChapter 5 - Adenoidectomy: Suman GollaGloriaCorredorNoch keine Bewertungen
- Complications Andmanagement Ofseptoplasty: Amy S. Ketcham,, Joseph K. HanDokument8 SeitenComplications Andmanagement Ofseptoplasty: Amy S. Ketcham,, Joseph K. HanEduardo Cantu GarzaNoch keine Bewertungen
- Orientation of The Premaxilla in The Origin of Septal DeviationDokument5 SeitenOrientation of The Premaxilla in The Origin of Septal Deviationnisrina hanifNoch keine Bewertungen
- Eccles Nasal Air Flow in Health and DiseaseDokument16 SeitenEccles Nasal Air Flow in Health and DiseasemanalNoch keine Bewertungen
- Septumplastia 2Dokument9 SeitenSeptumplastia 2vsberraondoNoch keine Bewertungen
- Counter Autografting of Dorsal SeptumDokument9 SeitenCounter Autografting of Dorsal SeptumÇağlayan YağmurNoch keine Bewertungen
- Indications of The Caldwell-Luc Procedure in The eDokument7 SeitenIndications of The Caldwell-Luc Procedure in The edayu100% (1)
- Klasifikasi Dan Management Deviasi SeptumDokument8 SeitenKlasifikasi Dan Management Deviasi SeptummawarmelatiNoch keine Bewertungen
- Aboudara2009 PDFDokument12 SeitenAboudara2009 PDFYsl OrtodonciaNoch keine Bewertungen
- Internal Nasal ValveDokument6 SeitenInternal Nasal ValveAmmar EidNoch keine Bewertungen
- Otolaryngol - Head Neck Surg - 2020 - Tunkel - Clinical Practice Guideline Nosebleed EpistaxisDokument38 SeitenOtolaryngol - Head Neck Surg - 2020 - Tunkel - Clinical Practice Guideline Nosebleed Epistaxisruba azfr-aliNoch keine Bewertungen
- Orthodontics in Obstructive Sleep Apnea Patients: A Guide to Diagnosis, Treatment Planning, and InterventionsVon EverandOrthodontics in Obstructive Sleep Apnea Patients: A Guide to Diagnosis, Treatment Planning, and InterventionsSu-Jung KimNoch keine Bewertungen
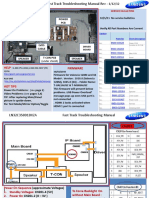
- Samsung LN55C610N1FXZA Fast Track Guide (SM)Dokument4 SeitenSamsung LN55C610N1FXZA Fast Track Guide (SM)Carlos OdilonNoch keine Bewertungen
- GundamDokument25 SeitenGundamBattlecruiser ScharnhorstNoch keine Bewertungen
- N Mon Visualizer OverviewDokument27 SeitenN Mon Visualizer OverviewClaudioQuinterosCarreñoNoch keine Bewertungen
- Grade 7 - R & C - Where Tigers Swim - JanDokument15 SeitenGrade 7 - R & C - Where Tigers Swim - JanKritti Vivek100% (3)
- Under The SHODH Program For ResearchDokument3 SeitenUnder The SHODH Program For ResearchSurya ShuklaNoch keine Bewertungen
- RP Poster FinalDokument1 SeiteRP Poster Finalapi-270795195Noch keine Bewertungen
- CNL DivisionDokument38 SeitenCNL DivisionaniketnareNoch keine Bewertungen
- Marketing Research Completed RevisedDokument70 SeitenMarketing Research Completed RevisedJodel DagoroNoch keine Bewertungen
- Sagittarius ProfileDokument3 SeitenSagittarius ProfileWAQAS SHARIFNoch keine Bewertungen
- Altium Designer Training For Schematic Capture and PCB EditingDokument248 SeitenAltium Designer Training For Schematic Capture and PCB EditingAntonio Dx80% (5)
- Binary To DecimalDokument8 SeitenBinary To DecimalEmmanuel JoshuaNoch keine Bewertungen
- Mind'S Nest Review Center Inc.,: Criteria of A Good Research Problem: Easibility Nterest EsearchabilityDokument21 SeitenMind'S Nest Review Center Inc.,: Criteria of A Good Research Problem: Easibility Nterest EsearchabilitySherlyn Pedida100% (1)
- Data Processing and Management Information System (AvtoBərpaEdilmiş)Dokument6 SeitenData Processing and Management Information System (AvtoBərpaEdilmiş)2304 Abhishek vermaNoch keine Bewertungen
- Xiameter OFS-6020 Silane: Diaminofunctional Silane Features ApplicationsDokument2 SeitenXiameter OFS-6020 Silane: Diaminofunctional Silane Features ApplicationsDelovita GintingNoch keine Bewertungen
- Optimizing Patient Flow: Innovation Series 2003Dokument16 SeitenOptimizing Patient Flow: Innovation Series 2003Jeff SavageNoch keine Bewertungen
- Unit 6 Selected and Short AnswersDokument19 SeitenUnit 6 Selected and Short Answersbebepic355Noch keine Bewertungen
- North-South Railway Project - South LineDokument49 SeitenNorth-South Railway Project - South LinesuperNoch keine Bewertungen
- Course: Consumer Behaviour: Relaunching of Mecca Cola in PakistanDokument10 SeitenCourse: Consumer Behaviour: Relaunching of Mecca Cola in PakistanAnasAhmedNoch keine Bewertungen
- 8 - Packed Tower Design-1Dokument65 Seiten8 - Packed Tower Design-1M.H vafaeiNoch keine Bewertungen
- ESUR Guidelines 10.0 Final VersionDokument46 SeitenESUR Guidelines 10.0 Final Versionkon shireNoch keine Bewertungen
- Perfume 130Dokument3 SeitenPerfume 130Gurdeep BhattalNoch keine Bewertungen
- Motivational QuotesDokument39 SeitenMotivational QuotesNarayanan SubramanianNoch keine Bewertungen
- D6 Gamemasters Aid Screen Weg51019eOGLDokument40 SeitenD6 Gamemasters Aid Screen Weg51019eOGLMr DM100% (1)
- Unit 5, Orders and Cover Letters of Orders For StsDokument13 SeitenUnit 5, Orders and Cover Letters of Orders For StsthuhienNoch keine Bewertungen
- Lux Level Calculation: WILSON ELECTRICAL ENGINEERING BOOKS (Simplified Edition 2020)Dokument1 SeiteLux Level Calculation: WILSON ELECTRICAL ENGINEERING BOOKS (Simplified Edition 2020)Wilson (Electrical Engineer)Noch keine Bewertungen
- Cultivation and Horticulture of SandalwoodDokument2 SeitenCultivation and Horticulture of SandalwoodAnkitha goriNoch keine Bewertungen
- Symantec Endpoint Protection 14.3 RU3 Release NotesDokument28 SeitenSymantec Endpoint Protection 14.3 RU3 Release NotesMilind KuleNoch keine Bewertungen
- Three Moment Equation For BeamsDokument12 SeitenThree Moment Equation For BeamsRico EstevaNoch keine Bewertungen
- Purchase Spec. For Bar (SB425)Dokument4 SeitenPurchase Spec. For Bar (SB425)Daison PaulNoch keine Bewertungen
- CV - en - Hamdaoui Mohamed AmineDokument2 SeitenCV - en - Hamdaoui Mohamed AmineHAMDAOUI Mohamed Amine100% (1)