Das könnte Ihnen auch gefallen
- A Case Study On Chronic Renal DiseaseDokument17 SeitenA Case Study On Chronic Renal Diseasematucojulio100% (1)
- Chronic Kidney Disease Case PresDokument32 SeitenChronic Kidney Disease Case Presnnaesor_1091Noch keine Bewertungen
- Chronic Kidney DiseaseDokument12 SeitenChronic Kidney DiseaseRoseben SomidoNoch keine Bewertungen
- My Case Study of Liver CirrhosisDokument13 SeitenMy Case Study of Liver Cirrhosisdysphile100% (1)
- End Stage Renal Disease Case StudyDokument8 SeitenEnd Stage Renal Disease Case StudyNikko Dela CruzNoch keine Bewertungen
- Case Study CKD DM Type 2Dokument7 SeitenCase Study CKD DM Type 2Brian Cornel0% (3)
- End Stage Renal DiseaseDokument62 SeitenEnd Stage Renal DiseaseMae Navidas DigdiganNoch keine Bewertungen
- ESRD Secondary To Diabetic Nephropathy CASE STUDY Docx 2Dokument42 SeitenESRD Secondary To Diabetic Nephropathy CASE STUDY Docx 2Eyerusalem100% (1)
- A Case Study On Chronic Kidney DiseaseDokument103 SeitenA Case Study On Chronic Kidney DiseaseLouella Mae CoraldeNoch keine Bewertungen
- Case Study On End Stage Renal FailureDokument19 SeitenCase Study On End Stage Renal Failurelenecarglbn100% (1)
- Chronic Renal FailureDokument1 SeiteChronic Renal Failurejj_cuttingedges100% (2)
- Case Study On Chronic Kidney DiseaseDokument101 SeitenCase Study On Chronic Kidney DiseaseZNEROL100% (6)
- CHF Case StudyDokument38 SeitenCHF Case StudyMelissa David100% (1)
- Chronic Kidney DiseaseDokument15 SeitenChronic Kidney Diseaseapi-270623039Noch keine Bewertungen
- Chronic Kidney DiseaseDokument33 SeitenChronic Kidney DiseasesexiiimammaNoch keine Bewertungen
- Liver CirrhosisDokument31 SeitenLiver CirrhosisAsniah Hadjiadatu Abdullah100% (1)
- Chronic Renal FailureDokument37 SeitenChronic Renal Failuredorkiebaby100% (10)
- CKD (F&e)Dokument110 SeitenCKD (F&e)Al-nazer Azer Al100% (1)
- Case Study On Chronic Kidney Disease Probably To Secondary HypertensionDokument18 SeitenCase Study On Chronic Kidney Disease Probably To Secondary Hypertensionkyeria77% (26)
- Case Study 18 CKDDokument7 SeitenCase Study 18 CKDapi-301049551Noch keine Bewertungen
- Case Study On Alcoholic Liver DiseaseDokument24 SeitenCase Study On Alcoholic Liver DiseaseKristine Alejandro100% (5)
- CaseStudy ChronicRenalFailureDokument29 SeitenCaseStudy ChronicRenalFailureCarlcedrick ManlapusNoch keine Bewertungen
- Pathophysiology of Alcoholic Liver DiseaseDokument4 SeitenPathophysiology of Alcoholic Liver Diseaseshailendra tripathiNoch keine Bewertungen
- Liver Cirrhosis: A Case Study OnDokument31 SeitenLiver Cirrhosis: A Case Study OnCharmaine del RosarioNoch keine Bewertungen
- Chronic Kidney Disease Case StudyDokument52 SeitenChronic Kidney Disease Case StudyGi100% (1)
- Acute Glomerulonephritis Case StudyDokument12 SeitenAcute Glomerulonephritis Case Study19lyon92100% (6)
- Acute Glomerulonephritis 42-mDokument27 SeitenAcute Glomerulonephritis 42-mcbanguisNoch keine Bewertungen
- Case Study - Chronic Kidney Disease Treated With DialysisDokument7 SeitenCase Study - Chronic Kidney Disease Treated With Dialysisapi-387604918100% (1)
- Acute Renal FailureDokument59 SeitenAcute Renal Failurepaul_v_44440% (1)
- Case Study 18Dokument4 SeitenCase Study 18api-271284613Noch keine Bewertungen
- Case Study - Septic ShockDokument16 SeitenCase Study - Septic ShockIrene Mae Villanueva Ariola100% (2)
- Case Study 10 Renal FailureDokument19 SeitenCase Study 10 Renal FailureAriadne Cordelette100% (2)
- End - Stage Renal DiseaseDokument59 SeitenEnd - Stage Renal DiseaseJonathan Diaz93% (15)
- Non-St Segment Elevation Myocardial Infarction (Nstemi)Dokument24 SeitenNon-St Segment Elevation Myocardial Infarction (Nstemi)MHIEMHOINoch keine Bewertungen
- Chronic Renal FailureDokument3 SeitenChronic Renal FailureIvana Yasmin Bulandres100% (2)
- Alcoholic Liver DiseaseDokument70 SeitenAlcoholic Liver Diseaseaannaass nNoch keine Bewertungen
- Pathophysiology of Chronic Kidney Disease: Predisposing Factors: Precipitating FactorsDokument1 SeitePathophysiology of Chronic Kidney Disease: Predisposing Factors: Precipitating FactorsReina Samson0% (1)
- Chronic Kidney Disease CompilationDokument33 SeitenChronic Kidney Disease CompilationGwen Stefanie Lagrimas ValloyasNoch keine Bewertungen
- Myocardial Infarction Case StudyDokument19 SeitenMyocardial Infarction Case Studyapi-312992151Noch keine Bewertungen
- Acute GlomerulonephritisDokument17 SeitenAcute GlomerulonephritisBayanSecond WardNoch keine Bewertungen
- Case Study of Chronic Kidney DiseaseDokument54 SeitenCase Study of Chronic Kidney DiseaseJomari Zapanta100% (4)
- Cholecystitis Case PresDokument103 SeitenCholecystitis Case PresAnton LaurencianaNoch keine Bewertungen
- CKDDokument35 SeitenCKDNATTAPAT SANGKAKULNoch keine Bewertungen
- Case Analysis FinalDokument29 SeitenCase Analysis FinalVeyNoch keine Bewertungen
- NCP Liver CirrhosisDokument7 SeitenNCP Liver CirrhosisIris Jimenez-BuanNoch keine Bewertungen
- Liver Cirrhosis: Review HepatologyDokument71 SeitenLiver Cirrhosis: Review HepatologyAstri Arri FebriantiNoch keine Bewertungen
- Acute Renal Failure Case StudyDokument18 SeitenAcute Renal Failure Case Studymanjeet3680% (5)
- Chronic Kidney DiseaseDokument9 SeitenChronic Kidney Diseaseluvgrace100% (1)
- Case StudyDokument37 SeitenCase StudyAnonymous t78m8ku100% (1)
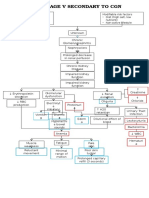
- Pathophysiology CKD Secondary To CGNDokument1 SeitePathophysiology CKD Secondary To CGNNathan Vince CruzNoch keine Bewertungen
- Kidney Transplant PresentationDokument23 SeitenKidney Transplant PresentationApple Dela CruzNoch keine Bewertungen
- GlomerulonephritisDokument8 SeitenGlomerulonephritisMatthew Ryan100% (1)
- CHRONIC KIDNEY DISEASE Secondary To Chronic GlomerulonephritisDokument31 SeitenCHRONIC KIDNEY DISEASE Secondary To Chronic GlomerulonephritisJerwin Jade Bolor33% (3)
- 17 Urinary SystemDokument5 Seiten17 Urinary SystemOribello, Athenna Jae W.Noch keine Bewertungen
- Case Study ReportDokument16 SeitenCase Study ReportOluebube HerbertNoch keine Bewertungen
- ManuscriptDokument97 SeitenManuscriptAi RimandoNoch keine Bewertungen
- Chronic Renal FailureDokument46 SeitenChronic Renal Failurestepharry08100% (1)
- Case Study JatDokument45 SeitenCase Study JatHSEINNoch keine Bewertungen
- Mr. R.E.B. - CKDDokument61 SeitenMr. R.E.B. - CKDChristy Rose AgrisNoch keine Bewertungen
- CKD Case AnalysisDokument25 SeitenCKD Case Analysisしゃいな ふかみNoch keine Bewertungen
- Informed ConsentDokument4 SeitenInformed Consentnnaesor_1091Noch keine Bewertungen
- Impaired Skin Integrity Related To Surgical Removal of SkinDokument3 SeitenImpaired Skin Integrity Related To Surgical Removal of Skinnnaesor_10910% (2)
- Fire Works InjuryDokument39 SeitenFire Works Injurynnaesor_1091Noch keine Bewertungen
- Deductive Reasoning ReportDokument3 SeitenDeductive Reasoning Reportnnaesor_1091Noch keine Bewertungen
- Deductive Reasoning.Dokument13 SeitenDeductive Reasoning.nnaesor_1091Noch keine Bewertungen
- Some One Like You CordDokument2 SeitenSome One Like You Cordnnaesor_1091Noch keine Bewertungen
- The Lower Limb Tendinopathies Etiology, Biology and Treatment-Springer International (2016)Dokument202 SeitenThe Lower Limb Tendinopathies Etiology, Biology and Treatment-Springer International (2016)Tony Miguel Saba Saba100% (1)
- Learning Through PlayDokument2 SeitenLearning Through PlayThe American Occupational Therapy Association100% (1)
- A View On TB ControlDokument30 SeitenA View On TB ControlhonorinanuguidNoch keine Bewertungen
- Psychological Impact of Light and ColorDokument3 SeitenPsychological Impact of Light and ColorOwais MahmoodNoch keine Bewertungen
- Product CatalogDokument13 SeitenProduct Catalogkleos70Noch keine Bewertungen
- A Comparative Study of The Clinical Efficiency of Chemomechanical Caries Removal Using Carisolv® and Papacarie® - A Papain GelDokument8 SeitenA Comparative Study of The Clinical Efficiency of Chemomechanical Caries Removal Using Carisolv® and Papacarie® - A Papain GelA Aran PrastyoNoch keine Bewertungen
- Current Issues & Trends in Older: Persons Chronic CareDokument12 SeitenCurrent Issues & Trends in Older: Persons Chronic CareKeepItSecretNoch keine Bewertungen
- Indocollyre PDFDokument6 SeitenIndocollyre PDFUpik MoritaNoch keine Bewertungen
- Understanding HypokalemiaDokument4 SeitenUnderstanding HypokalemiaAudrey Leonar100% (1)
- Daniel J Carlat-The Psychiatric InterviewDokument391 SeitenDaniel J Carlat-The Psychiatric InterviewFrancielle Machado86% (7)
- NCP-DP NCM112LecDokument4 SeitenNCP-DP NCM112LecShane CabucosNoch keine Bewertungen
- Threatened AbortionDokument3 SeitenThreatened Abortionjay5ar5jamorabon5torNoch keine Bewertungen
- Advances and Challenges in Stroke RehabilitationDokument13 SeitenAdvances and Challenges in Stroke Rehabilitationarif 2006Noch keine Bewertungen
- Castlegar/Slocan Valley Pennywise November 21, 2017Dokument42 SeitenCastlegar/Slocan Valley Pennywise November 21, 2017Pennywise PublishingNoch keine Bewertungen
- Teresa Iacono 2014 What It Means To Have Complex Communication NeedsDokument6 SeitenTeresa Iacono 2014 What It Means To Have Complex Communication Needsapi-260603230Noch keine Bewertungen
- WarfarinDokument10 SeitenWarfarinMar Ordanza100% (1)
- Insulin IndexDokument13 SeitenInsulin IndexbookbookpdfNoch keine Bewertungen
- 3 Cultural GenogramDokument11 Seiten3 Cultural GenogramJohn Stanley100% (2)
- Assessing Apical PulseDokument5 SeitenAssessing Apical PulseMatthew Ryan100% (1)
- Lumbar Disc HerniationDokument8 SeitenLumbar Disc Herniationandra_scooterNoch keine Bewertungen
- Silver Hill Hospital Chronic Pain and Recovery CenterDokument8 SeitenSilver Hill Hospital Chronic Pain and Recovery CenterSilver Hill HospitalNoch keine Bewertungen
- The Art of Narrative PsychiatryDokument227 SeitenThe Art of Narrative Psychiatryroxyoancea100% (8)
- BiomekanikDokument474 SeitenBiomekanikRicaariani MyGeisha SmashblastNoch keine Bewertungen
- Montano NCP TbiDokument6 SeitenMontano NCP TbiKarl Angelo MontanoNoch keine Bewertungen
- European Union Herbal Monograph Mentha X Piperita L Aetheroleum Revision 1 enDokument12 SeitenEuropean Union Herbal Monograph Mentha X Piperita L Aetheroleum Revision 1 enTabsherah AnsariNoch keine Bewertungen
- How To Use BNF With ScenariosDokument6 SeitenHow To Use BNF With ScenariosLuxs23Noch keine Bewertungen
- Liver CleanseDokument84 SeitenLiver CleanseBrian Jones100% (7)
- Color - Enhancing Foods For Aquarium Fish: Sivaramakris Hnan.T, IvDokument18 SeitenColor - Enhancing Foods For Aquarium Fish: Sivaramakris Hnan.T, IvArun SudhagarNoch keine Bewertungen
- Acne RosaceaDokument28 SeitenAcne Rosaceanathy_soares100% (1)
- Phenoxymethyl Penicillin Potassium: PaciphenDokument2 SeitenPhenoxymethyl Penicillin Potassium: PaciphenKath CorralesNoch keine Bewertungen
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainVon EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainBewertung: 3.5 von 5 Sternen3.5/5 (38)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomVon EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomBewertung: 4 von 5 Sternen4/5 (1)
- Eat & Run: My Unlikely Journey to Ultramarathon GreatnessVon EverandEat & Run: My Unlikely Journey to Ultramarathon GreatnessNoch keine Bewertungen
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyVon EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyBewertung: 4.5 von 5 Sternen4.5/5 (4)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeVon EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNoch keine Bewertungen
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookVon EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookBewertung: 3.5 von 5 Sternen3.5/5 (2)
- The Complete Beck Diet for Life: The 5-Stage Program for Permanent Weight LossVon EverandThe Complete Beck Diet for Life: The 5-Stage Program for Permanent Weight LossBewertung: 3.5 von 5 Sternen3.5/5 (6)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarVon EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarBewertung: 5 von 5 Sternen5/5 (352)
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingVon EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingBewertung: 5 von 5 Sternen5/5 (61)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonVon EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonBewertung: 3.5 von 5 Sternen3.5/5 (33)
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodVon EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNoch keine Bewertungen
- Eat Complete: The 21 Nutrients That Fuel Brainpower, Boost Weight Loss, and Transform Your HealthVon EverandEat Complete: The 21 Nutrients That Fuel Brainpower, Boost Weight Loss, and Transform Your HealthBewertung: 2 von 5 Sternen2/5 (1)
- The Stark Naked 21-Day Metabolic Reset: Effortless Weight Loss, Rejuvenating Sleep, Limitless Energy, More MojoVon EverandThe Stark Naked 21-Day Metabolic Reset: Effortless Weight Loss, Rejuvenating Sleep, Limitless Energy, More MojoNoch keine Bewertungen
- Keto Friendly Recipes: Easy Keto For Busy PeopleVon EverandKeto Friendly Recipes: Easy Keto For Busy PeopleBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Rapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsVon EverandRapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsBewertung: 5 von 5 Sternen5/5 (7)
- Good Sugar Bad Sugar: Eat yourself free from sugar and carb addictionVon EverandGood Sugar Bad Sugar: Eat yourself free from sugar and carb addictionBewertung: 4.5 von 5 Sternen4.5/5 (29)
- Smarter Not Harder: The Biohacker's Guide to Getting the Body and Mind You WantVon EverandSmarter Not Harder: The Biohacker's Guide to Getting the Body and Mind You WantBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Foods That Cause You to Lose Weight: The Negative Calorie EffectVon EverandFoods That Cause You to Lose Weight: The Negative Calorie EffectBewertung: 3 von 5 Sternen3/5 (5)
- Dr. Nowzaradan's Diet Plan: The Scales Don't Lie, People Do! The Only 1200 kcal Diet from Dr. NOW to Lose Weight Fast. 30-Day Diet PlanVon EverandDr. Nowzaradan's Diet Plan: The Scales Don't Lie, People Do! The Only 1200 kcal Diet from Dr. NOW to Lose Weight Fast. 30-Day Diet PlanNoch keine Bewertungen
- The Glucose Goddess Method: The 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingVon EverandThe Glucose Goddess Method: The 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingBewertung: 4.5 von 5 Sternen4.5/5 (4)
- Rapid Weight Loss Hypnosis for Women: Self-Hypnosis, Affirmations, and Guided Meditations to Burn Fat, Gastric Band, Eating Habits, Sugar Cravings, Mindfulness, and More.Von EverandRapid Weight Loss Hypnosis for Women: Self-Hypnosis, Affirmations, and Guided Meditations to Burn Fat, Gastric Band, Eating Habits, Sugar Cravings, Mindfulness, and More.Bewertung: 5 von 5 Sternen5/5 (36)
- The Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondVon EverandThe Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondBewertung: 4.5 von 5 Sternen4.5/5 (28)
- The Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesVon EverandThe Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesNoch keine Bewertungen
- The Carnivore Diet Bible: A Beginner’s Guide To Achieving Optimum Health, A Lean Body And Fast Fat LossVon EverandThe Carnivore Diet Bible: A Beginner’s Guide To Achieving Optimum Health, A Lean Body And Fast Fat LossBewertung: 5 von 5 Sternen5/5 (1)
- Extreme Weight Loss Hypnosis for Women: Powerful & Rapid Weight-Loss: Self-Hypnosis, Guided Meditations & Affirmations to Burn Fat, Look Amazing, Change Your Habits, Emotional Eating and More.Von EverandExtreme Weight Loss Hypnosis for Women: Powerful & Rapid Weight-Loss: Self-Hypnosis, Guided Meditations & Affirmations to Burn Fat, Look Amazing, Change Your Habits, Emotional Eating and More.Bewertung: 5 von 5 Sternen5/5 (28)
- Body Confidence: Venice Nutrition's 3 Step System That Unlocks Your Body's Full PotentialVon EverandBody Confidence: Venice Nutrition's 3 Step System That Unlocks Your Body's Full PotentialBewertung: 4 von 5 Sternen4/5 (2)
- Ultrametabolism: The Simple Plan for Automatic Weight LossVon EverandUltrametabolism: The Simple Plan for Automatic Weight LossBewertung: 4.5 von 5 Sternen4.5/5 (28)