Das könnte Ihnen auch gefallen
- Social Media-2Dokument10 SeitenSocial Media-2api-258330934Noch keine Bewertungen
- Fasdfinalworkingdocument1 2Dokument42 SeitenFasdfinalworkingdocument1 2api-258330934Noch keine Bewertungen
- Portfolio CVDokument3 SeitenPortfolio CVapi-258330934Noch keine Bewertungen
- Stephanie Janzen - Best PracticesDokument11 SeitenStephanie Janzen - Best Practicesapi-258330934Noch keine Bewertungen
- Fiona Portfolio ReportDokument4 SeitenFiona Portfolio Reportapi-258330934Noch keine Bewertungen
- Debate AnalysisDokument7 SeitenDebate Analysisapi-258330934Noch keine Bewertungen
- Reading Comprehension Intervention StrategiesDokument18 SeitenReading Comprehension Intervention Strategiesapi-258330934Noch keine Bewertungen
- PPVT 4Dokument13 SeitenPPVT 4api-258330934100% (1)
- Personal Position PaperDokument18 SeitenPersonal Position Paperapi-258330934Noch keine Bewertungen
- Article Critique Edps 612 l01Dokument8 SeitenArticle Critique Edps 612 l01api-258330934Noch keine Bewertungen
- First Step To SuccessDokument20 SeitenFirst Step To Successapi-258330934Noch keine Bewertungen
- Janzen Stephanie - Article Critique Edps 612 03 Docx0-2Dokument8 SeitenJanzen Stephanie - Article Critique Edps 612 03 Docx0-2api-258330934Noch keine Bewertungen
- Ecological Article CritiqueDokument7 SeitenEcological Article Critiqueapi-258330934Noch keine Bewertungen
- Janzen - 674 Asynch Activity Week 10Dokument3 SeitenJanzen - 674 Asynch Activity Week 10api-258330934Noch keine Bewertungen
- Adhd and Ritalin PaperDokument18 SeitenAdhd and Ritalin Paperapi-258330934Noch keine Bewertungen
- Jordan PPDokument8 SeitenJordan PPapi-258330934Noch keine Bewertungen
- BSP Evaluation PlanDokument3 SeitenBSP Evaluation Planapi-258330934Noch keine Bewertungen
- Ethical OrganizationDokument11 SeitenEthical Organizationapi-258330934Noch keine Bewertungen
- WM MathDokument6 SeitenWM Mathapi-258330934Noch keine Bewertungen
- Janzen - Edps 674 FbaDokument11 SeitenJanzen - Edps 674 Fbaapi-258330934Noch keine Bewertungen
- Cultural BiasDokument6 SeitenCultural Biasapi-258330934Noch keine Bewertungen
- Stephaniejanzen15 11 2012Dokument13 SeitenStephaniejanzen15 11 2012api-258330934Noch keine Bewertungen
- Shifting Paradigms in The History of Special EducationDokument10 SeitenShifting Paradigms in The History of Special Educationapi-258330934Noch keine Bewertungen
- Portfolio Same Report - Jordan Academic PracticumDokument5 SeitenPortfolio Same Report - Jordan Academic Practicumapi-258330934Noch keine Bewertungen
- Anti Bullying 2Dokument31 SeitenAnti Bullying 2api-258330934Noch keine Bewertungen
- Assessment ReviewDokument4 SeitenAssessment Reviewapi-258330934Noch keine Bewertungen
- Processing Speed HandoutDokument1 SeiteProcessing Speed Handoutapi-258330934Noch keine Bewertungen
- Social Skills Rating SystemDokument12 SeitenSocial Skills Rating Systemapi-25833093460% (5)
- Unit PresentationDokument24 SeitenUnit Presentationapi-258330934Noch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Vibrant Blue Beginner Guide To Essential OilsDokument11 SeitenVibrant Blue Beginner Guide To Essential OilsTonnie RostelliNoch keine Bewertungen
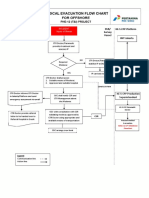
- 3-A4 - Medical Evacuation Flow Chart (Rev.0)Dokument1 Seite3-A4 - Medical Evacuation Flow Chart (Rev.0)SiskaNoch keine Bewertungen
- Covid Hospitals Yet To Get NOC From Fire Department: 20 Critically Ill Die Due To Lack of Oxygen in DelhiDokument16 SeitenCovid Hospitals Yet To Get NOC From Fire Department: 20 Critically Ill Die Due To Lack of Oxygen in DelhiblessNoch keine Bewertungen
- PsychopathiaDokument26 SeitenPsychopathiaKunal KejriwalNoch keine Bewertungen
- The Addiction Casebook - Chap 04Dokument11 SeitenThe Addiction Casebook - Chap 04Glaucia MarollaNoch keine Bewertungen
- Call The MidwifeDokument12 SeitenCall The MidwifeCecilia DemergassoNoch keine Bewertungen
- United States Food and Drug Administration (Usfda)Dokument50 SeitenUnited States Food and Drug Administration (Usfda)Hyma RamakrishnaNoch keine Bewertungen
- EUA Abiomed ImpellaLV IFU3Dokument254 SeitenEUA Abiomed ImpellaLV IFU3Angelina LeungNoch keine Bewertungen
- YMAA - List of Articles About Qigong & MeditationDokument7 SeitenYMAA - List of Articles About Qigong & MeditationnqngestionNoch keine Bewertungen
- Introduction To Clinical AssessmentDokument13 SeitenIntroduction To Clinical AssessmentnurmeenNoch keine Bewertungen
- HeelDokument4 SeitenHeelDoha EbedNoch keine Bewertungen
- Endoscopic Evaluation of Post-Fundoplication Anatomy: Esophagus (J Clarke and N Ahuja, Section Editors)Dokument8 SeitenEndoscopic Evaluation of Post-Fundoplication Anatomy: Esophagus (J Clarke and N Ahuja, Section Editors)Josseph EscobarNoch keine Bewertungen
- Complete Project PDFDokument67 SeitenComplete Project PDFRaghu Nadh100% (1)
- Kapitel 6Dokument125 SeitenKapitel 6Jai Murugesh100% (1)
- Fibromyalgia Acupressure TherapyDokument3 SeitenFibromyalgia Acupressure TherapyactoolNoch keine Bewertungen
- Family-Fasciolidae Genus: Fasciola: F. Hepatica, F. GiganticaDokument3 SeitenFamily-Fasciolidae Genus: Fasciola: F. Hepatica, F. GiganticaSumit Sharma PoudelNoch keine Bewertungen
- Social and Emotional Well Being Framework 2004-2009Dokument79 SeitenSocial and Emotional Well Being Framework 2004-2009MikeJacksonNoch keine Bewertungen
- A Fluids and ElectrolytesDokument8 SeitenA Fluids and ElectrolytesAnastasiafynnNoch keine Bewertungen
- Lasers: Effect of Laser Therapy On Chronic Osteoarthritis of The Knee in Older SubjectsDokument8 SeitenLasers: Effect of Laser Therapy On Chronic Osteoarthritis of The Knee in Older SubjectsBasith HalimNoch keine Bewertungen
- Faml360 - Final Assesment PaperDokument9 SeitenFaml360 - Final Assesment Paperapi-544647299Noch keine Bewertungen
- Individual Assignment A1 Engineering Technologist in Society Clb40002Dokument13 SeitenIndividual Assignment A1 Engineering Technologist in Society Clb40002Anonymous T7vjZG4otNoch keine Bewertungen
- Complicatii Si Sechele Tardive Dupa Tratamentul Multimodal Al GlioamelorDokument35 SeitenComplicatii Si Sechele Tardive Dupa Tratamentul Multimodal Al GlioamelorBiblioteca CSNTNoch keine Bewertungen
- Neurologic Music Therapy Improves Executive Function and Emotional Adjustment in Traumatic Brain Injury RehabilitationDokument11 SeitenNeurologic Music Therapy Improves Executive Function and Emotional Adjustment in Traumatic Brain Injury RehabilitationTlaloc GonzalezNoch keine Bewertungen
- GI PathologyDokument22 SeitenGI Pathologyzeroun24100% (5)
- Cholesteatoma Guide: Symptoms, Diagnosis and Treatment OptionsDokument9 SeitenCholesteatoma Guide: Symptoms, Diagnosis and Treatment Optionssergeantchai068Noch keine Bewertungen
- Potts DiseaseDokument8 SeitenPotts Diseaseaimeeros0% (2)
- AP2 Lab Report Lab 06Dokument4 SeitenAP2 Lab Report Lab 06kingcon420Noch keine Bewertungen
- Orange Peel MSDSDokument4 SeitenOrange Peel MSDSarvind kaushikNoch keine Bewertungen
- Q A Random - 16Dokument8 SeitenQ A Random - 16ja100% (1)
- NMC Standards For Competence For Registered NursesDokument21 SeitenNMC Standards For Competence For Registered NursesAgnieszka WaligóraNoch keine Bewertungen