Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Comparison of Common Meds For Diabetic Neuropathy: Pharmacist'S Letter / Prescriber'S LetterDokument5 SeitenComparison of Common Meds For Diabetic Neuropathy: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Noch keine Bewertungen
- 1253Dokument3 Seiten1253carramrod2Noch keine Bewertungen
- Selecting A Sulfonylurea: Pharmacist'S Letter / Prescriber'S LetterDokument3 SeitenSelecting A Sulfonylurea: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Noch keine Bewertungen
- 250803111111Dokument4 Seiten250803111111carramrod2Noch keine Bewertungen
- 1214Dokument4 Seiten1214carramrod2Noch keine Bewertungen
- 1215Dokument11 Seiten1215carramrod2Noch keine Bewertungen
- DfsefDokument4 SeitenDfsefcarramrod2Noch keine Bewertungen
- Initiation and Adjustment of Insulin Regimens For Type 2 DiabetesDokument2 SeitenInitiation and Adjustment of Insulin Regimens For Type 2 Diabetescarramrod2Noch keine Bewertungen
- Treatment of Diabetes in Women Who Are Pregnant: Pharmacist'S Letter / Prescriber'S LetterDokument5 SeitenTreatment of Diabetes in Women Who Are Pregnant: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Noch keine Bewertungen
- Thiazides and Diabetes: Pharmacist'S Letter / Prescriber'S LetterDokument2 SeitenThiazides and Diabetes: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Noch keine Bewertungen
- 1107Dokument5 Seiten1107carramrod2Noch keine Bewertungen
- 205rfqergqergDokument4 Seiten205rfqergqergcarramrod2Noch keine Bewertungen
- Proper Disposal of Expired or Unwanted DrugsDokument9 SeitenProper Disposal of Expired or Unwanted Drugscarramrod2Noch keine Bewertungen
- Prescribing For Self or FamilyDokument15 SeitenPrescribing For Self or Familycarramrod2100% (2)
- Tablet Splitting - To Split or Not To SplitDokument2 SeitenTablet Splitting - To Split or Not To Splitcarramrod2Noch keine Bewertungen
- Generic Drug VariabilityDokument5 SeitenGeneric Drug Variabilitycarramrod2Noch keine Bewertungen
- 3807Dokument2 Seiten3807carramrod2Noch keine Bewertungen
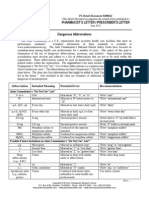
- Dangerous AbbreviationsDokument3 SeitenDangerous Abbreviationscarramrod2Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Renal Calculi Concept Map PathophysiologyDokument3 SeitenRenal Calculi Concept Map PathophysiologySharon TanveerNoch keine Bewertungen
- The Social Norms ApproachDokument7 SeitenThe Social Norms ApproachJasmine TereaNoch keine Bewertungen
- Screening ADHDDokument2 SeitenScreening ADHDPsiholog Alina Mirela CraiuNoch keine Bewertungen
- Fundamental of Nursing QuizDokument15 SeitenFundamental of Nursing QuizDr. Jayesh Patidar100% (1)
- Pertemuan 8Dokument3 SeitenPertemuan 8Furi WigitaNoch keine Bewertungen
- InBody 270Dokument27 SeitenInBody 270lee CeeNoch keine Bewertungen
- Chapter 4 MayangDokument12 SeitenChapter 4 MayangJames FulgencioNoch keine Bewertungen
- Guidelines On Aesthetic Medical Practice For Registered Medical PractitionersDokument47 SeitenGuidelines On Aesthetic Medical Practice For Registered Medical Practitionerszahisma890% (1)
- Regulatory Bodies of Nursing in India: Dr. Maheswari JaikumarDokument75 SeitenRegulatory Bodies of Nursing in India: Dr. Maheswari Jaikumarkalla sharonNoch keine Bewertungen
- Meditation and Energy HealingDokument16 SeitenMeditation and Energy HealingCristian CatalinaNoch keine Bewertungen
- Ashta Sthana ParikshaDokument35 SeitenAshta Sthana ParikshaSwanand Avinash JoshiNoch keine Bewertungen
- BioF5-4.4 Contribution of Science and Technology To Human ReproductionDokument24 SeitenBioF5-4.4 Contribution of Science and Technology To Human ReproductionteahockNoch keine Bewertungen
- GDS - Goldberg's Depression ScaleDokument2 SeitenGDS - Goldberg's Depression ScaleAnton Henry Miaga100% (1)
- Nursing Care Plan: Louise O. Reponte BSN-3CDokument12 SeitenNursing Care Plan: Louise O. Reponte BSN-3CLouise MurphyNoch keine Bewertungen
- Literature Review Network SecurityDokument8 SeitenLiterature Review Network Securityc5q8g5tz100% (1)
- DMA Ethics GuidelinesDokument51 SeitenDMA Ethics GuidelinesTesteNoch keine Bewertungen
- Adult Survivors of Childhood Trauma: Complex Trauma, Complex NeedsDokument9 SeitenAdult Survivors of Childhood Trauma: Complex Trauma, Complex NeedsPhy MedNoch keine Bewertungen
- ResearchDokument10 SeitenResearch999saitama 999Noch keine Bewertungen
- Hooper Appointment Referral PacketDokument8 SeitenHooper Appointment Referral PacketJustin RolnickNoch keine Bewertungen
- General ObjectivesDokument13 SeitenGeneral ObjectiveskevinNoch keine Bewertungen
- Medical AnimationDokument2 SeitenMedical AnimationAtellier StudiosNoch keine Bewertungen
- Disorders of The Eye LidsDokument33 SeitenDisorders of The Eye Lidsc/risaaq yuusuf ColoowNoch keine Bewertungen
- Lamotte 4493 - SDSDokument7 SeitenLamotte 4493 - SDSSyed AhmedNoch keine Bewertungen
- Homework PaperDokument12 SeitenHomework Paperapi-509662228Noch keine Bewertungen
- ทิพยมนต์กับการบำบัดโรคDokument7 Seitenทิพยมนต์กับการบำบัดโรคtachetNoch keine Bewertungen
- The Early Trauma Inventory Self Report-Short FormDokument8 SeitenThe Early Trauma Inventory Self Report-Short FormMiguel Angel Alemany NaveirasNoch keine Bewertungen
- Urinalysis and Other Body FluidsDokument64 SeitenUrinalysis and Other Body FluidsJahre Mark ToledoNoch keine Bewertungen
- SarcomaDokument2 SeitenSarcomaedrichaNoch keine Bewertungen
- Tri DoshaDokument7 SeitenTri DoshaSKNoch keine Bewertungen
- Structural Family Therapy Versus Strategic Family Therapy: A Comparative DiscussionDokument11 SeitenStructural Family Therapy Versus Strategic Family Therapy: A Comparative DiscussionDavid P Sanchez100% (8)