Das könnte Ihnen auch gefallen
- Comparison of Common Meds For Diabetic Neuropathy: Pharmacist'S Letter / Prescriber'S LetterDokument5 SeitenComparison of Common Meds For Diabetic Neuropathy: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Noch keine Bewertungen
- Selecting A Sulfonylurea: Pharmacist'S Letter / Prescriber'S LetterDokument3 SeitenSelecting A Sulfonylurea: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Noch keine Bewertungen
- 1253Dokument3 Seiten1253carramrod2Noch keine Bewertungen
- Initiation and Adjustment of Insulin Regimens For Type 2 DiabetesDokument2 SeitenInitiation and Adjustment of Insulin Regimens For Type 2 Diabetescarramrod2Noch keine Bewertungen
- Treatment of Diabetes in Women Who Are Pregnant: Pharmacist'S Letter / Prescriber'S LetterDokument5 SeitenTreatment of Diabetes in Women Who Are Pregnant: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Noch keine Bewertungen
- 1215Dokument11 Seiten1215carramrod2Noch keine Bewertungen
- 1214Dokument4 Seiten1214carramrod2Noch keine Bewertungen
- Thiazides and Diabetes: Pharmacist'S Letter / Prescriber'S LetterDokument2 SeitenThiazides and Diabetes: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Noch keine Bewertungen
- DfsefDokument4 SeitenDfsefcarramrod2Noch keine Bewertungen
- 205rfqergqergDokument4 Seiten205rfqergqergcarramrod2Noch keine Bewertungen
- Proper Disposal of Expired or Unwanted DrugsDokument9 SeitenProper Disposal of Expired or Unwanted Drugscarramrod2Noch keine Bewertungen
- 1107Dokument5 Seiten1107carramrod2Noch keine Bewertungen
- Management of Common Skin DiseasesDokument17 SeitenManagement of Common Skin Diseasescarramrod2Noch keine Bewertungen
- 3807Dokument2 Seiten3807carramrod2Noch keine Bewertungen
- Prescribing For Self or FamilyDokument15 SeitenPrescribing For Self or Familycarramrod2100% (2)
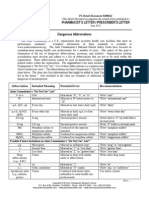
- Dangerous AbbreviationsDokument3 SeitenDangerous Abbreviationscarramrod2Noch keine Bewertungen
- Tablet Splitting - To Split or Not To SplitDokument2 SeitenTablet Splitting - To Split or Not To Splitcarramrod2Noch keine Bewertungen
- Generic Drug VariabilityDokument5 SeitenGeneric Drug Variabilitycarramrod2Noch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Garlic - Toxic & A Brain Synchronization DestroyerDokument1 SeiteGarlic - Toxic & A Brain Synchronization DestroyerJonas Sunshine CallewaertNoch keine Bewertungen
- Medical Terms in MandarinDokument17 SeitenMedical Terms in MandarinmrhoNoch keine Bewertungen
- Drug Name Indication Mode of Action Contraindications Side Effects Nursing ConsiderationsDokument3 SeitenDrug Name Indication Mode of Action Contraindications Side Effects Nursing ConsiderationsAlyssa RodriguezNoch keine Bewertungen
- Tsr-Backpain Ebook FinalDokument24 SeitenTsr-Backpain Ebook FinalRodrigo LimaNoch keine Bewertungen
- United States Complaint in Intervention in False Claims Act Lawsuits Accusing Insys Therapeutics of Paying Kickbacks and Engaging in Other Unlawful Practices to Promote Subsys, A Powerful Opioid PainkillerDokument37 SeitenUnited States Complaint in Intervention in False Claims Act Lawsuits Accusing Insys Therapeutics of Paying Kickbacks and Engaging in Other Unlawful Practices to Promote Subsys, A Powerful Opioid PainkillerBeverly Tran100% (1)
- Pancreatic Pseudocyst Laparoscopic Drainage Case ReportDokument17 SeitenPancreatic Pseudocyst Laparoscopic Drainage Case ReportrazvanccNoch keine Bewertungen
- Trigger Points Massage Therapy GuideDokument24 SeitenTrigger Points Massage Therapy GuideTaina Avramescu100% (2)
- Mastering USMLE Step 2 CS with Kaplan CasesDokument3 SeitenMastering USMLE Step 2 CS with Kaplan CasesadamNoch keine Bewertungen
- ERA System Brochure1Dokument6 SeitenERA System Brochure1Ana Massiel NarváezNoch keine Bewertungen
- Corneal Foreign Body: Causes, Symptoms & TreatmentDokument2 SeitenCorneal Foreign Body: Causes, Symptoms & Treatmentmegayani santosoNoch keine Bewertungen
- Fetal valproate syndrome review: teratogenic effects and managementDokument8 SeitenFetal valproate syndrome review: teratogenic effects and managementKumar Gavali SuryanarayanaNoch keine Bewertungen
- Asas Perancangan Rekabentuk Fasiliti Kesihatan (F)Dokument82 SeitenAsas Perancangan Rekabentuk Fasiliti Kesihatan (F)farahazuraNoch keine Bewertungen
- Bumetanide preclinical toxicity profileDokument15 SeitenBumetanide preclinical toxicity profileKrishna MahidaNoch keine Bewertungen
- 25 - Application of Isokinetics in Testing and RehabilitationDokument23 Seiten25 - Application of Isokinetics in Testing and RehabilitationCarlos GarciaNoch keine Bewertungen
- Final PaperDokument12 SeitenFinal PaperKhaled Atef ElhayesNoch keine Bewertungen
- 03 The Role of "Smart" Infusion Pumps in Patient Safety PDFDokument11 Seiten03 The Role of "Smart" Infusion Pumps in Patient Safety PDFSaravanan NallasivanNoch keine Bewertungen
- The Elements of Success:: 21 Customer Stories On Achieving Autonomous TransformationDokument34 SeitenThe Elements of Success:: 21 Customer Stories On Achieving Autonomous TransformationValenNoch keine Bewertungen
- 12Dokument5 Seiten12yeremias setyawanNoch keine Bewertungen
- Hyper Parathyroid IsmDokument7 SeitenHyper Parathyroid IsmEllene Mae Dejapa VillasisNoch keine Bewertungen
- Albuterol Sulfate Drug StudyDokument4 SeitenAlbuterol Sulfate Drug StudyFrancis Corpuz100% (1)
- KNGF Guideline For Physical Therapy in Patients With ParkinsDokument89 SeitenKNGF Guideline For Physical Therapy in Patients With ParkinsSrđan ŠarenacNoch keine Bewertungen
- 3rd Newsletter FinalDokument14 Seiten3rd Newsletter FinalBhavish RamroopNoch keine Bewertungen
- PCC EasamcDokument22 SeitenPCC EasamchusnaNoch keine Bewertungen
- Guiding Pharmacist Patient Interview ModelDokument25 SeitenGuiding Pharmacist Patient Interview ModelHumera Sarwar100% (1)
- Acute Care Final Reflective Journal 2018 - Jamie BorelDokument4 SeitenAcute Care Final Reflective Journal 2018 - Jamie Borelapi-431213859Noch keine Bewertungen
- 3.guía CLSI Documento H3 - A6Dokument56 Seiten3.guía CLSI Documento H3 - A6Majo Tovar67% (3)
- PERSONALITY DISORDERS: CLUSTERS A AND BDokument58 SeitenPERSONALITY DISORDERS: CLUSTERS A AND BJoanneMontalboNoch keine Bewertungen
- Lecture Cardio Physiotherapy 1Dokument318 SeitenLecture Cardio Physiotherapy 1Nurse GhanemNoch keine Bewertungen
- Theophylline DIDokument4 SeitenTheophylline DIamberNoch keine Bewertungen
- Acute PancreatitisDokument23 SeitenAcute PancreatitisGel Torres Galvez50% (2)