Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Dental Office Marketing PlanDokument20 SeitenDental Office Marketing PlanPalo Alto Software100% (10)
- JadaDokument14 SeitenJadaadambear213Noch keine Bewertungen
- 3-Evaluation of Human Recession Defects Treated With Coronally Advanced Flaps and Either Enamel Matrix Derivatives or Connective Tissue - Comparison of Clinical Parameters at 10Dokument10 Seiten3-Evaluation of Human Recession Defects Treated With Coronally Advanced Flaps and Either Enamel Matrix Derivatives or Connective Tissue - Comparison of Clinical Parameters at 10adambear213Noch keine Bewertungen
- Step-By-Step Instructions On The: Straumann TibrushDokument4 SeitenStep-By-Step Instructions On The: Straumann Tibrushadambear213Noch keine Bewertungen
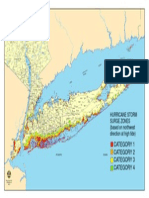
- Nys Storm Surge ZonesDokument1 SeiteNys Storm Surge Zonesadambear213Noch keine Bewertungen
- Ideas Academy Reports: and InnovationsDokument9 SeitenIdeas Academy Reports: and Innovationsadambear213Noch keine Bewertungen
- Sterile Healing Solutions FOFDokument2 SeitenSterile Healing Solutions FOFadambear213Noch keine Bewertungen
- Jop 1974 45 3 151Dokument4 SeitenJop 1974 45 3 151adambear213Noch keine Bewertungen
- Keratinized Mucosa Around Dental ImplantsDokument2 SeitenKeratinized Mucosa Around Dental Implantsadambear213Noch keine Bewertungen
- Periodontal Dictates For Esthetic Ceramometal Crowns: R - Sheldon Stein, DMDDokument11 SeitenPeriodontal Dictates For Esthetic Ceramometal Crowns: R - Sheldon Stein, DMDadambear213Noch keine Bewertungen
- 27Dokument7 Seiten27adambear213Noch keine Bewertungen
- Malpractice and Perio DiseaseDokument4 SeitenMalpractice and Perio Diseaseadambear213Noch keine Bewertungen
- Average Tooth MeasurmentsDokument1 SeiteAverage Tooth Measurmentsadambear213Noch keine Bewertungen
- CDC - Half of American Adults Have Periodontal Disease - PerioDokument3 SeitenCDC - Half of American Adults Have Periodontal Disease - Perioadambear213Noch keine Bewertungen
- Greenstein Et Tarnow 2006ddDokument11 SeitenGreenstein Et Tarnow 2006ddAnup Lal RajbahakNoch keine Bewertungen
- TISPDokument14 SeitenTISPadambear213100% (1)
- WhatsNew E OldDokument25 SeitenWhatsNew E Oldadambear213Noch keine Bewertungen
- J 1600-0757 1997 tb00094 XDokument21 SeitenJ 1600-0757 1997 tb00094 Xadambear213Noch keine Bewertungen
- Suture Surg Gut Chrom Bge FS2 4Dokument1 SeiteSuture Surg Gut Chrom Bge FS2 4adambear213Noch keine Bewertungen
- 16Dokument9 Seiten16adambear213Noch keine Bewertungen
- REVISED ASSIGNMENTS Biology and Pathology of The PeriodontiumDokument2 SeitenREVISED ASSIGNMENTS Biology and Pathology of The Periodontiumadambear213Noch keine Bewertungen
- IBR Application CDokument12 SeitenIBR Application CChris HudginsNoch keine Bewertungen
- WhatsNew EDokument37 SeitenWhatsNew Eadambear213Noch keine Bewertungen
- Sterile Healing Solutions FOFDokument2 SeitenSterile Healing Solutions FOFadambear213Noch keine Bewertungen
- Map ArenaDokument1 SeiteMap Arenaadambear213Noch keine Bewertungen
- Outscraper-2023110612255569c3 Pathology +1Dokument590 SeitenOutscraper-2023110612255569c3 Pathology +1OFC accountNoch keine Bewertungen
- Chap 9 The Health Care Delivery SystemDokument26 SeitenChap 9 The Health Care Delivery Systemjocelyn bernardoNoch keine Bewertungen
- Steroids in Chronic Subdural Hematomas SUCRE TrialDokument8 SeitenSteroids in Chronic Subdural Hematomas SUCRE TrialEdward Arthur IskandarNoch keine Bewertungen
- HB Year 1 and 2 MBBS Programme Handbook - Apr 2018Dokument149 SeitenHB Year 1 and 2 MBBS Programme Handbook - Apr 2018Peter GadielNoch keine Bewertungen
- Jennifer Tripodi ResumeDokument2 SeitenJennifer Tripodi Resumeapi-242986811Noch keine Bewertungen
- ScheduleDokument52 SeitenSchedulerohitNoch keine Bewertungen
- 2016 Issue 1Dokument86 Seiten2016 Issue 1Fareesha KhanNoch keine Bewertungen
- Phlebotomy TechniqueDokument87 SeitenPhlebotomy TechniqueJigs YumangNoch keine Bewertungen
- Ds OresolDokument2 SeitenDs OresolShannie PadillaNoch keine Bewertungen
- Philippine Obstetrical and Philippine Obstetrical and Gynecological Society (POGS), Foundation, Inc. Gynecological Society (POGS), Foundation, IncDokument51 SeitenPhilippine Obstetrical and Philippine Obstetrical and Gynecological Society (POGS), Foundation, Inc. Gynecological Society (POGS), Foundation, IncJanna Janoras ŰNoch keine Bewertungen
- Principles of Bag TechniqueDokument3 SeitenPrinciples of Bag TechniqueClare AlcoberNoch keine Bewertungen
- (24!03!2020) LKS Pembelajaran Virus Corona Nisrina Nabila Azzahra X-TEI SMK PiramidaDokument43 Seiten(24!03!2020) LKS Pembelajaran Virus Corona Nisrina Nabila Azzahra X-TEI SMK PiramidaUne NuneNoch keine Bewertungen
- Antepartum HemorrhageDokument3 SeitenAntepartum Hemorrhagenur1146Noch keine Bewertungen
- Tele Health and Tele Care Health Health and Social Care EssayDokument22 SeitenTele Health and Tele Care Health Health and Social Care EssayHND Assignment Help100% (1)
- Tuvalu Standard Treatment GuidelinesDokument401 SeitenTuvalu Standard Treatment GuidelinesportosinNoch keine Bewertungen
- More Serious Health ProblemsDokument3 SeitenMore Serious Health ProblemsYassin KhanNoch keine Bewertungen
- Care PlanDokument3 SeitenCare Planapi-381438480Noch keine Bewertungen
- Syphilis in Pregnancy: Clinical Expert SeriesDokument15 SeitenSyphilis in Pregnancy: Clinical Expert SeriesWindy MuldianiNoch keine Bewertungen
- Telepharmacy and Home Delivery Program in SpainDokument4 SeitenTelepharmacy and Home Delivery Program in SpainAthenaeum Scientific PublishersNoch keine Bewertungen
- CPR: Lifesaving Technique for Cardiac & Respiratory EmergenciesDokument5 SeitenCPR: Lifesaving Technique for Cardiac & Respiratory EmergenciesMukesh KumarNoch keine Bewertungen
- Analysis of Us Health Care PolicyDokument7 SeitenAnalysis of Us Health Care Policyapi-520841770Noch keine Bewertungen
- SIP Poster - 4Dokument1 SeiteSIP Poster - 4NCPQSWNoch keine Bewertungen
- Clostridium BotulinumDokument37 SeitenClostridium Botulinumjoevani_007Noch keine Bewertungen
- Uses of Water As Therapeutic AgentDokument3 SeitenUses of Water As Therapeutic AgentJake ArizapaNoch keine Bewertungen
- Acute Headache Guide for Emergency PhysiciansDokument6 SeitenAcute Headache Guide for Emergency PhysiciansRoselyn DawongNoch keine Bewertungen
- Guidelines For DPT Case StudyDokument7 SeitenGuidelines For DPT Case StudyHello RainbowNoch keine Bewertungen
- Director - ProfileDokument2 SeitenDirector - ProfileHimanshu GoyalNoch keine Bewertungen
- hw410 Unit 9 AssignmentDokument12 Seitenhw410 Unit 9 Assignmentapi-569132011Noch keine Bewertungen
- B-2211 Implementation of DCI Revised B.D.S. CourseDokument17 SeitenB-2211 Implementation of DCI Revised B.D.S. CourseShital KiranNoch keine Bewertungen
- Basic AudiologyDokument42 SeitenBasic Audiologyapi-3743483100% (2)