Das könnte Ihnen auch gefallen
- Surviving Cutaneous Melanoma. A Clinical Review of Follow-Up Practices, Surveillance, and Management of RecurrenceDokument14 SeitenSurviving Cutaneous Melanoma. A Clinical Review of Follow-Up Practices, Surveillance, and Management of RecurrenceNguyen DuongNoch keine Bewertungen
- New Tattoo Approaches in DermatologyDokument6 SeitenNew Tattoo Approaches in DermatologyNguyen DuongNoch keine Bewertungen
- Filler Placement and The Fat CompartmentsDokument14 SeitenFiller Placement and The Fat CompartmentsNguyen Duong100% (1)
- Innate and Intrinsic Antiviral Immunity in SkinDokument8 SeitenInnate and Intrinsic Antiviral Immunity in SkinNguyen DuongNoch keine Bewertungen
- Obstetrics and Gynecology-An Illustrated Colour TextDokument174 SeitenObstetrics and Gynecology-An Illustrated Colour TextAlina CiubotariuNoch keine Bewertungen
- Complications of Infantile HemangiomasDokument6 SeitenComplications of Infantile HemangiomasNguyen DuongNoch keine Bewertungen
- Efficacy and Safety of Intense Pulsed Light in Treatment of Melasma in Chinese PatientsDokument9 SeitenEfficacy and Safety of Intense Pulsed Light in Treatment of Melasma in Chinese PatientsNguyen DuongNoch keine Bewertungen
- 1,064-Nm Q-Switched Neodymium-Doped Yttrium Aluminum Garnet Laser and 1,550-Nm Fractionated Erbium-Doped Fiber Laser For The Treatment of Nevus of Ota in Fitzpatrick Skin Type IVDokument5 Seiten1,064-Nm Q-Switched Neodymium-Doped Yttrium Aluminum Garnet Laser and 1,550-Nm Fractionated Erbium-Doped Fiber Laser For The Treatment of Nevus of Ota in Fitzpatrick Skin Type IVNguyen Duong100% (1)
- Forehead Plasty For Facial RejuvenationDokument12 SeitenForehead Plasty For Facial RejuvenationNguyen DuongNoch keine Bewertungen
- Traditional AbdominoplastyDokument23 SeitenTraditional AbdominoplastyNguyen DuongNoch keine Bewertungen
- Aesthetic Facial ImplantsDokument21 SeitenAesthetic Facial ImplantsNguyen DuongNoch keine Bewertungen
- Endoscopic Forehead Lift. Technique and Case PresentationsDokument9 SeitenEndoscopic Forehead Lift. Technique and Case PresentationsNguyen DuongNoch keine Bewertungen
- One Hundred Cases of Endoscopic Brow LiftDokument5 SeitenOne Hundred Cases of Endoscopic Brow LiftNguyen DuongNoch keine Bewertungen
- Chapter 23 - Cosmetic Plastic SurgeryDokument24 SeitenChapter 23 - Cosmetic Plastic SurgeryNguyen DuongNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- A Study On Financial Performance of State Bank of India: April 2018Dokument6 SeitenA Study On Financial Performance of State Bank of India: April 2018priyankaNoch keine Bewertungen
- Assessment in The K To 12Dokument49 SeitenAssessment in The K To 12Alec Palcon JovenNoch keine Bewertungen
- Clinical Practice EvalDokument17 SeitenClinical Practice Evalapi-712107767Noch keine Bewertungen
- (MCQ'S) Production Planning and ControlDokument5 Seiten(MCQ'S) Production Planning and ControlHVFTOOLS HVFNoch keine Bewertungen
- Adani LTDDokument12 SeitenAdani LTDcekedNoch keine Bewertungen
- Skin LesionDokument2 SeitenSkin Lesion_carido_Noch keine Bewertungen
- Compression Ratio PDFDokument6 SeitenCompression Ratio PDFRafael LuqueNoch keine Bewertungen
- Service Manual: Compact Disc ReceiverDokument130 SeitenService Manual: Compact Disc Receiverjose luisNoch keine Bewertungen
- Hanz I para Record ArDokument591 SeitenHanz I para Record ArJuanpeGarbayoNoch keine Bewertungen
- Uml Lab ManualDokument38 SeitenUml Lab ManualcomputerstudentNoch keine Bewertungen
- Implied Volatility Forecast and Option Trading STRDokument12 SeitenImplied Volatility Forecast and Option Trading STRK P LoNoch keine Bewertungen
- NCM 101 - Health Assessment SyllabusDokument2 SeitenNCM 101 - Health Assessment SyllabusRA100% (3)
- Post-Earthquake Report On Bamboo Structures and Recommendations For Reconstruction With Bamboo On The Ecuadorian CoastDokument36 SeitenPost-Earthquake Report On Bamboo Structures and Recommendations For Reconstruction With Bamboo On The Ecuadorian CoastRUENoch keine Bewertungen
- (The American Scholar Vol. 13 Iss. 4) John Dewey - The Problem of The Liberal Arts College (1944) (10.2307 - 41206764) - Libgen - LiDokument4 Seiten(The American Scholar Vol. 13 Iss. 4) John Dewey - The Problem of The Liberal Arts College (1944) (10.2307 - 41206764) - Libgen - LiDang Tuan DungNoch keine Bewertungen
- Chirp Induced Vortices PRA v1 HighlightedDokument9 SeitenChirp Induced Vortices PRA v1 HighlightedShooboNoch keine Bewertungen
- DLL 10-11Dokument5 SeitenDLL 10-11LORIBELLE MALDEPENANoch keine Bewertungen
- C 1891622Dokument199 SeitenC 1891622api-3729284Noch keine Bewertungen
- Basic Tools in Nutrition 1Dokument10 SeitenBasic Tools in Nutrition 1Khibul LimNoch keine Bewertungen
- Prof - Ed 5 Facilitating Learner Centered Teaching Module 5 Week 5Dokument5 SeitenProf - Ed 5 Facilitating Learner Centered Teaching Module 5 Week 5Leanne Lawrence BonaobraNoch keine Bewertungen
- Building Electrification Unit 03Dokument3 SeitenBuilding Electrification Unit 03SURAJ KUMARNoch keine Bewertungen
- List of CollegesDokument2 SeitenList of Collegesbipul pandeyNoch keine Bewertungen
- Aol Act 11 RandyDokument3 SeitenAol Act 11 RandyaksanaNoch keine Bewertungen
- CDP AT FINGER PIER - StudyDokument25 SeitenCDP AT FINGER PIER - Studyd_mazieroNoch keine Bewertungen
- MIT - Sip FundamentalsDokument13 SeitenMIT - Sip Fundamentalskoalla01Noch keine Bewertungen
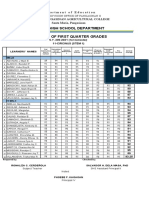
- Department of Education Senior High School 1st Quarter GradesDokument4 SeitenDepartment of Education Senior High School 1st Quarter GradesRonaliza CerdenolaNoch keine Bewertungen
- Wolfsdorf The Socratic Fallacy and The Epistimological Priority of Definitional KnowledgeDokument17 SeitenWolfsdorf The Socratic Fallacy and The Epistimological Priority of Definitional KnowledgeMaria SozopoulouNoch keine Bewertungen
- FWBD Mop 2019Dokument181 SeitenFWBD Mop 2019Aflkjael JamaelNoch keine Bewertungen
- Origin of NatyasastraDokument9 SeitenOrigin of NatyasastraArya V NairNoch keine Bewertungen
- Long-Term Contracts Loss AdjustmentDokument30 SeitenLong-Term Contracts Loss AdjustmentDina Adel DawoodNoch keine Bewertungen