Das könnte Ihnen auch gefallen
- SNL 02 Best Overall DesignDokument133 SeitenSNL 02 Best Overall DesignSNLeaderNoch keine Bewertungen
- SNL 07 Best News Series - Man Reinvented MethDokument17 SeitenSNL 07 Best News Series - Man Reinvented MethSNLeader100% (2)
- Redacted Report - NewsLeaderDokument158 SeitenRedacted Report - NewsLeaderSNLeaderNoch keine Bewertungen
- SNL 01 General ExcellenceDokument125 SeitenSNL 01 General ExcellenceSNLeaderNoch keine Bewertungen
- 2009 InvestigationDokument8 Seiten2009 InvestigationSNLeaderNoch keine Bewertungen
- SNL 07 Best News Series - Man Reinvented MethDokument17 SeitenSNL 07 Best News Series - Man Reinvented MethSNLeader100% (2)
- Missouri House Committee's Supplemental Report On Greitens InvestigationDokument5 SeitenMissouri House Committee's Supplemental Report On Greitens InvestigationKevinSeanHeldNoch keine Bewertungen
- SNL 07 Best News Series - Filed ForgottenDokument12 SeitenSNL 07 Best News Series - Filed ForgottenSNLeaderNoch keine Bewertungen
- Springfield Police DepartmentDokument1 SeiteSpringfield Police DepartmentSNLeaderNoch keine Bewertungen
- SNL 07 Best News Series - Craig Wood TrialDokument22 SeitenSNL 07 Best News Series - Craig Wood TrialSNLeaderNoch keine Bewertungen
- 2012 InvestigationDokument3 Seiten2012 InvestigationSNLeaderNoch keine Bewertungen
- SNL 07 Best News Series - Convicted BloodDokument24 SeitenSNL 07 Best News Series - Convicted BloodSNLeaderNoch keine Bewertungen
- Chart: STDs in The OzarksDokument1 SeiteChart: STDs in The OzarksSNLeaderNoch keine Bewertungen
- SNL 07 Best News Series - Convicted BloodDokument24 SeitenSNL 07 Best News Series - Convicted BloodSNLeaderNoch keine Bewertungen
- SNL 25 Best Local Business CoverageDokument24 SeitenSNL 25 Best Local Business CoverageSNLeaderNoch keine Bewertungen
- Readiness For Kindergarten 2016Dokument21 SeitenReadiness For Kindergarten 2016SNLeaderNoch keine Bewertungen
- SNL 07 Best News Series - Filed ForgottenDokument12 SeitenSNL 07 Best News Series - Filed ForgottenSNLeaderNoch keine Bewertungen
- Estrada v. City 1531-CC00465 Post Judgment OrderDokument6 SeitenEstrada v. City 1531-CC00465 Post Judgment OrderSNLeaderNoch keine Bewertungen
- SNL 17 Community Service - More To The StoryDokument21 SeitenSNL 17 Community Service - More To The StorySNLeaderNoch keine Bewertungen
- Jefferson Ave Footbridge Report - Vs EngineeringDokument4 SeitenJefferson Ave Footbridge Report - Vs EngineeringSNLeaderNoch keine Bewertungen
- Jan. 14, 1925, Edition of The Springfield RepublicanDokument10 SeitenJan. 14, 1925, Edition of The Springfield RepublicanSNLeaderNoch keine Bewertungen
- Fire Fatality HotspotDokument1 SeiteFire Fatality HotspotSNLeaderNoch keine Bewertungen
- Second Email Thread Between Greene County Commissioner Bob Cirtin and Citizen Christopher CrossDokument4 SeitenSecond Email Thread Between Greene County Commissioner Bob Cirtin and Citizen Christopher CrossSNLeaderNoch keine Bewertungen
- Email Thread Between Greene County Sheriff Jim Arnott and Citizen Christopher CrossDokument7 SeitenEmail Thread Between Greene County Sheriff Jim Arnott and Citizen Christopher CrossSNLeaderNoch keine Bewertungen
- Bass Pro Marathon RoutesDokument1 SeiteBass Pro Marathon RoutesSNLeaderNoch keine Bewertungen
- Email Thread Between Greene County Sheriff Jim Arnott and Citizen Christopher CrossDokument7 SeitenEmail Thread Between Greene County Sheriff Jim Arnott and Citizen Christopher CrossSNLeaderNoch keine Bewertungen
- 401k LawsuitDokument65 Seiten401k LawsuitSNLeaderNoch keine Bewertungen
- First Email Thread Between Greene County Commissioner Bob Cirtin and Citizen Christopher CrossDokument5 SeitenFirst Email Thread Between Greene County Commissioner Bob Cirtin and Citizen Christopher CrossSNLeaderNoch keine Bewertungen
- Examining Counties' Health: MSU's New Center Open For BusinessDokument1 SeiteExamining Counties' Health: MSU's New Center Open For BusinessSNLeaderNoch keine Bewertungen
- BatmanDokument1 SeiteBatmanSNLeaderNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- EclampsiaDokument56 SeitenEclampsiagalihtrimuninggarNoch keine Bewertungen
- CardiologyDokument88 SeitenCardiologyAlshare NisreenNoch keine Bewertungen
- 12th MCQDokument88 Seiten12th MCQRishik Kr. Sahu 'B'Noch keine Bewertungen
- OET Writing 7Dokument3 SeitenOET Writing 7fernanda1rondelli100% (1)
- Cardiology Krok 2Dokument14 SeitenCardiology Krok 2Suha AbdullahNoch keine Bewertungen
- The Metabolic Syndrome (Insulin Resistance Syndrome or Syndrome X)Dokument24 SeitenThe Metabolic Syndrome (Insulin Resistance Syndrome or Syndrome X)Bruno SchefferNoch keine Bewertungen
- 01 Hypertension - 2019 2020 PDFDokument122 Seiten01 Hypertension - 2019 2020 PDFbaraa abu sneineh100% (1)
- ESC Congress 2020: The Digital ExperienceDokument9 SeitenESC Congress 2020: The Digital ExperienceMeatus AcusticusNoch keine Bewertungen
- Managing Hypertension in PregnancyDokument59 SeitenManaging Hypertension in Pregnancykevin jonathanNoch keine Bewertungen
- Creatinine ClearanceDokument6 SeitenCreatinine ClearancedianaNoch keine Bewertungen
- 2005 Meeting AbstractsDokument122 Seiten2005 Meeting AbstractsMaria MariaNoch keine Bewertungen
- R2Dokument24 SeitenR2Nomer SenadorNoch keine Bewertungen
- Indonesian Journal of Nursing Research (IJNR) : Hubungan Kualitas Tidur Dengan Tekanan DarahDokument8 SeitenIndonesian Journal of Nursing Research (IJNR) : Hubungan Kualitas Tidur Dengan Tekanan Darahkucing menariNoch keine Bewertungen
- Preventing and Managing Hypertension in Lucban SeniorsDokument16 SeitenPreventing and Managing Hypertension in Lucban SeniorsSiena PlacinoNoch keine Bewertungen
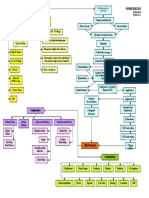
- Hypertension Concept MapDokument1 SeiteHypertension Concept Mapashleydean100% (7)
- Lexington Medical Center Heart Health InsertDokument12 SeitenLexington Medical Center Heart Health InsertLexington Medical CenterNoch keine Bewertungen
- Geriatric Pharmacotherapy PDFDokument6 SeitenGeriatric Pharmacotherapy PDFverry aswardsNoch keine Bewertungen
- Cardiac Output, Blood Flow, and Blood PressureDokument69 SeitenCardiac Output, Blood Flow, and Blood PressureUzma KhanNoch keine Bewertungen
- Respiratory Relaxation Therapy Improves Elderly Hypertension Patients' Quality of LifeDokument12 SeitenRespiratory Relaxation Therapy Improves Elderly Hypertension Patients' Quality of LifeJulianto DeviNoch keine Bewertungen
- Senam Lansia Terhadap HipertensiDokument13 SeitenSenam Lansia Terhadap HipertensiHimawanNoch keine Bewertungen
- Foot & Back Massage On BP & Sleep Quality in HTNDokument41 SeitenFoot & Back Massage On BP & Sleep Quality in HTNDr Vaishali MathapatiNoch keine Bewertungen
- High Risk Pregnancy (Notes)Dokument17 SeitenHigh Risk Pregnancy (Notes)rhenier_ilado100% (10)
- Review of New Hypertension Guidelines PDFDokument4 SeitenReview of New Hypertension Guidelines PDFOsiithaa CañaszNoch keine Bewertungen
- 3.hospital RHC Stgs - Federal Government of Somalia PDFDokument200 Seiten3.hospital RHC Stgs - Federal Government of Somalia PDFFaisal mohammed AbdullahiNoch keine Bewertungen
- Pengaruh Pemberian Jus Belimbing Manis Terhadap Penurunan Tekanan Darah Pada Penderita Hipertensi Di Panti Werdha Bina Bhakti Serpong TAHUN 2018Dokument17 SeitenPengaruh Pemberian Jus Belimbing Manis Terhadap Penurunan Tekanan Darah Pada Penderita Hipertensi Di Panti Werdha Bina Bhakti Serpong TAHUN 2018Siti SugiartiNoch keine Bewertungen
- Nursing Care Plan - Urban DistrictDokument4 SeitenNursing Care Plan - Urban DistrictYjah Cheimira ASEBONoch keine Bewertungen
- Paradise TrialDokument26 SeitenParadise TrialMiguel Martinez DuranNoch keine Bewertungen
- Walker V Good Shepherd CHRONOLOGYDokument34 SeitenWalker V Good Shepherd CHRONOLOGYMiddle CNoch keine Bewertungen
- Understanding and Treating Uchcha Raktachapa (Hypertension) in Perspective of Vidhishonitiya Adhyaya of Charaka Samhita - A Clinical ReviewDokument11 SeitenUnderstanding and Treating Uchcha Raktachapa (Hypertension) in Perspective of Vidhishonitiya Adhyaya of Charaka Samhita - A Clinical ReviewBinal PatelNoch keine Bewertungen
- Practical Cardiology An Approach To The Management of Problems in Cardiology (PDFDrive)Dokument405 SeitenPractical Cardiology An Approach To The Management of Problems in Cardiology (PDFDrive)hendratj90Noch keine Bewertungen