Das könnte Ihnen auch gefallen
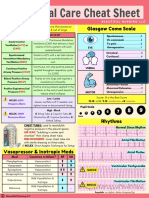
- Critical Care Cheat Sheet FreebieDokument2 SeitenCritical Care Cheat Sheet FreebieJeshan Yanong Beltran100% (1)
- Breath Sounds Incredibly EasyDokument4 SeitenBreath Sounds Incredibly EasyMatthew Ryan100% (3)
- NCP Ineffective Airway ClearanceDokument5 SeitenNCP Ineffective Airway ClearanceEmm Estipona HaoNoch keine Bewertungen
- Respiratory Physiology: Ventilation Perfusion DiffusionDokument6 SeitenRespiratory Physiology: Ventilation Perfusion DiffusionShiara Ruth EdrosoloNoch keine Bewertungen
- PT in Respiratory Care EvbDokument562 SeitenPT in Respiratory Care EvbaeeraadeevaNoch keine Bewertungen
- Ventilator Waveforms and The Physiology of Pressure Support PDFDokument21 SeitenVentilator Waveforms and The Physiology of Pressure Support PDFRoberto RamirezNoch keine Bewertungen
- Nclex review: Pneumonia, COPD, Asthma StudyDokument11 SeitenNclex review: Pneumonia, COPD, Asthma Studymj078Noch keine Bewertungen
- Chronic Obstructive Pulmonary DiseaseDokument18 SeitenChronic Obstructive Pulmonary DiseaseMaryam BajwaNoch keine Bewertungen
- Respiratory Distress SyndromeDokument30 SeitenRespiratory Distress SyndromeDennis MiritiNoch keine Bewertungen
- Measuring Lung Capacity Using Portable SpirometerDokument11 SeitenMeasuring Lung Capacity Using Portable SpirometerTootsie88% (16)
- Seizures in ChildrenDokument21 SeitenSeizures in ChildrenTera SurbaktiNoch keine Bewertungen
- Test Bank For Mechanical Ventilation 7th Edition J M CairoDokument13 SeitenTest Bank For Mechanical Ventilation 7th Edition J M CairocalliopesilasaagyNoch keine Bewertungen
- Lower Respiratory Tract InfectionDokument8 SeitenLower Respiratory Tract InfectionRarasRachmandiarNoch keine Bewertungen
- "A Study ON Chronic Obstructive Pulmonary Diseases": Ananta Institute of Medical Sciences and ResearchDokument13 Seiten"A Study ON Chronic Obstructive Pulmonary Diseases": Ananta Institute of Medical Sciences and ResearchHamid RazaNoch keine Bewertungen
- Protocol 2Dokument14 SeitenProtocol 2Hamid RazaNoch keine Bewertungen
- 01585-2021 FullDokument156 Seiten01585-2021 FullywtmyxpezickztrkcfNoch keine Bewertungen
- BODEXDokument8 SeitenBODEXLindsey KaufmanNoch keine Bewertungen
- Diffusing Capacity of Carbon Monoxide in Assessment of COPD: Original ResearchDokument9 SeitenDiffusing Capacity of Carbon Monoxide in Assessment of COPD: Original ResearchKlinikdr RIDHANoch keine Bewertungen
- 1 s2.0 S2452247318303200 MainDokument5 Seiten1 s2.0 S2452247318303200 Mainputujunidtd13Noch keine Bewertungen
- The Impact of COPD On Health Status: Findings From The BOLD StudyDokument12 SeitenThe Impact of COPD On Health Status: Findings From The BOLD StudyAnonymous Cpmq1iHHNoch keine Bewertungen
- Long-term telemonitoring effects on healthcareDokument9 SeitenLong-term telemonitoring effects on healthcaremerlinakisNoch keine Bewertungen
- Primary Care Summary of The British Thoracic Society Guidelines For The Management of Community Acquired Pneumonia in Adults: 2009 UpdateDokument7 SeitenPrimary Care Summary of The British Thoracic Society Guidelines For The Management of Community Acquired Pneumonia in Adults: 2009 UpdateMusyfiqoh TusholehahNoch keine Bewertungen
- JCOPDF 2015 0172 BerryDokument13 SeitenJCOPDF 2015 0172 BerrydhilaidrisNoch keine Bewertungen
- JR 2 CopdDokument6 SeitenJR 2 CopdDoc AwaNoch keine Bewertungen
- Scoring System CopdDokument9 SeitenScoring System CopdAnty FftNoch keine Bewertungen
- Print 1Dokument8 SeitenPrint 1Zaura Meliana MulyadiNoch keine Bewertungen
- Key Points on Diagnosing and Assessing Severity of COPDDokument12 SeitenKey Points on Diagnosing and Assessing Severity of COPDfallenczarNoch keine Bewertungen
- CCRPM 2011 001 PDFDokument5 SeitenCCRPM 2011 001 PDFAlexandria Firdaus Al-farisyNoch keine Bewertungen
- Predictive Value of Red Blood Cell Distribution Width in ChronicDokument8 SeitenPredictive Value of Red Blood Cell Distribution Width in ChronicAndreea MoalesNoch keine Bewertungen
- Jurnal Perawatan PaliatifDokument16 SeitenJurnal Perawatan Paliatifnurwanda hamidaNoch keine Bewertungen
- The Modified Medical Research Council Scale For The Assessment of Dyspnea in Daily Living in Obesity: A Pilot StudyDokument7 SeitenThe Modified Medical Research Council Scale For The Assessment of Dyspnea in Daily Living in Obesity: A Pilot StudyArizal AbdullahNoch keine Bewertungen
- Serum Surfactant Protein D Is Steroid Sensitive and Associated With Exacerbations of COPDDokument8 SeitenSerum Surfactant Protein D Is Steroid Sensitive and Associated With Exacerbations of COPDPatrick RamosNoch keine Bewertungen
- Relationship Between Lung Functions and Extend of Emphysema in Patients With Chronic Obstructive Pulmonary Disease 2161 105X.1000191Dokument5 SeitenRelationship Between Lung Functions and Extend of Emphysema in Patients With Chronic Obstructive Pulmonary Disease 2161 105X.1000191Trhy Rahyou MarbaniatyNoch keine Bewertungen
- Management of COPD Exacerbations in Primary Care: A Clinical Cohort StudyDokument7 SeitenManagement of COPD Exacerbations in Primary Care: A Clinical Cohort StudyNurusshiami KhairatiNoch keine Bewertungen
- Artículo PulmonarDokument9 SeitenArtículo PulmonarSamuel GasparNoch keine Bewertungen
- PJMS 34 1408Dokument4 SeitenPJMS 34 1408Tayyaba RahatNoch keine Bewertungen
- Chest: High Prevalence of Undiagnosed Airfl Ow Limitation in Patients With Cardiovascular DiseaseDokument8 SeitenChest: High Prevalence of Undiagnosed Airfl Ow Limitation in Patients With Cardiovascular DiseaseRoberto Enrique Valdebenito RuizNoch keine Bewertungen
- RCCM 202212-2300ocDokument14 SeitenRCCM 202212-2300ocLucas PereiraNoch keine Bewertungen
- Relationship Between Extravascular Lung Water and Severity Categories of Acute Respiratory Distress Syndrome by The Berlin DefinitionDokument9 SeitenRelationship Between Extravascular Lung Water and Severity Categories of Acute Respiratory Distress Syndrome by The Berlin DefinitionVictor Euclides Briones MoralesNoch keine Bewertungen
- ContentServer 13 PDFDokument10 SeitenContentServer 13 PDFFerdy LainsamputtyNoch keine Bewertungen
- ContentServer 13 PDFDokument10 SeitenContentServer 13 PDFFerdy LainsamputtyNoch keine Bewertungen
- PESI Critical Care 2005Dokument6 SeitenPESI Critical Care 2005Rocio Méndez FrancoNoch keine Bewertungen
- In-home pulmonary telerehabilitation via telehealth improves COPD outcomesDokument10 SeitenIn-home pulmonary telerehabilitation via telehealth improves COPD outcomesNica AuliaNoch keine Bewertungen
- TRD 70 323 1Dokument7 SeitenTRD 70 323 1Nurul Ummah NuNoch keine Bewertungen
- Copd Nihilismo BuenisimoDokument8 SeitenCopd Nihilismo BuenisimoJose Lopez FuentesNoch keine Bewertungen
- UK cystic fibrosis patients prefer forced techniques and oscillating PEP for airway clearanceDokument25 SeitenUK cystic fibrosis patients prefer forced techniques and oscillating PEP for airway clearancePaula UrsuNoch keine Bewertungen
- COPD Clinical Management Review Provides GuidanceDokument11 SeitenCOPD Clinical Management Review Provides GuidanceAlejandro Kanito Alvarez SNoch keine Bewertungen
- Copd 1Dokument8 SeitenCopd 1Meinita M.DNoch keine Bewertungen
- Antibiotics 02 00001Dokument10 SeitenAntibiotics 02 00001Jenny AlmagroNoch keine Bewertungen
- Artificial Intelligence Techniques in Chronic Condition Lung DiseaseDokument14 SeitenArtificial Intelligence Techniques in Chronic Condition Lung DiseaseNexgen TechnologyNoch keine Bewertungen
- 1806 3756 Jbpneu 48 01 E20210371Dokument11 Seiten1806 3756 Jbpneu 48 01 E20210371cronoss21Noch keine Bewertungen
- IJC - Smokingcessationmanuscript - Accepted VersionDokument18 SeitenIJC - Smokingcessationmanuscript - Accepted VersionUnderdog EsportNoch keine Bewertungen
- Diagnosing Pneumonia in Patients With Acute Cough: Clinical Judgment Compared To Chest RadiographyDokument7 SeitenDiagnosing Pneumonia in Patients With Acute Cough: Clinical Judgment Compared To Chest RadiographyCaptain NarongNoch keine Bewertungen
- 105 FullDokument7 Seiten105 FullMohamad Fiqih ArrachmanNoch keine Bewertungen
- Sarcoidoza Ers Ghid - FullDokument251 SeitenSarcoidoza Ers Ghid - FullCătălina BlajinNoch keine Bewertungen
- 1 s2.0 S2531043718301107 MainDokument8 Seiten1 s2.0 S2531043718301107 MainCraniolyne RefianNoch keine Bewertungen
- COPD RehabilitationDokument12 SeitenCOPD RehabilitationharbiNoch keine Bewertungen
- Jur Nal Reading 1Dokument11 SeitenJur Nal Reading 1Lalu Ryan NovariNoch keine Bewertungen
- MakananDokument8 SeitenMakananAnonymous VXZymiNoch keine Bewertungen
- Nonpharmacological Treatment For Patients With Nontuberculous Mycobacterial Lung DiseaseDokument9 SeitenNonpharmacological Treatment For Patients With Nontuberculous Mycobacterial Lung DiseaseskoamdaskondiajosNoch keine Bewertungen
- Early ViewDokument34 SeitenEarly Viewyesid urregoNoch keine Bewertungen
- Pertanyaan 7Dokument14 SeitenPertanyaan 7WicakNoch keine Bewertungen
- COPD Readmission Risk FactorsDokument19 SeitenCOPD Readmission Risk FactorsAmit ShrivastavNoch keine Bewertungen
- Gold Copd 2017Dokument4 SeitenGold Copd 2017ChrisNoch keine Bewertungen
- Efficacy and Safety of Acupoint Autohemotherapy in PDFDokument5 SeitenEfficacy and Safety of Acupoint Autohemotherapy in PDFtizziana carollaNoch keine Bewertungen
- Peak Flow Meter 3Dokument7 SeitenPeak Flow Meter 3Anushree DatarNoch keine Bewertungen
- Laboratory Tests For Pneumonia in General Practice The Diagnostic Values Depend On The Duration of IllnessDokument8 SeitenLaboratory Tests For Pneumonia in General Practice The Diagnostic Values Depend On The Duration of IllnesskaeranNoch keine Bewertungen
- PDF (8) JurnalDokument11 SeitenPDF (8) JurnalIcha Chaphedech hildantraNoch keine Bewertungen
- Rehabilitasi CopdDokument8 SeitenRehabilitasi CopdHenny RahmawatiNoch keine Bewertungen
- Print PDFDokument19 SeitenPrint PDFMohamed Saeed El KhayatNoch keine Bewertungen
- Essentials in Lung TransplantationVon EverandEssentials in Lung TransplantationAllan R. GlanvilleNoch keine Bewertungen
- Mortuary GDokument1 SeiteMortuary GArizal AbdullahNoch keine Bewertungen
- Diagnosis and Management of Epilepsies in Children and Young PeopleDokument2 SeitenDiagnosis and Management of Epilepsies in Children and Young PeopleArizal AbdullahNoch keine Bewertungen
- Mortuary DDokument1 SeiteMortuary DArizal AbdullahNoch keine Bewertungen
- Mortuary eDokument1 SeiteMortuary eArizal AbdullahNoch keine Bewertungen
- CHAPTER III-case Report v1.0Dokument7 SeitenCHAPTER III-case Report v1.0Arizal AbdullahNoch keine Bewertungen
- Mortuary FDokument1 SeiteMortuary FArizal AbdullahNoch keine Bewertungen
- Mortuary BDokument1 SeiteMortuary BArizal AbdullahNoch keine Bewertungen
- Chapter 2: Fuel Utilization and Muscle Metabolism During ExerciseDokument14 SeitenChapter 2: Fuel Utilization and Muscle Metabolism During ExerciseArizal AbdullahNoch keine Bewertungen
- Heart FailureDokument14 SeitenHeart FailureArizal AbdullahNoch keine Bewertungen
- Mortuary CDokument1 SeiteMortuary CArizal AbdullahNoch keine Bewertungen
- 735 951 1 PB PDFDokument9 Seiten735 951 1 PB PDFArizal AbdullahNoch keine Bewertungen
- Jugular Vena PressureDokument5 SeitenJugular Vena PressureArizal AbdullahNoch keine Bewertungen
- Mortuary ADokument1 SeiteMortuary AArizal AbdullahNoch keine Bewertungen
- Tukar BDokument1 SeiteTukar BArizal AbdullahNoch keine Bewertungen
- 33 3583 PDFDokument5 Seiten33 3583 PDFArizal AbdullahNoch keine Bewertungen
- Tukar CDokument1 SeiteTukar CArizal AbdullahNoch keine Bewertungen
- Hemorrhoidsummary PDFDokument6 SeitenHemorrhoidsummary PDFArizal AbdullahNoch keine Bewertungen
- Diagnosing and Managing Common Anorectal IssuesDokument60 SeitenDiagnosing and Managing Common Anorectal IssuesArizal Abdullah100% (1)
- Hemorrhoids: What Are Hemorrhoids? What Are The Symptoms of Hemorrhoids?Dokument6 SeitenHemorrhoids: What Are Hemorrhoids? What Are The Symptoms of Hemorrhoids?Devina NugrohoNoch keine Bewertungen
- Descriptive Epidemiology1Dokument16 SeitenDescriptive Epidemiology1Arizal AbdullahNoch keine Bewertungen
- Clinical Review of Haemorrhoid ManagementDokument4 SeitenClinical Review of Haemorrhoid ManagementLucky PratamaNoch keine Bewertungen
- Villalba PDFDokument3 SeitenVillalba PDFArizal AbdullahNoch keine Bewertungen
- Jurnal Hemoroid 1 PDFDokument23 SeitenJurnal Hemoroid 1 PDFArizal AbdullahNoch keine Bewertungen
- STG Agiolax 1Dokument10 SeitenSTG Agiolax 1lingnoiNoch keine Bewertungen
- 009 6565am0709 53 65Dokument13 Seiten009 6565am0709 53 65Tri Rahma Yani YawatiNoch keine Bewertungen
- WhichTreatmentsBestHemorrhoids PDFDokument2 SeitenWhichTreatmentsBestHemorrhoids PDFArizal AbdullahNoch keine Bewertungen
- CH34 PDFDokument7 SeitenCH34 PDFArizal AbdullahNoch keine Bewertungen
- HemorrhoidDokument6 SeitenHemorrhoidMuftiNoch keine Bewertungen
- 6525 PDFDokument6 Seiten6525 PDFArizal AbdullahNoch keine Bewertungen
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDokument3 SeitenSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNoch keine Bewertungen
- Administering Oxygen by Cannula/Face Mask/Face TentDokument4 SeitenAdministering Oxygen by Cannula/Face Mask/Face TentLixa Mae Cawal-oNoch keine Bewertungen
- Plan of Care For Ineffective Air Way 1Dokument6 SeitenPlan of Care For Ineffective Air Way 1LisaNoch keine Bewertungen
- Our 4-In-1 Device.: Fabian HFODokument9 SeitenOur 4-In-1 Device.: Fabian HFOLeevan BauNoch keine Bewertungen
- Ehs Hospitals All StatesDokument85 SeitenEhs Hospitals All Statesnaiduu497Noch keine Bewertungen
- Treatment of Acute BronchitisDokument3 SeitenTreatment of Acute BronchitisjokosudibyoNoch keine Bewertungen
- Interstitial Pneumonia With Autoimmune Features (IPAF) : Interesting CaseDokument10 SeitenInterstitial Pneumonia With Autoimmune Features (IPAF) : Interesting CaseSilp SatjawattanavimolNoch keine Bewertungen
- Body Plethysmography e Its Principles and Clinical Use: ReviewDokument13 SeitenBody Plethysmography e Its Principles and Clinical Use: ReviewfandiroziNoch keine Bewertungen
- Mendelson's SyndromeDokument17 SeitenMendelson's SyndromeMeena ViswaNoch keine Bewertungen
- BronchiolitisDokument5 SeitenBronchiolitisreshianeNoch keine Bewertungen
- Carganilla - Pathophysiology - Week 1Dokument4 SeitenCarganilla - Pathophysiology - Week 1Marjorie CarganillaNoch keine Bewertungen
- Ineffective Airway ClearanceDokument10 SeitenIneffective Airway ClearanceHannah VueltaNoch keine Bewertungen
- BronchiolitisDokument4 SeitenBronchiolitistingtingcrazyNoch keine Bewertungen
- BMCMedicalReportSummaryMarquezSleepStudyDokument7 SeitenBMCMedicalReportSummaryMarquezSleepStudyDamian GriffoNoch keine Bewertungen
- Niv BK 9051941 EnusDokument84 SeitenNiv BK 9051941 EnusmatijahNoch keine Bewertungen
- "Assessing Respirations": Prepared By: Marie Cecille Liberty S. VarillaDokument11 Seiten"Assessing Respirations": Prepared By: Marie Cecille Liberty S. VarillaMarie Cecille Soliven VarillaNoch keine Bewertungen
- Cues/Clues S - "Nahihirapan Ako Huminga Lalo Na Kapag Tanghali", AsDokument3 SeitenCues/Clues S - "Nahihirapan Ako Huminga Lalo Na Kapag Tanghali", Astito edNoch keine Bewertungen
- QUIZ ROUND-2 ASTHMA RAPID FIRE QUESTIONSDokument58 SeitenQUIZ ROUND-2 ASTHMA RAPID FIRE QUESTIONSSwati SharmaNoch keine Bewertungen
- 42 Respiratory Insufficiency-Pathophysiology, Diagnosis, Oxygen TherapyDokument73 Seiten42 Respiratory Insufficiency-Pathophysiology, Diagnosis, Oxygen TherapyLaila AcehNoch keine Bewertungen