Beruflich Dokumente
Kultur Dokumente
Basic Life Support Protocol Book
Hochgeladen von
Anonymous hvOuCjOriginalbeschreibung:
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Basic Life Support Protocol Book
Hochgeladen von
Anonymous hvOuCjCopyright:
Verfügbare Formate
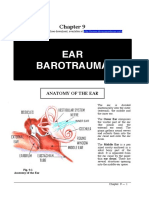
Basic Life Support
Pre-Hospital
Treatment Protocols
2nd Edition
Emergency Medical Services
South Dakota Department of Health
600 East Capitol Avenue
Pierre, South Dakota 57501-2536
http://www.state.sd.us/doh/ems/_index.htm
i
1,500 copies printed at a cost of $1.36 per document.
ii
i
Introduction
The Pre-hospital Treatment Protocols were developed to establish standards of care which are consistent
throughout the state of South Dakota, and to provide the EMS provider with a quick field reference.
Users of these protocols are assumed to have knowledge of the more detailed and basic patient care
principles found in EMS textbooks and literature appropriate to the EMS provider's level of certification.
These protocols are intended to reflect the current treatment guidelines for Basic Life Support Pre-
hospital Care. These protocols are not intended to be absolute treatment doctrines, but rather guidelines
which have sufficient flexibility to meet the complex cases presented to the Emergency Medical
Technician in the field.
The South Dakota Pre-hospital Treatment Protocols, First Edition was developed by Presentation Health
System and Don J ones, BS, NREMT-P, EMS Education Coordinator at McKennan Hospital, Sioux Falls,
South Dakota. Funding provided by the South Dakota Department of Health, Office of Rural Health,
through the Essential Access Community Hospital Grant Program administered by the Health Care
Financing Administration.
The South Dakota Pre-hospital Treatment Protocols, Second Edition, was revised and updated by
Rhonda Bonnema, NREMT-P, EMS Educator. Revision supported by McKennan Health Services, Sioux
Falls, South Dakota. Pediatric protocols supported in part by Project No. MCH-464001-03 from the
Emergency Medical Services for Children Program (Section 1910, U.S. PHS Act), HRSA, DHHS.
Revised J une, 1997
ii
Table of Contents
Trauma Protocols
Trauma Protocol #1: Assessment Priorities.......................................................................................... 1
Trauma Protocol #2: Trauma Assessment and Treatment................................................................... 4
Trauma Protocol #3: Trauma Triage Criteria........................................................................................ 5
Trauma Protocol #4: Head/Neck/Spine Injuries.................................................................................... 7
Trauma Protocol #5: Chest Injuries ...................................................................................................... 9
Trauma Protocol #6: Abdominal Injuries...............................................................................................10
Trauma Protocol #7: Extremity Injuries.................................................................................................11
Trauma Protocol #8: Amputations ........................................................................................................12
Trauma Protocol #9: Bleeding (External)..............................................................................................13
Trauma Protocol #10: Burns...................................................................................................................14
Trauma Protocol #11: Shock/Hypoperfusion..........................................................................................16
Trauma Protocol #12: Sexual Assault.....................................................................................................17
Trauma Protocol #13: Near Drowning....................................................................................................18
Medical Protocols
Medical Protocol #14: Medical Assessment...........................................................................................19
Medical Protocol #15: Abdominal Pain...................................................................................................20
Medical Protocol #16: Anaphylaxis.........................................................................................................21
Medical Protocol #16b: Epinephrine Auto-Injector..................................................................................22
Medical Protocol #17: Cardiopulmonary Resuscitation (CPR)...............................................................24
Medical Protocol #18: Cerebrovascular Accident - Stroke.....................................................................27
Medical Protocol #19: Chest Pain...........................................................................................................28
Medical Protocol #19b: Nitroglycerin......................................................................................................29
Medical Protocol #20: Childbirth.............................................................................................................31
Medical Protocol #21: Cold Emergencies...............................................................................................34
Medical Protocol #22: Diabetic Emergencies .........................................................................................36
Medical Protocol #22b: Oral Glucose.....................................................................................................37
Medical Protocol #23: Dyspnea (Difficulty Breathing) ............................................................................38
Medical Protocol #23b: Prescribed Inhaler.............................................................................................40
Medical Protocol #24: Heat Emergencies...............................................................................................42
Medical Protocol #25: Poisonings..........................................................................................................43
Medical Protocol #25b: Activated Charcoal............................................................................................45
Medical Protocol #26: Psychiatric Emergencies.....................................................................................47
Medical Protocol #27: Seizures ..............................................................................................................48
Medical Protocol #28: Unconscious Patient. ..........................................................................................50
References
Reference #29: APGAR Scale................................................................................................................51
Reference #30: Burn Chart.....................................................................................................................52
Reference #31: Diabetes Fact Sheet......................................................................................................53
Reference #32: Glasgow Coma Scale....................................................................................................54
Reference #33: MAST/PASG .................................................................................................................55
Reference #34: O
2
Administration Chart.................................................................................................56
Reference #35: Helpful Mnemonics........................................................................................................58
Reference #36: Radio/Phone Consultation............................................................................................59
Reference #37: Splints............................................................................................................................60
Reference #38: Vital Signs .....................................................................................................................61
Reference #39: Self-Protection and Personal Safety.............................................................................62
iii
References (continued)
Reference #40: Pulse Oximetry..............................................................................................................63
Reference #41: Semi-Automatic External Dibrillation (AED)..................................................................64
Reference #42: Blood or Body Fluids Exposure.....................................................................................65
Reference #43: Unusual or Rare Infectious Diseases Exposure...........................................................66
Pediatric Protocols
Pediatric Protocol #44: General Considerations.....................................................................................67
Pediatric Protocol #45: Altered Mental Status ........................................................................................69
Pediatric Protocol #46: Child Abuse.......................................................................................................70
Pediatric Protocol #47: Fever/Hyperthermia...........................................................................................72
Pediatric Protocol #48: Respiratory Distress ..........................................................................................73
Pediatric Protocol #49: Seizures.............................................................................................................75
Pediatric Protocol #50: Trauma..............................................................................................................76
iv
Trauma Protocol #1: Assessment Priorities
Scene Size-Up
1. Take body substance isolation precautions (BSI).
2. Determine if the scene is safe for you, the patient, your team members, and bystanders.
a. If the scene is not safe, make it safe.
3. Determine the mechanism of injury or nature of illness.
4. Determine the total number of patients.
a. If there are too many patients for one unit to handle, call for additional help and begin
triage.
5. Request other resources (fire, rescue, law enforcement) and activate ALS as needed.
6. If trauma patient, stabilize cervical spine.
Initial Assessment
1. Form a general impression of the patient.
a. Presence of life-threatening injuries or signs/symptoms.
b. Patient's age and sex.
2. Assess level of consciousness.
3. Assess the airway.
a. Open the airway as needed with the appropriate technique; head tilt-chin lift for medical
patients; jaw thrust for trauma patients.
b. Consider suctioning and the use of airway adjuncts; i.e., oropharyngeal or
nasopharyngeal airways.
4. Assess adequacy of breathing.
a. Administer oxygen and assess ventilations as needed.
5. Assess circulatory status.
a. Assess rate and strength of radial and carotid pulses.
b. Initiate CPR and use of the AED as appropriate.
c. Assess skin color, condition, and temperature.
d. Assess for and control major bleeding.
6. Identify priority patients and make transport decision.
1
Focused History and Physical Exam
1. Trauma patients. (See to Trauma Protocol #2, page 4.)
2. Medical patients. (See to Medical Protocol #14, page 19.)
Detailed Physical Exam
On low priority patients, this is done on the scene. On high priority patients, this is done in the ambulance
enroute to the hospital.
1. Assess the head and face for DCAP-BTLS.
a. Check for Battles sign and raccoon eyes.
b. Check ears, nose, and mouth for drainage of blood/fluids.
c. Assess the eyes, checking pupils for size, equality, and reactivity.
2. Assess the neck for DCAP-BTLS and jugular vein distention and tracheal deviation.
3. Assess the chest for DCAP-BTLS and paradoxical motion.
a. Auscultate lung sounds.
4. Assess the abdomen for DCAP-BTLS and rigidity/distention.
5. Assess the pelvis for DCAP-BTLS and stability. (If previous complaint of pelvic pain, do not
assess.)
6. Assess the genitalia/perineum as needed.
7. Assess each extremity for DCAP-BTLS and CMS (circulation, movement, and sensation).
8. Logroll the patient and assess the posterior of the body for DCAP-BTLS.
a. If the patient is on a backboard, do not do this assessment.
9. Manage injuries per specific protocol.
10. Re-assess vital signs.
Ongoing Assessment
This assessment is done every 15 minutes for stable patients, and every 5 minutes for unstable patients.
1. Repeat Initial Assessment.
2. Re-assess vital signs.
3. Repeat assessment of each injury/complaint found during previous assessments.
4. Check each intervention done for the patient; i.e., oxygen, cervical collar, bandages, splints, etc.
2
Notes:
D - Deformities B - Burns
C - Contusions T - Tenderness
A - Abrasions L - Lacerations
P - Penetrations/Punctures S - Swelling
3
Trauma Protocol #2: Trauma Assessment and Treatment
1. Complete Scene Size-Up and Initial Assessment. (See Trauma Protocol #1, page 1.)
2. Reconsider mechanism of injury.
3. If minor mechanism of injury and minor injuries
a. Assess injuries based on chief complaint.
b. Assess baseline vital signs.
c. Assess the SAMPLE history. (See Reference #35, page 58.)
4. If major mechanism of injury and/or major injuries, perform rapid trauma assessment
a. Continue stabilization of cervical spine and re-assess ABCs.
b. Rapidly assess head and neck for DCAP-BTLS.
1) Assess the neck for jugular vein distention and tracheal deviation.
2) Apply a cervical collar.
c. Rapidly assess the chest for DCAP-BTLS and paradoxical motion. Auscultate lung
sounds.
1) If found, manually seal sucking chest wounds and stabilize flail segments.
d. Rapidly assess abdomen for DCAP-BTLS and rigidity/distention.
e. Rapidly assess pelvis for DCAP-BTLS and stability.
1) If patient is complaining of pelvic pain, do not assess.
f. Rapidly assess each extremity for DCAP-BTLS and CMS (circulation, movement, and
sensation).
g. Logroll the patient and assess the posterior of the body for DCAP-BTLS.
1) Logroll onto a backboard and secure torso/extremities with straps and head with
head blocks or tape and towel rolls.
h. Obtain baseline vital signs and SAMPLE history. (See Reference #35, page 58.)
i. Move patient to the ambulance, go to the hospital, and do Detailed Physical Exam.
Notes:
D - Deformities B - Burns
C - Contusions T - Tenderness
A - Abrasions L - Lacerations
P - Penetrations/Puncture S - Swelling
4
Trauma Protocol #3: Trauma Triage Criteria
Suggested Guidelines for Requesting Advanced Life Support
Physiological
1. Systolic BP <90.
2. Respiratory Distress - Rate <10 or >29.
3. Altered mental status, or Glasgow coma scale <14. (See Reference #32, page 54.)
Anatomical
1. Flail chest.
2. Two or more long bone fractures (humerus, femur).
3. Significant penetrating injury to head, neck, torso or groin.
4. Trauma combined with >10% burns in same body area.
5. Burns to face or airway.
6. Amputation proximal to the wrist or ankle.
7. Paralysis of any limb.
8. Pelvic fractures.
Mechanism
1. Extrication from vehicle >20 minutes.
2. Death of any occupant in the patient's vehicle.
3. Ejection of patient from vehicle.
4. Fall >20 feet.
5. Pedestrian struck at speed >5 mph.
6. Motorcycle accident >20 mph.
7. Evidence of high impact; i.e., rollover, major deformity (20" or more) to vehicle, passenger
compartment intrusion >12".
8. Crash speed (change in velocity) of 20 mph or more.
Comorbid Factors (These increase the possibility of complications from trauma.)
1. Age <5 or >55.
5
2. Pregnancy.
3. Pre-existing medical problems.
4. Extremes of environment.
6
Trauma Protocol #4: Head/Neck/Spine Injuries
Assessment
1. DO NOT HYPEREXTEND NECK.
2. Perform Rapid Trauma Assessment. (See Trauma Protocol #2, page 4.) Be sure to note
mechanism of injury.
3. Assume cervical spine injury to be present in all trauma patients.
4. Perform neurological exam assessing level of consciousness.
A - Patient is alert
V - Patient responds to voice stimuli
P - Patient responds to painful stimuli
U - Patient is unresponsive
See Glasgow coma scale. (See Reference #32, page 54.)
See Trauma score. (See Reference #32, page 54.)
5. Obtain history (i.e., helmet or seat belt use) and level of consciousness since injury.
6. Note cerebrospinal fluid from ears, nose, mouth.
7. Check for associated injuries.
Comparison of Vital Signs in Shock and Head Injury
Vital Signs Shock Head Injury
Blood Pressure Decreased Increased
Pulse Increased Decreased
Respiration Increased Decreased
Level of Consciousness Decreased Decreased
Treatment
1. Secure airway per spine injury protocol.
2. Administer 100% oxygen via non-rebreather mask. If ventilation assistance is needed, bag-
valve- mask with reservoir (100% O
2
) at 24 times per minute. (Remember to have suction
immediately available).
3. Realign neck to a neutral, in-line position unless resistance is met.
4. MANUALLY stabilize head, neck and spine until secured on appropriate device. DO NOT
APPLY TRACTION.
7
5. Continuously monitor and record all observations.
6. If shock is present, see Trauma Protocol #11, page 16.
Notes:
1. A cervical collar alone WILL NOT provide cervical spine
immobilization.
2. Do not use traction on the cervical spine!
3. Anticipate vomiting, seizures, and rapidly deteriorating
condition.
8
Trauma Protocol #5: Chest Injuries
Assessment
1. Perform Rapid Trauma Assessment. (See Trauma Protocol #2, page 4.)
2. Note unequal breath sounds, open wounds, flail segments, tracheal deviation, subcutaneous
emphysema, and adequacy of ventilation.
3. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
Treatment
1. Administer 100% oxygen via non-rebreather mask, or assist with bag-valve-mask at 24 times per
minute.
2. Seal open chest wound with occlusive dressing sealed on three sides to allow air to escape but
not to enter.
3. Stabilize rib fractures or flail segments with direct pressure, then bulky dressing secured to chest
wall.
4. Impaled object should be stabilized in place with an occlusive dressing.
5. Consider spinal immobilization if appropriate; or if possible, place patient on injured side.
Comparison of Pneumothorax, Hemothorax and Pericardial Tamponade
Signs/Symptoms
Tension
Pneumothorax
Hemothorax Pericardial
Tamponade
Presenting Symptoms Difficulty breathing and
then shock
Shock, then difficulty
breathing
Narrowing pulse
pressure, then shock
Neck Veins Distended Flat Distended
Breath Sounds Decreased or absent
on side of injury
Decreased or absent
on side of injury
Bilateral and clear
Percussion of Chest Hyperresonant Dull Normal Resonance
Tracheal Deviation Away from side of
injury
Usually not present Not present
Notes:
1. Suspect abdominal injuries if injury is below nipple line of chest.
2. Increasing respiratory distress should alert the EMT to a developing
tension pneumothorax.
3. Be sure to examine patients abdomen and posterior chest.
9
Trauma Protocol #6: Abdominal Injuries
Assessment
1. Perform Rapid Trauma Assessment. (See Trauma Protocol #2, page 4.)
2. Observe for wounds, bruises, evisceration, distention. Note any tenderness or rigidity.
3. Note mechanism of injury.
4. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
Treatment
1. Gently cover any eviscerated organ with gauze moistened with saline or water. DO NOT
attempt to push intestines back into the abdomen.
2. Immobilize impaled objects in place. DO NOT remove.
Notes:
1. If injury is high in abdomen, suspect chest injuries. (See
Trauma Protocol #5, page 9.)
2. Injury to the abdomen may cause vomiting; protect the airway.
3. Immobilize patient as indicated.
4. If the patient is female, determine if pregnant.
10
Trauma Protocol #7: Extremity Injuries
Assessment
1. Perform Rapid Trauma Assessment (Trauma Protocol #2, page 4) or Focused History and
Physical Exam.
2. Be alert for and treat for shock. (See Trauma Protocol #11, page16.)
3. Note mechanism of injury.
4. Check circulation, movement, and sensation distal to the injury before and after splinting.
Treatment
1. While extremity injuries are often conspicuous and painful injuries, they are rarely life-threatening
in and of themselves. Do not allow the obvious fracture to obscure other assessment findings.
2. Protect the injury from excessive movement.
3. Immobilize one joint above and below suspected injury. (See Reference #37, page 60.)
4. Realignment of fracture may be necessary to facilitate splinting, correct a circulatory compromise
or neurological deficit. However, careful assessment before and after manipulation and minimal
movement of injury site is critical.
5. Fractures involving joint (or within 3 inches of a joint) should be splinted in the position found.
6. Elevate and apply cold packs to injury when practical.
Notes:
1. Pelvic and femur fractures can cause sever hemorrhage; anticipate and
treat for shock!
2. Failure to immobilize fractures can do greater harm than the original
injury.
3. When using air splints, avoid overinflation which can result in circulatory
or neurological compromise. Observe for changes when moving from
cold to warm temperatures.
4. If other injuries are present, the long spine board will provide adequate
total body splinting.
11
Trauma Protocol #8: Amputations
Assessment
1. Perform Rapid Trauma Assessment. (See Trauma Protocol #2, page 4.) Be sure the obvious
injury is the only injury.
2. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
Treatment
1. Control bleeding with FIRM direct pressure.
2. Cover stump with sterile dressing.
3. Rinse amputated part gently and briefly with normal saline to remove loose debris; do not scrub.
4. Wrap amputated part in gauze moistened with saline.
5. Place wrapped part into plastic bag and seal with tape (do not pour more fluid into bag). Label
with name, date, and time.
6. Place plastic bag into container filled with ice and water. Cold packs can provide same level of
cooling. Do not allow it to freeze.
Notes:
1. Be sure amputated parts accompany ALL patients, including patients who
are
dead on arrival.
2. Many extremity parts can be re-attached: arm, ear, finger, foot, hand, leg,
nose, penis, and scalp.
3. Optimal results are obtained when implantation occurs within a few hours of
injury.
4. Arterial bleeding will require very firm direct pressure--dont just cover
bleeding with more dressings thereby hiding further bleeding
12
Trauma Protocol #9: Bleeding (External)
Assessment
1. Perform Rapid Trauma Assessment. (See Trauma Protocol #2, page 4.)
2. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
Treatment
1. Apply direct pressure over wound with your gloved hand.
2. Place sterile dressing over the wound and re-apply direct pressure. Secure with gauze or elastic
bandage.
3. Elevate the bleeding site.
4. Arterial bleeding will require firm prolonged pressure. DO NOT just cover active bleeding with
more dressings, thereby hiding further bleeding. If bleeding persists, control with
a. additional pressure dressings.
b. arterial pressure points.
c. tourniquet application as a last resort.
5. Apply splint to any associated fractures.
6. Check distal circulatory function.
Notes:
1. Consider removal of impaled objects only if necessary or if
the objects
a. Interferes with patient airway.
b. Bleeding absolutely cannot be controlled around it.
13
Trauma Protocol #10: Burns
Assessment
1. ENSURE YOUR OWN SAFETY.
2. Stop the burning process.
3. Perform Rapid Trauma Assessment. (See Trauma Protocol #2, page 4.)
4. Be alert and treat for airway and respiratory compromise. (See Medical Protocol #23, page 38.)
5. Be alert and treat for shock. (See Trauma Protocol #11, page 16.)
6. Identify mechanism of injury.
7. Estimate depth of burn, length of exposure, and percent of body surface area injured. (See
Reference #30, page 52.)
Treatment
Thermal Burns
1. Stop the burning process and remove burning clothing.
2. O
2
per non-rebreather mask at 10-15 LPM.
3. DO NOT cool burn with water. (Exception: presence of smoldering clothes, or material adhering
to skin that could continue burning process.)
4. Remove jewelry and clothing from burned area.
5. For large surface burns, place patient between clean sheets. For smaller burns, dress with
sterile dry dressings.
6. Be alert for hypothermia. (See Medical Protocol #21, page 34.)
7. Burns affecting less then 10% of the body may require moist sterile dressing.
Chemical Burns
1. Remove contaminant.
a. Chemical on skin.
1) Remove clothing and jewelry, flush skin with water for 10 minutes, and wash
gently with soap and water, then rinse.
2) If contaminant is dry powder, brush off BEFORE flushing.
3) Apply sterile dressing or burn sheet.
4) Identify contaminant.
5) See Poisonings, Medical Protocol #25, page 43.
b. Chemical in eye
1) Flood eye(s) with lukewarm water for at least 15 minutes; have patient blink
14
frequently during irrigation.
2) Identify contaminant.
3) See Poisonings, Medical Protocol #25, page 43.
Electrical Burns
1. Eliminate electrical contact--ENSURE YOUR OWN SAFETY.
2. O
2
per non-rebreather mask at 10-15 LPM.
3. Identify both entry and exit wounds. It is necessary to remove ALL clothing because exit wounds
may be on feet, etc.
4. Place patient between clean sheets.
5. Obtain vitals every 5 minutes.
6. Be prepared for cardiac arrest.
Notes:
1. Watch for hypothermia--heat loss is 70 times greater in a burn wound
area!
2. Be alert for progressing airway problems in patients with burns involving
face, head, neck or chest!
3. Be alert for smoke inhalation!
4. At the scene, the burn injury is the lowest priority. Remember the ABCs!
15
Trauma Protocol #11: Shock/Hypoperfusion
Assessment
1. Perform Rapid Trauma Assessment. (See Trauma Protocol #2, page 4.)
2. Early shock.
Restlessness and anxiety
Tachycardia, >110 BPM
Pale, cool, wet skin
Narrowed pulse pressure
Nausea and vomiting
Weakness
3. Late shock.
The above signs and symptoms plus:
Tachypnea
Diaphoresis
Decreased level of consciousness
Cyanosis
Hypotension <90 systolic
Treatment
1. Transport as soon and as efficiently as possible.
2. Immobilize the spine.
3. O
2
by non-rebreather mask at 10-15 LPM.
4. Control profuse external bleeding.
5. Elevate lower extremities.
6. Maintain body temperature.
7. Apply MAST/PASG if local protocols allow. (See Reference #33, page 55.)
8. Repeat Ongoing Assessment every 5 minutes. (See Trauma Protocol #1, page 1.)
Note:
1. Most field treatment of shock should be done in the ambulance on
the way to the hospital.
16
Trauma Protocol #12: Sexual Assault
Assessment
1. Protect the scene and preserve evidence in cooperation with law enforcement.
2. Crew members of the same sex may relate better with the patient in time of emotional crisis.
3. Do not allow patient to bathe, douche, brush teeth, defecate, urinate, or change clothes.
4. Notify law enforcement.
Treatment
1. Reassure patient and provide emotional support.
2. Administer O
2
if indicated.
3. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
4. Treat other injuries as indicated. See specific protocols.
5. Transfer to nearest center capable of handling sexual assault.
Notes:
1. This is a highly emotional and volatile situation; be sure your findings and
treatment are clearly documented on the trip report form.
2. Do not let emotions and anxiety cause you to miss underlying injuries and
to take priority over crime scene preservation.
17
Trauma Protocol #13: Near Drowning
Assessment
1. Perform Rapid Trauma Assessment (Trauma Protocol #2, page 4) using spinal precautions.
2. If patient is hypothermic, respiratory and pulse rates may be slower and more difficult to feel.
check for a minimum of 30 to 45 seconds.
3. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
4. Note and record
a) Cleanliness of the water,
b) Length of submersion,
c) Age and general health of the victim, and
d) Water temperature (be alert for hypothermia).
Treatment
1. Protect yourself.
2. If trained to do so, rescue the victim from the water (ventilation can take place in the water).
3. If patient was diving or fell, observe cervical spine precautions.
4. Perform CPR, if needed, as you would for any patient in cardiac arrest.
5. If patient has spontaneous respirations, administer O
2
by non-rebreather mask at 10-15 LPM;
ventilate and suction as needed.
6. Control any profuse bleeding.
7. Transport ALL near drowning victims to the hospital.
Notes:
1. Gastric distension and vomiting are common in near drowning. Be
prepared!
2. Victims in cold water (below 68
o
F can sometimes be resuscitated after
30 minutes or more in cardiac arrest.
3. A near drowning victim can develop secondary complications (such as
pulmonary edema) and die up to 72 hours after the incident. (Fifteen
15% of deaths are due to secondary complications.)
18
Medical Protocol #14: Medical Assessment
1. Complete Scene Size-Up and Initial Assessment. (See Trauma Protocol #1, page 1.)
2. Assess the history of present illness, using OPQRST questions. (See Reference #35, page 58.)
3. Responsive patient.
a. Assess chief complaint and signs/symptoms.
b. Obtain SAMPLE history. (See Reference #35, page 58.)
c. Obtain baseline vital signs.
d. Perform physical assessment as needed.
4. Unresponsive patient.
a. Rule out trauma.
1) If unable to rule out trauma, immobilize cervical spine and do Trauma
Assessment. (See Trauma Protocol #2, page 4.)
b. Rapidly assess head, neck, chest, abdomen, pelvis, extremities, and posterior of patient.
c. Obtain SAMPLE history.
d. Obtain baseline vital signs.
5. Perform care based on signs and symptoms.
19
Medical Protocol #15: Abdominal Pain
Assessment
1. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
2. Visualize and palpate abdomen.
3. Obtain pertinent medical history.
a) SAMPLE. (See Reference #35, page 58.)
b) OPQRST. (See Reference #35, page 58.)
c) Bowel and urinary function? Bleeding?
d) Last menstrual period? Possibly pregnant?
e) Vomiting or nausea?
4. Obtain and record vital signs.
Treatment
1. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
2. Allow patient to seek position of comfort.
3. Consider oxygen administration.
20
Medical Protocol #16: Anaphylaxis
Assessment
1. Perform Patient Assessment. (See Medcail Protocol #14, page 19.)
2. Presence of edema of tongue, mouth and/or throat, dyspnea, and/or hypoperfusion are
indications for immediate transport.
3. Be alert for and treat for dyspnea. (See Medical Protocol #23, page 38.)
4. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
5. Obtain pertinent medical history.
a) SAMPLE.
b) Possible source of toxin/reaction.
6. Note the medications the patient has taken, how much, when, and response.
Treatment
1. O
2
per non-rebreather mask at 10-15 LPM.
2. Consider administration of epinephrine auto-injector. (See Medical Protocol #16b, page 22.)
3. If an insect sting, scrape stinger out. Do not pull stinger out. Consider constricting band if on an
extremity.
4. No treatment should significantly delay transport of critical patients.
Notes:
1. Airway management is the top priority.
2. The EMT MAY ASSIST THE PATIENT in administration of prescribed
epinephrine auto-injectors.
3. Check for medical alert tags.
4. Runny nose, watery eyes, itching skin, skin rash are all forms of allergic
reactions. These may progress to more severe reactions like asthma or
anaphylaxis.
21
Medical Protocol #16b: Epinephrine Auto-Injector
Medication Names
1. Generic: epinephrine.
2. Trade: Adrenalin, Epi-Pen.
Indications
1. Patient exhibits signs of a severe allergic reaction, including either respiratory distress or shock.
2. Medication is prescribed for this patient by a physician.
3. Medical direction authorizes use for this patient.
Contraindications
1. No contraindications when used in a life-threatening situation.
Dosage
1. Adult: one auto-injector (0.3mg).
2. Child or infant: one infant/child auto-injector (0.15mg).
Administration
1. Obtain patient's auto-injector.
a. Ensure that prescription is written for the patient who is experiencing the reaction.
b. Ensure that the medication is not discolored (if visible).
2. Obtain medical direction, either on-line or off-line.
3. Remove cap from auto-injector.
4. Place tip of auto-injector on the lateral portion of the patient's thigh, midway between waist and
knee.
5. Push the injector firmly against the thigh until the injector activates.
6. Hold the injector in place until the medication is injected (at least 10 seconds).
7. Document administration site, dose, and time.
8. Dispose of injector in biohazard (sharps) container.
9. If patient's condition worsens (decreasing mental status and blood pressure and increasing
respiratory distress), obtain authorization for an additional dose. Treat for shock and be prepared
to initiate basic life support procedures.
10. If patient's condition improves, continue oxygen therapy and treat for shock.
22
Side Effects
1. Increased heart rate.
2. Pallor.
3. Dizziness.
4. Chest pain.
5. Headache.
6. Nausea and vomiting.
7. Excitability, anxiety.
Actions:
1. Dilates the bronchioles.
2. Constricts the blood vessels.
23
The EMT must be certified as a Healthcare Provider or BLS-C and renew that certification each year.
The EMT should perform CPR in accordance with the latest American Heart Association standards.
Medical Protocol #17: Cardiopulmonary Resuscitation (CPR)
Objectives Actions
Adult: 8 years and older
Child: 1 to 8 years
Infant: less than one year
1. Assessment:
Determine un-
responsiveness.
Adult/Child: Tap or gently shake shoulder. Shout
"Are you OK?"
Infant: Observe.
2. Activate EMS system
if patient is an adult.
Call 911 or your local emergency number.
2a. Get help if patient is
a child or infant.
Call out "Help!"
3. Position the victim. Turn on back as a unit, supporting head and neck
if necessary.
A. Airway
4. Open the airway. Head tilt-chin lift or jaw thrust.
5. Assessment:
Determine
breathlessness.
Maintain open airway. Place ear over mouth,
observing chest. Look, listen, and feel for
breathing.
B. Breathing
6. If victim is not
breathing, give two slow
breaths.
Maintain open airway. Seal mouth to barrier
device and give two slow breaths, 1 1/2 to 2
seconds each. Observe chest rise. Allow lung
deflation between breaths.
7. If airway is obstructed a. Reposition victim's head, open airway and re-
attempt rescue breaths.
b. If rescue breaths unsuccessful, activate EMS.
c. Adult/Child: Give five sub-diaphragmatic
abdominal thrusts--the Heimlich maneuver.
Infant: Alternate five back blows with five chest
thrusts.
d. Adult: Check for foreign body with a finger
sweep.
Child/Infant: Finger sweep only if you see a
foreign body in the airway.
If unsuccessful, repeat steps a, c, and d.
24
Objectives Actions
8. Assessment:
Determine
pulselessness.
Adult/Child: Check carotid pulse.
Infant: Check brachial pulse.
8a. If child or infant,
activate EMS.
If someone responded to call for help, send them
to activate the EMS system. If rescuer is alone,
do one minute of CPR and then activate EMS
system.
9. Begin chest
compressions by
checking landmark.
Adult/Child: Run middle finger along bottom edge
of rib cage to notch at center (tip of sternum).
Infant: Draw an imaginary line with index finger
between the nipples.
10. Hand position. Adult/Child: Place index finger next to finger on
notch. Place hand next to index finger, and then
compress 1 1/2 to 2 inches with both hands for
adults, 1 to 1 1/2 inches with one hand for
children.
Infant: Place 2 to 3 fingers on sternum, one
finger's-width below imaginary line, and depress
1/2 to 1 inch.
C. Circulation
11. Compression rate Adult: 80 to 100 per minute.
Child: 100 per minute.
Infant: at least 100 per minute.
12. Ration of chest
compressions to
ventilations
Adult: 15 chest compressions to 2 ventilations.
Child/Infant: 5 chest compressions to 1
ventilation.
CPR Cycles
13. Number of cycles Adult: four cycles (about one minute)
Child/Infant: 20 cycles (about one minute)
14. Reassessment Adult/Child: Palpate for carotid pulse. If no pulse,
resume CPR starting with chest compressions.
Infant: Palpate for brachial pulse. If no pulse,
resume CPR starting with chest compressions.
Option for Return of
Pulse
15. If no breathing, give
rescue breaths.
Adult: One breath every five seconds.
Child/Infant: One breath every three seconds.
25
Second rescuer: "I know
CPR. Can I help?"
First rescuer completes
CPR cycle.
Adult: End cycle with two rescue breaths.
Child/Infant: End cycle with one rescue breath.
Option for Entrance
of Second Rescuer
Second rescuer checks
pulse.
Adult/Child: Palpate carotid pulse.
Infant: Palpate brachial pulse.
If no pulse, continue
CPR.
Second rescuer begins chest compressions. First
rescuer delivers rescue breaths. Continue cycles
of five compressions to one rescue breath for
adult, child, and infant.
Monitor. Second rescuer should monitor adequacy of
rescue breaths by observing chest rise and the
first rescuer should monitor chest compressions
by palpating carotid pulse.
26
Medical Protocol #18: Cerebrovascular Accident - Stroke
Assessment
1. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
2. Symptoms depend on area of brain affected. Monitor motor, speech, and sensory centers.
3. Obtain pertinent medical history.
a) SAMPLE. (See Reference #35, page 58.)
b) Glasgow coma scale. (See Reference #32, page 54.)
c) Pupil reaction.
d) Vital signs.
e) Neurological assessment on all four extremities.
f) Observe face for asymmetry.
Treatment
1. Protect airway, suction secretions if needed.
2. O
2
by non-rebreather mask at 10-15 LPM.
3. Elevate head of bed, allow patient to seek position of comfort, and maintain body heat.
4. Protect paralyzed extremities.
5. Reassure patient continuously and transport quietly to hospital.
Notes:
1. While stroke patients may not be able to speak they are usually aware
of their surroundings and are anxious. Talk to your patient and keep the
patient informed about the treatment being rendered even if the patient
is unconscious. High speed and loud sirens during transport may
increase the anxiety and are rarely necessary.
2. Transient Ischemic Attacks (TIAs) are temporary stroke symptoms
lasting from several minutes to hour and may warn of an impending
CVA.
3. Watch for signs of seizure activity. (See Medical Protocol #27, page 48.)
27
Medical Protocol #19: Chest Pain
Assessment
1. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
2. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
3. Be alert for irregular pulse rhythm.
4. Obtain and record vital signs every 5 minutes.
5. Obtain pertinent medical history.
a) SAMPLE. (See Reference #35, page 58.)
b) OPQRST. (See Reference #35, page 58.)
Treatment
1. O
2
by non-rebreather mask at 10-15 LPM.
2. Do not allow patient to ambulate. Place patient in position of comfort and loosen clothing.
Unconscious patients should be placed in the recovery position.
3. The EMT may assist the patient with self-administration of their own nitroglycerine (1 tablet),
repeated at 5 minute intervals if systolic BP remains above 100 mmHg, to a maximum of 3 tablets
or relief of pain. (See Medical Protocol #19b, page 29.)
4. Expedite transport and notify hospital as soon as possible.
Notes:
1. Be prepared to deal with respiratory and cardiac arrest.
2. Remember, with the new thrombolytic agents, time equals heart muscle.
USE THE PATIENTS TIME WISELY!
28
Medical Protocol #19b: Nitroglycerin
Medication Names
1. Generic: Nitroglycerin.
2. Trade: Nitrostat, Nitro-bid.
Indications
1. The patient complains of chest pain.
2. The patient has a history of cardiac problems.
3. The patient's physician has prescribed nitroglycerin.
4. The systolic blood pressure is greater than 100 systolic.
5. Medical direction authorizes administration of the medication.
Contraindications
1. The patient has hypotension or a systolic blood pressure below 100.
2. The patient has a head injury.
3. The patient is an infant or child.
4. The patient has already taken the maximum prescribed dose.
Dosage
1. One tablet (0.4 mg) or one spray, sublingual. If no relief and systolic blood pressure remains
above 100, and if authorized by medical direction, two additional doses may be given 3 to 5
minutes apart.
Administration
1. Perform focused assessment for cardiac patient.
2. Take blood pressure.
3. Contact medical direction if no standing orders.
4. Assure right medication, right patient, right dose, and check expiration date.
5. Assure patient is alert.
6. Question patient on last dose taken and effects. Assure understanding of route of administration.
7. Ask patient to lift tongue and place tablet or spray dose under tongue (while wearing gloves) or
have patient place tablet or spray under tongue.
8. Have patient keep mouth closed with tablet under tongue (without chewing and swallowing) until
dissolved and absorbed.
29
9. Recheck blood pressure in two minutes.
10. Document administration, route, and time.
11. Monitor blood pressure and pulse rate.
12. Ask patient about pain relief.
Side Effects
1. Hypotension.
2. Headache.
3. Pulse rate changes.
Actions:
1. Relaxes blood vessels.
2. Decreases workload of heart.
30
Medical Protocol #20: Childbirth
Assessment
1. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
2. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
3. Obtain pertinent medical and obstetrical history.
a) Chronic illness; i.e., seizures, cardiac problems, diabetes, etc.
b) Number of pregnancies (gravidity).
c) Number of live births (parity).
d) Onset, frequency and duration of contractions.
e) Length of labor in previous births.
f) Membranes ruptured.
g) Date of expected birth.
h) Expecting multiple births.
4. Visualize patient's perineum.
a) If perineum is bulging or crowning is visualized prepare to deliver the baby.
b) If patient has had one or more normal deliveries and complains of urge to "push,"
"bear down," or "have a bowel movement" prepare to deliver the baby.
c) If no visible signs of impending delivery transport patient to the hospital.
d) If complications are apparent; i.e., foot, hand, or cord visible or severe bleeding.
TRANSPORT immediately to hospital.
Normal Delivery
1. Allow delivery to progress spontaneously; unwrap OB kit and prepare mother for delivery.
Administer O
2
by non-rebreather mask at 10-15 LPM.
a) Use gentle counter-pressure equally distributed on top of baby's head to prevent
explosive birth.
b) Suction baby's airway, both nose and mouth, with bulb syringe as soon as head is
clear of birth canal.
c) Support baby's head and body as delivery proceeds. DO NOT PULL ON BABY. Gentle
downward pressure on upper shoulder may be needed if shoulders don't deliver quickly.
d) Reassure the mother continuously, keeping her informed of progress and instructing
her to push with contractions.
31
2. When baby is delivered.
a) Using bulb syringe, again suction MOUTH first, then the NOSE.
b) Keep the baby at the level of the vagina to prevent over/under transfusion.
c) Stimulate cry by tapping soles of feet. If no spontaneous cry within 1 minute, suction
again and begin CPR. (See Medical Protocol #17, 24.)
d) Check respiratory rate.
1) >20 or crying: no action needed.
2) <20: tactile stimulation, assist ventilations as needed with 100% O
2
.
Check heart rate.
1) >100: no action needed.
2) 60-100: ventilate with 100% O
2
.
3) <60: begin chest compressions and ventilate with 100% O
2
.
Check color.
1) Normal: no action needed.
2) Central cyanosis: 100% O
2
and assist ventilation as needed.
e) Double clamp the cord at least 4 inches from baby and cut between the clamps.
f) Dry the infant thoroughly, wrap in dry blanket and place on mother's abdomen.
g) Record APGAR (See Reference #29, page 51.) at 1 minute and 5 minutes after birth.
h) Do not wait for delivery of placenta; however, if placenta delivers spontaneously
1) Place placenta in plastic bag and transport along into the hospital.
2) Gently massage mother's lower abdomen until it becomes firm.
3) Place sterile pad over vaginal opening.
4) Cover mother with clean bedding.
Abnormal Delivery
1. Breech (buttocks first).
a) Administer O
2
by non-rebreather mask at 10-15 LPM.
b) Allow delivery to progress spontaneously.
c) Support infant's body as it is delivered.
d) If head delivers spontaneously, proceed as in normal delivery.
e) If head does not deliver within 3 minutes, insert gloved hand into vagina, keeping your
palm TOWARD baby's face; form a "V" with your fingers and push wall of vagina AWAY
from baby's face, thereby creating an airway for baby.
f) TRANSPORT IMMEDIATELY. DO NOT REMOVE YOUR HAND UNTIL RELIEVED BY
HOSPITAL STAFF.
32
2. Limb presentation.
a) Place mother in Trendelenburg position.
b) Administer O
2
by non-rebreather mask at 10-15 LPM.
c) TRANSPORT IMMEDIATELY.
3. Prolapsed cord.
a) Place the mother in Trendelenburg position.
b) Administer O
2
by non-rebreather mask at 10-15 LPM.
c) Insert gloved hand into vagina and gently push baby's head off the cord.
d) TRANSPORT IMMEDIATELY. DO NOT REMOVE HAND UNTIL RELIEVED BY
HOSPITAL STAFF.
4. Multiple births.
a) This is usually not a surprise to the mother, as she has probably already been told to
expect the same by her doctor, but BE ALERT for the multiple birth possibility. Monitor
patient closely.
b) Deliver as you would for normal delivery of one infant.
5. Heavy vaginal bleeding following delivery.
a) Control bleeding; massage lower abdomen firmly.
b) Treat for shock. (See Trauma Protocol #11, page 16.)
c) Consider putting baby to breast.
d) Transport immediately.
6. Miscarriage.
a) May result in profuse vaginal bleeding.
b) Treat for shock. (See Trauma Protocol #11, page 16.)
c) Save expelled tissues and transport without delay to the hospital.
Notes:
1. If cord is around babys neck during delivery, slip cord over
babys
head to avoid strangulation.
2. The greatest risk to the newborn is airway obstruction and
hypothermia. KEEP BABY COVERED, WARM AND DRY.
KEEP AIRWAY SUCTIONED with bulb syringe.
3. When using bulb syringe to suction infant, remember to squeeze
bulb PRIOR to insertion into babys mouth or nose.
4. Greatest risk to mother is postpartum hemorrhage; watch closely
for signs of shock and excessive vaginal bleeding.
33
Medical Protocol #21: Cold Emergencies
Assessment
1. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
2. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
3. Because breathing and pulse rates may be slower and more difficult to feel, assess for a
minimum of 30 to 45 seconds.
Treatment
Frostbite
1. Protect injured areas from pressure, trauma, and friction.
2. Remove all coverings from injured areas, but DO NOT RUB OR BREAK BLISTERS. Cover with
dry sterile dressings.
3. Do not allow patient to ambulate unless absolutely necessary.
4. Do not allow limb to thaw if there is a chance that the limb might refreeze before evacuation is
completed.
5. Maintain core temperature with blankets.
6. Rewarming frostbitten area should be left for a hospital setting.
Hypothermia
1. HANDLE WITH CARE! Rough handling might precipitate cardiac arrest. If cardiac arrest
develops, treat as normothermic patient. (See Medical Protocol #17, page 24.)
2. Administer warm O
2
by non-rebreather mask at 10-15 LPM.
3. Gently remove cold/wet clothing and replace with blankets.
4. When practical, major rewarming should be left for a hospital setting.
5. Cover patient with warm blankets during transport.
34
Notes:
1. If possible, core temperature should be recorded with a low-temperature
rectal thermometer. Shivering occurs between 86-90
o
F, but not below. This
is an indication of severity of hypothermia in the patient.
2. Chest compressions should never be done if clinical signs of functional
cardiac activity are present, even if a pulse is not palpable under field
conditions; i.e., movement, respirations, or other signs of life.
35
Medical Protocol #22: Diabetic Emergencies
Assessment
1. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
2. Obtain pertinent medical history from patient, family, bystanders and check for medical
identification device.
a) How much and when was insulin taken.
b) Patients last meal.
c) Recent or current illness, heavy exercise or high stress; i.e., flu, athletic activity, accident.
3. If unconscious, check Glasgow coma scale. (See Reference #32, page 54.)
4. See Reference #31, page 53 for diabetes fact sheet.
Treatment
1. Protect airway and administer O
2
per non-rebreather mask at 10-15 LPM.
2. Maintain body temperature. In South Dakota, hypoglycemia is the most common cause of
hypothermia.
3. If patient is conscious, administer a substance high in sugar; i.e., honey, commercial glucose
preparation (See Medical Protocol #22b, page 37), or orange juice with 2-3 teaspoons sugar
added.
4. Transport in position of comfort. If unconscious, transport patient on side in recovery position.
Notes:
1. Under no circumstances allow the administration of insulin!
2. Be prepared for patient to vomit!
3. Unconsciousness may occur in diabetic patients from other etiologies as
well. (See Medical Protocol #28, page 50.)
36
Medical Protocol #22b: Oral Glucose
Medication Names
1. Generic: oral glucose.
2. Trade: Glucose, Insta-Glucose.
Indications
1. Patients with an altered mental status and a known history of diabetes mellitus.
Contraindications
1. Unconsciousness.
2. Unable to swallow.
3. Known diabetic who has not taken insulin for a number of days.
Dosage
1. One tube or as directed on the package and by medical direction.
Administration
1. Assure the patient has signs and symptoms of altered mental status and a known history of
diabetes.
2. Assure the patient is conscious, can swallow, and maintain airway.
3. Administer glucose.
a. Place gel on a tongue depressor between cheek and gum.
b. Have the patient self-administer between cheek and gum.
4. If the patient loses consciousness or has a seizure, remove tongue depressor from mouth.
Side Effects
1. None when given properly. May be aspirated by a patient without a gag reflex.
Action:
1. Increases blood sugar.
37
Medical Protocol #23: Dyspnea (Difficulty Breathing)
Assessment
1. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
2. Note signs of respiratory insufficiency.
a) Respiratory rate <10 or >30 breaths per minute.
b) Cyanosis.
c) Decreased level of consciousness. (See Glasgow coma scale, Reference #32, page 54.)
d) Increased anxiety and restlessness.
e) Abnormal respiratory pattern; i.e., Cheyne-Stokes respirations.
f) Use of accessory muscles in breathing.
g) Neck vein distension.
h) Cough producing frothy, purulent, or blood-tinged sputum.
I) Ankle edema.
3. Assess breath sounds, note type and location; i.e., bilateral sounds, wheezing, rales, and stridor.
4. Obtain pertinent medical history and check for medical identification device.
a) Onset and duration of problem.
b) Previous similar episode.
c) Current medications (prescription, non-prescription) and when last taken.
d) Known allergies.
e) Associated symptoms; i.e., chest pain.
Treatment
1. Administer O
2
per non-rebreather mask at 10-15 LPM.
2. Assist ventilations if needed with 100% O
2
.
3. Loosen restrictive clothing, sit upright or allow patient to seek position of comfort.
4. REASSURE THE PATIENT.
5. Consider administration of metered-dose inhaler. (See Medical Protocol #23b, page 40.)
38
Notes:
1. DO NOT withhold O
2
if it is needed! If COPD patients react adversely be
prepared to assist ventilations.
2. Conscious, dyspneic patients may rapidly deteriorate to respiratory failure and
arrest. PREPARE TO INTERVENE!
3. DYSPNEA is a symptom, not a disease/injury. Reassess for cause and
correct as necessary/possible.
4. Allergic reactions are frequently responsible for dyspneic episodes, thus
assessment for known allergies must include substances other than
medications.
5. If patient has a personal prescribed inhaler, the EMT may assist the patient
with administration.
6. When dealing with pediatric patients, consider allowing parent to accompany
patient.
7. DO NOT significantly delay transport with BLS treatments.
39
Medical Protocol #23b: Prescribed Inhaler
Medication Names
1. Generic: albuterol, isoetharine, metaproteranol.
2. Trade: Proventil, Ventolin, Bronkosol, Bronkometer, Alupent, Metaprel.
Indications
Meets all of the following criteria.
1. Patient exhibits signs and symptoms of respiratory emergency.
2. Patient has a physician prescribed handheld inhaler.
3. Specific authorization by medical direction to use.
Contraindications
1. Inability of patient to use the device; i.e., not alert.
2. Inhaler is not prescribed for patient.
3. No authorization from medical direction.
4. Patient has already taken maximum prescribed dose prior to the EMT's arrival.
Dosage
1. Number of inhalations based on medical direction.
Administration
1. Obtain authorization from medical direction, either on-line or off-line.
2. Check the expiration date of the inhaler.
3. Check if the patient has already used the inhaler.
4. Assure the inhaler is at room temperature or warmer.
5. Shake inhaler vigorously several times.
6. Remove oxygen adjunct from patient and have the patient exhale deeply.
7. Have the patient put his/her lips around the opening of the inhaler.
8. Instruct the patient to begin an inhalation and then depress the inhaler.
9. Instruct the patient to hold his/her breath for as long as comfortably possible to enhance
absorption of the medication.
10. Replace the oxygen adjunct on the patient.
40
11. Allow patient to breathe normally for 1-2 minutes and then repeat second dose if so ordered.
12. If the patient has a spacer device, it should be used to allow more effective use of the medication.
13. Document use of the inhaler.
14. Reassess vital signs, the chest, and respiratory status.
15. If breathing becomes inadequate, provide artificial ventilations.
Side Effects
1. Increased heart rate.
2. Tremors.
3. Nervousness.
Action:
1. The prescribed inhalers are beta-agonist bronchodilators. They dilate the
bronchioles, reducing airway resistance.
41
Medical Protocol #24: Heat Emergencies
Assessment
1. Perform Patient Assessment. (See Protocol #14, page 19.)
2. Record skin temperature, condition, and color.
3. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
4. Obtain pertinent history.
Treatment
1. Remove from heat source.
2. Administer O
2
per non-rebreather mask at 10-15 LPM.
3. Transport and cool enroute by sponge bathing with water.
Notes:
1. Rapid cooling may cause vomiting!
2. Not all heat emergencies are environmental in nature. They may have
febrile, neurological, or pharmacological etiology.
3. High body temperature is associated with seizures, particularly in
infants. (See Medical Protocol #27, page 48.)
4. Heat stroke frequently presents altered level of consciousness or
neurological symptoms.
42
Medical Protocol #25: Poisonings
Assessment
1. PROTECT YOURSELF FROM POSSIBLE EXPOSURE.
2. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
3. Be alert for and treat respiratory difficulty. (See Medical Protocol #23, page 38.)
4. Be alert for and treat shock. (See Trauma Protocol #11, page 16.)
5. Be alert for and treat seizures. (See Medical Protocol #27, page 48.)
6. Identify time of exposure, contaminant, and quantity. If possible, take empty containers to
hospital.
7. Obtain pertinent history.
Treatment
Ingested Poison
1. Identify substance and quantity ingested.
2 Place patient in recovery position. Vomiting is common.
3. Contact Poison Control Center and treat as directed.
4. Consider administration of activated charcoal. (See Medical Protocol #25b, page 45.)
Inhaled Poison
1. Remove patient to fresh air. Place in recovery position.
2. Administer O
2
by non-rebreather mask at 10-15 LPM.
3. Assist ventilations as needed with 100% O
2
via bag-valve-mask.
4. Identify substance inhaled and duration of exposure.
5. Contact Poison Control Center and treat as directed.
Poison on Skin
1. Remove contaminated clothing and flood skin with water for 10 minutes; wash with soap and
water, then rinse.
2. If contaminant is dry powder, brush off before washing.
3. Identify contaminant.
43
4. Contact Poison Control Center and treat as directed.
Poison in Eye
1. Flood eye(s) with lukewarm water continuously for at least 15 minutes. Have patient blink
frequently during irrigation.
2. Identify contaminant.
3. Contact Poison Control Center and treat as directed.
Injected Poison (Stings, Poisonous Snakebites, Etc.)
1. BE ALERT for dyspnea. (See Medical Protocol #23, page 38.)
2. Check for medical identification device and ask about history of allergies.
3. Try to identify source of injected poison, and check for marks, rashes, or welts.
4. Transport immediately.
5. Consider constricting band and/or sterile suction.
Notes:
1. If ingestion is by small child, other children present may also have
ingested substance.
2. Use gloves and waterproof gowns during decontamination of pesticides
and other toxins that can be absorbed through the skin on contact.
3. Delays in transport will increase the amount of toxin absorbed.
SIOUX VALLEY POISON CONTROL CENTER
STATE OF SOUTH DAKOTA TOLL FREE NUMBER
1-800-764-7661
(1-800-POISON-1)
44
Medical Protocol #25b: Activated Charcoal
Medication Names
1. Generic: activated charcoal.
2. Trade: Superchar, Instachar, Actidose, Liqui-char.
Indications
1. Poisoning by oral ingestion.
Contraindications
1. Altered mental status.
2. Ingestion of acids or alkalis.
3. Inability to swallow.
Dosage
1. Adults and children: 1 gram activated charcoal per kilogram of body weight.
2. Usual adult dose: 25-50 grams.
3. Usual pediatric dose: 12.5-25 grams.
Administration
1. Consult medical direction.
2. Shake container thoroughly.
3. Patient may need to be persuaded to drink the medication as it has an unpleasant appearance.
Providing a covered container and straw may improve patient compliance.
4. If patient does not drink the medication right away, the charcoal will settle. Shake or stir it again
before continuing administration.
5. Document the name of the medication, the dose, and the route and time of administration.
6. Be prepared for the patient to vomit.
Side Effects
1. Black stools.
2. Some patients, particularly those who have ingested poisons that cause nausea, may vomit. If
the patient vomits, repeat the dose once.
45
Action:
1. Activated charcoal binds to certain poisons and prevents them from being
absorbed into the body.
46
Medical Protocol #26: Phychiatric Emergencies
Assessment
1. PROTECT YOURSELF AND OTHERS. Summon law enforcement if necessary.
2. ONE EMT should be responsible for situation and establish contact with the patient to reduce
confusion and minimize stress. Multiple EMTs might increase patient's confusion and agitation.
3. Assess and treat life threatening injuries. Additional assessment and treatment as situation
permits.
4. Obtain pertinent medical history.
a) Prescription or non-prescription drugs.
b) Possible underlying medical cause; i.e., hypoxia, brain tumor, chemotherapy,
hypoglycemia, etc.
c) Previous history of psychiatric problems.
d) Events immediately preceding problem/incident.
Treatment
1. The SAME EMT who performed assessment should remain with patient during transport.
2. Speak in a calm, quiet voice. Move slowly and explain what you are doing. Be honest, direct and
non-threatening.
3. Keep environment as quiet as possible; do not use lights and sirens unless indicated by injuries.
Notes:
1. Use physical restraint only if necessary for the protection of
yourself or the patient.
2. If patient refuses treatment, contact law enforcement.
47
Assessment
Medical Protocol #27: Seizures
1. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
2. Obtain pertinent medical history.
a) Medical alert tag, known seizure disorder.
b) Medications, what and when last taken.
c) Alcohol or drug intake.
d) Recent trauma. (See Head/Neck/Spine Injuries, Trauma Protocol #4, page 7.)
e) Note fever, particularly in children under five years of age. (See Heat Emergencies,
Medical Protocol #24, page 42.)
f) Note number and duration of seizures.
Treatment
During Seizure
1. DO NOT attempt to put anything into patient's mouth.
2. Protect patient from injury during seizure. Remove hazards. Avoid physical restraint unless
absolutely necessary.
3. Maintain patient's dignity by removing bystanders from scene and covering patient if possible.
4. Nasopharyngeal airways may be useful during seizures. Use with caution, however, as
nosebleeds are common if placed during seizure.
After Seizure
1. Administer O
2
by non-rebreather mask at 10-15 LPM.
2. Treat injuries per specific protocols.
3. Reassure patient by telling them what happened, where they are, and who you are.
4. Place patient in recovery position and have suction ready.
5. Transport in a quiet, non-stimulating environment. Lights and sirens may precipitate additional
seizure activity and should be used only if necessitated by injuries.
48
Notes:
1. Treatment of seizures is focused on maintaining the patients
airway and preventing injury. However, DO NOT attempt to insert
tongue blade or other instruments in the mouth of a patient having
a seizure.
2. Assessment and treatment should take place after the seizure has
terminated. Seizures lasting more than five minutes OR two or
more seizures without a period of consciousness between them
are
a LIFE-THREATENING emergency and transportation may be
necessary during seizure activity.
49
Medical Protocol #28: Unconscious Patient
Assessment
1. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
2. If unconsciousness is due to TRAUMA or UNKNOWN ETIOLOGY, assume patient has a spinal
injury and perform RAPID TRAUMA ASSESSMENT. (See Trauma Protocol #2, page 4.)
3. Assess for trauma, drugs, diabetes, breath odor, needle tracks, and medical alert tags.
4. Be alert for and treat for shock. (See Trauma Protocol #11, page 16.)
5. Perform Glasgow coma scale (See Reference #32, page 54.) and assess pupils for reactivity,
size, and equality.
Treatment
1. Immobilize spine if indicated; otherwise place patient in recovery position.
2. Administer O
2
by non-rebreather mask at 10-15 LPM, suction, and assist ventilations as needed.
3. Find and transport all medications with patient.
4. Treat as indicated; see specific protocols.
5. Activate advanced life support unit if available.
Notes:
1. TALK to patient. Hearing is the last sense to be lost, even in coma.
2. Prepare for seizure. (See Medical Protocol #27, page 48.)
3. Prepare for a combative, disoriented patient.
4. Prepare for respiratory/cardiac arrest. (See Medical Protocol #17,
page 24.)
50
Reference #29: APGAR Scores
Assessment O Points 1 Point 2 Points
Blue, pale Body: pink
Extremities: blue
Fully pink Appearance (Skin Color)
Absent Less than 100 More than 100 Pulse Rate
No response Some motion Active motion Grimace (Reflex Irritability
When Feet Stimulated)
Flaccid Some flexion Active motion Activity (Muscle Tone)
Absent Weak cry Strong cry Respiratory Effort
- APGAR scores should be taken one and five minutes after birth.
- Infants with a score of 7-10 usually require supportive care only.
- Scores of 4-6 indicate moderate depression.
- Infants with scores less than 4 require aggressive resuscitation.
51
Reference #30: Burn Chart
Adult Child
(Only 2 and 3 burns are counted)
Note:
1. Major burns should be treated in a burn center. These include
burns covering more than 25% of body surface area; burns of
hands, feet, face or perineum; electrical burns; inhalation
injuries; severe chemical burns; other co existing injuries; or
severe pre-existing medical problems.
52
Reference #31: Diabetes Fact Sheet
Signs and Symptoms Diabetic Coma
(Ketoacidosis)
Insulin Shock
(Low Blood Sugar)
Appearance Extremely ill Very weak
Skin Red and dry Pale and wet
Mouth Dry Drooling
Thirst Intense Absent
Hunger Absent Intense
Respiratory Exaggerated air hunger
(Kussmaul's respirations)
Normal - shallow
Breath Odor Acetone (sweet) Normal
Blood Pressure Low Normal
Rapid Normal or rapid Pulse
Restless, decreasing level of
consciousness
Apathy, irritability, decreasing
level of consciousness
Mental State
Tremors Absent Frequent
Gradual, over hours or days Onset Acute, over minutes
Rate of Improvement Gradual: 6-12 hours following
administration of insulin
Immediate: within minutes of
administering glucose
53
Infant Child/Adult
Eye Opening
4 Spontaneously
3 To speech
Reference #32: Glasgow Coma Scale
2 To pain
______ 1 No response
Spontaneously 4
To command 3
To pain 2
No response 1_______
Best Verbal Response
5 Coos, babbles
4 Irritable cries
3 Cries to pain
2 Moans, grunts
______ 1 No response
Oriented 5
Confused 4
Inappropriate words 3
Incomprehensible 2
No response 1_______
Best Motor Response
6 Spontaneous Obeys commands 6
5 Localizes pain Localizes pain 5
4 Withdraws from pain Withdraws from pain 4
3 Flexion (decorticate) Flexion (decorticate) 3
2 Extension (decerebrate) Extension (decerebrate) 2
______ 1 No response No response 1_______
______ Total Total _______
Revised Trauma Score
Respiratory Rate 10 - 29 4
> 30 3
6 - 9 2
1 - 5 1
None 0 _______
Systolic Blood Pressure > 90 4
76 - 89 3
50 - 75 2
1 - 49 1
No pulse 0 _______
Convert Glasgow Coma Scale 13 - 15 4
9 - 12 3
6 - 8 2
4 - 5 1
1 - 3 0 _______
Total for Revised Trauma Score _______
54
Indications for Application
Any history of illness or injury, signs/symptoms which make the EMS person suspect shock.
Indications for Inflation
1. BP <80 with pulse >100 BPM and a chief complaint or mechanism of injury consistent with
shock.
2. Injury to lower extremity or pelvis.
Contraindications
1. Pulmonary edema.
2. Cardiogenic shock.
3. Trauma above the level of the MAST/PASG.
Modifications
Contact medical control for permission to
1. Inflate abdominal section for patient who is obviously pregnant.
2. Remove impaled objects before any attempt to apply MAST.
3. Use MAST for any non-trauma source of shock.
4. Inflate MAST with potentially uncontrolled hemorrhage outside the confines of the MAST; e.g.,
thoracic trauma.
5. Do not use MAST as a splint unless "indications" (above) are present.
Procedure
1. Remove outer clothing and examine lower half of body.
2. Apply MAST.
3. Inflate leg chambers fully, then check blood pressure.
4. If BP <100, inflate abdominal chamber fully and recheck blood pressure.
5. Monitor vital signs every 5 minutes.
Reference #33: MAST/PASG
55
Oxygen Delivery and Ventilation Devices
Reference #34: O
2
Administration Chart
Method Flow Rate Percent O
2
Delivered
Room Air 21%
1 LPM 24%
2 LPM 28%
4 LPM 36%
Nasal Cannula
6 LPM 44%
Non-Rebreather Mask 10 - 15 LPM 80 - 90%
10 LPM 50% Pocket Mask
15 LPM 80%
Bag-Valve-Mask (with
Reservoir)
12 - 15 LPM 90 - 100%
Flow-Restricted, Oxygen-
Powered Device (Positive
Pressure)
40 LPM 100%
Notes:
1. Administration rates through nasal cannula of over 4 LPM are
uncomfortable for the patient.
2. Use humidified O
2
on infants, children, suspected respiratory tract burns,
and transports exceeding one hour duration.
3. If bag-valve-mask is used in patient transport, the 2-rescuer technique may
be necessary to achieve adequate seal. If only one rescuer is available,
the
pocket mask and/or the flow-restricted, oxygen-powdered device is
preferred.
4. Pressure cycled ventilators are NOT acceptable alternatives for O
2
therapy.
5. Percentages of delivered O
2
listed above are based on optimal conditions.
Altitude, equipment, etc., may significantly decrease percentages of
delivered O
2
.
56
Oxygen Cylinders
Bottle Size Volume in Liters Time @ 5 LPM Time @ 10 LPM Time @ 15 LPM
D 360 1 hr., 12 min. 36 min. 24 min.
625 2 hrs., 5 min. 1 hr., 3 min. 42 min. E
3,200 10 hrs. 5 hrs. 3 hrs., 20 min. M
5,300 17 hrs., 40 min. 8 hrs., 50 min. 5 hrs., 53 min. G
6,900 23 hrs. 11 hrs., 30 min. 7 hrs., 40 min. H
The above values are based on full bottle (2,000 - 2,200 psi) at 70F.
Allow for pressure drop of 5 psi for every 1 degree drop in temperature below 70F. This amounts to
approximately 10% reduction in volume at 32F or 18% reduction at OF.
57
Reference #35: Helpful Mnemonics
Brief Neurological Evaluation
A - Alert
V - Responds to Verbal stimuli
P - Responds to Painful stimuli
U - Unresponsive
Medical History
S - Signs and Symptoms
A - Allergies
M - Medications
P - Past medical history
L - Last oral intake
E - Events preceding illness or injury
Pain Evaluation
O - Onset (activity when pain started)
P - Provokes or palliates (what makes pain worse or better)
Q - Quality (sharp, dull)
R - Region, radiation
S - Severity (1-10 scale)
T - Time (since onset of pain)
When to Stop CPR
H - Help arrives and responsibility is transferred
E - Exhaustion forces you to stop
L - Life signs appear
P - Physician assumes responsibility
Immediate Treatment of Sprains
I - Ice
C - Compression using bandage
E - Elevation of extremity
58
Reference #36: Radio/Phone Consultation
Receiving Hospital:
Unit #: Service Name
Patient age: Sex:
Chief Complaint (onset, duration, etc.):
LOC: Level of Distress:
Signs & Symptoms:
Pulse: Blood Pressure: Respirations:
Skin: Pupils: Lung Sounds:
EKG:
Other pertinent physical findings:
Pertinent past medical history:
Pertinent medications:
Pertinent allergies:
Patient physician:
Emergency care:
ETA: Enroute code:
59
Reference #37: Splints
The splints listed are commonly available. Other materials may be appropriate.
Dislocations
Site Type of Splint
Shoulder Sling and swathe or support and immobilize in most comfortable position for
patient.
Elbow Padded board splint, sling and swathe, padded wire ladder splint, elbow splint.
Wrist/Hand Padded board splint, padded wire ladder splint, splint hand in position of
function.
Hip Padded long board splint, scoop stretcher, long spine board.
Knee Padded board splint, long spine board, scoop stretcher.
Ankle Pillow or blanket.
Fractures
Site Type of Splint
Upper Arm Padded board splint or padded wire ladder splint with sling and swathe.
Forearm Padded board splint or padded wire ladder splint with sling and swathe, air or
vacuum splint.
Wrist/Hand Padded board splint or padded wire ladder splint with sling and swathe, air or
vacuum splint.
Pelvis Scoop stretcher, spine board.
Hip Long backboard with pillow between legs, scoop stretcher.
Femur Traction splint, long padded board splint.
Knee Padded board splint, air or vacuum splint.
Tibia/Fibula Padded board splint, air or vacuum splint.
Ankle/Foot Pillow, air or vacuum splint.
60
Normal ranges of arterial blood pressures (mmHg), normal pulse rates (heart beats per minute), and
normal respiratory rates (respirations per minute) for various ages can be found in the chart below.
Ages Systolic BP
Reference #38: Vital Signs
Diastolic BP Pulse Rate Resp. Rate
Newborn 80 46 110-150 30-50
6 - 12 months 89 60 100-140 20-30
1 year 96 66 90-110
2 years 98 64
3 years 100 68 80-120
4 years 98 66
5 - 6 years 94 56 80-100
6 - 7 years 100 56
8 - 9 years 106 58 70-110
9 - 10 years 108 58 14-22
10 - 11 years 112 58
11 - 12 years 114 60 60-100
12 - 13 years 116 60 12-20
13 - 14 years 118 60
Notes:
1. Systolic values given above may vary up or down
significantly and still remain in a normal range as follows:
Newborn Plus/minus 16
6 months-4 yrs Plus/minus 25
4-10 years Plus/minus 16
10-14 years Plus/minus 18
2. Diastolic values given above may vary from plus/minus 9
mmHg to plus/minus 24 mmHg and still remain in the
normal range.
61
Reference #39: Self-Protection and Personal Safety
Basic Protective Measures From Disease Transmission
1. Use disposable gloves on every ambulance run.
2. Use face mask/protective eye wear.
3. Use pocket mask with one way valve when doing rescue breathing.
4. Use isolation gowns when appropriate.
5. Frequent handwashing recommended.
6. Annual tuberculosis testing.
7. Annual health examinations.
8. Recommended immunizations.
a. Measles vaccine.
b. Rubella vaccine.
c. Tetanus-diphtheria vaccine.
d. Mumps vaccine.
e. Influenza vaccine.
f. Hepatitis B vaccine.
Protective Clothing and Equipment
1. The EMT will be exposed to a wide variety of conditions and should dress appropriately for the
weather and/or rescue; i.e., cold weather or rain clothing, bunker gear, etc.
62
Reference #40: Pulse Oximetry
A pulse oximeter is a portable device that measures oxygen saturation (SaO
2
). It works by applying the
probe to a part of the body with thin tissue that contains an arterial bed, such as an earlobe or fingertip.
One side emits light and the other detects light content after passing through the tissue. The percent of
hemoglobin saturated with oxygen is then expressed in digital form.
Pulse oximetry provides continuous assessment of oxygen saturation during transport, even during
vomiting, suctioning or intubation attempts. It also allows for assessment of perfusion distal to orthopedic
injuries and pulse oximetry is an excellent way of providing an accurate systolic blood pressure in noisy
environments like the back of an ambulance or helicopter.
The pulse oximeter should be applied during transport. The application should not prolong scene times.
Caution
The EMT should remember to always treat the patient--NOT the numbers obtained from the
monitor. Occasionally pulse oximetry results can be misleading; i.e., carbon monoxide poisoning,
hypothermia, and hypovolemia.
Normal readings are 95% or higher. In the prehospital setting, the EMT should administer oxygen to the
patient with a saturation of less than 90%, and increase the oxygen liter flow until the saturation is above
90%.
REMEMBER:
The victims of trauma, heart attack, GI bleeding, and carbon
monoxide poisoning should receive oxygen regardless of pulse
oximetry measurements.
63
Reference #41: Semi-Automatic External Difibrillation (AED)
1. Assess ABCs. If patient is in cardiac arrest, begin CPR.
2. Turn on the defibrillator and apply electrodes to the patient as indicated on the package. Attach
cables, identify the time of day, the date, yourself, and the history of the patient.
3. STOP CPR and push the "ANALYZE" button. Do not touch the patient. The advisory screen
will display either "SHOCK ADVISED" or "NO SHOCK ADVISED". If "SHOCK ADVISED", the
unit will automatically charge to 200 joules.
4. Insure that no one is touching the patient! When the advisory screen indicates "SHOCK
NOW" or "READY, PRESS TO SHOCK" clear the area by saying "Shocking on 3 . . . 1, 2, 3".
Press the defibrillator button and observe for patient movement.
5. Repeat Steps 3 and 4, delivering a second shock between 200-300J , and a third shock at 360J .
6. Check the pulse, and if no pulse, do CPR for one minute. During the minute of CPR, assure the
adequacy of ventilations and chest compressions. Insert an oropharyngeal airway if not already
done, and assure the use of a bag-valve-mask with 100% oxygen.
7. Recheck the pulse. If no pulse, repeat steps 3 and 4 until a total of six shocks have been
delivered (Shocks 3 through 6 shall be delivered at 360J ). Continue CPR if needed and transport
the patient after delivering six shocks.
8. If "NO SHOCK ADVISED" check pulse and do CPR for one minute. Recheck pulse and if no
pulse re-analyze. After three consecutive "NO SHOCK ADVISED" messages continue CPR if no
pulse and transport the patient.
9. If a pulse is felt at any time, assess respiratory status and blood pressure, and transport the
patient in recovery position. Assist ventilations as needed and closely monitor the ABCs.
10. Maintain frequent pulse checks. If at anytime you cannot find a pulse, push "ANALYZE" and start
the protocol over.
Notes:
1. DO NOT ATTEMPT TO ANALYZE WHILE THE PATIENT IS MOVING!
The ANALYZE button should only be pushed when the vehicle is
stopped and no one is touching the patient.
2. The AED SHOULD NOT be used on anyone under the age of 8, unless
they weigh 90 pounds or more. If either the age or weight criteria is
met, you may treat the patient.
64
Reference #42: Blood or Body Fluids Exposure
The reportable diseases and conditions that are transmitted by blood and body fluids and invesigated for
possible exposure are:
1. Hepatitis B and C and
2. Human Immunodeficiency Visure Infection (including immunodeficiency syndrom/AIDS).
Occupational exposure to bloodborne pathogens may occur as the result of a needlestick or other
penetrating puncture of the skin with a used needle or other item; or either a splatter or aerosol into the
eye, nose, or mouth or any significant contamination of an open wound or non-intact skill with blood or
body fulids.
Any ambulance personnel who have significant exposure to blood or body fluids while providing
emergency care to an ill or injured person shall notify by facsimile or telephone the Department of Health,
Office of Communicable Disease Preventon and Control following such exposure. The Communicable
Disease Office fax number is (605) 773-5509; telephone number is 1-800-592-1861 or (605) 773-3737.
Upon receiving the report , the Office of Communicable Disease Prevention and Control will contact the
exposed individual to evaluate the exposure, counsel, and make referral to a physician if indicated.
Ambulance personnel at risk of exposure to blood or body fluids, must follow univeral precautions as set
forth in Recommendations for Prevention of HIV Transmission in Health Care Settings, August 21, 1997;
updated J une 24, 1998, Center for Disease Control and Prevention.
.
65
Reference #43: Unusual or Rare Infectious Diseases Exposure
Ambulance personnel who may have been exposed to a serious infectious disease such as infectious
tuberculosis, diphtheria, meningcoccal disease, plague, or rabies may contact the Office of
Communicable Disease Prevention and Control. The Communicable Disease Office will investigate the
incident and make recommenations and referral for medical followup. The Communicable Disease Office
telephone number is 1-800-592-1861 or (605) 773-3737.
66
Pediatric Protocol #44: General Considerations
General Parent-Child Considerations
1. When caring for a child, you are also caring for the family; therefore, you have multiple patients.
2. Conscious children should be transported with a parent unless this interferes with patient care.
3. If the child has a life-threatening injury or illness, the EMT should use his/her own discretion as to
whether the parent(s) should ride in the ambulance.
4. Have the parent(s) hold the child and assist with patient care as much as possible.
5. Use open, honest dialogue with both the parent(s) and the child. Direct assessment questions to
the child if old enough to answer; then to the parent(s).
6. Calming and supporting the parent(s) will improve your ability to deal with the child.
Developmental Considerations
1. Newborns and infants (birth to one year of age).
a. Minimal stranger anxiety but still do not like being separated from parent(s).
b. Need to be kept warm.
c. Feel suffocated by an oxygen mask.
d. Assess chest and lungs first before child becomes agitated.
2. Toddlers (one to three years of age).
a. Do not like to be touched.
b. Do not like having clothing removed; replace clothing after examination.
c. Are afraid of pain.
d. Think their illness/injury is a punishment.
3. Preschool/School-age (three to twelve years of age).
a. Are afraid of blood.
b. Are afraid of pain.
c. Are afraid of permanent injury and disfigurement.
d. Are very modest.
67
4. Adolescents (12 to 18 years of age).
a. Like to be treated as adults.
b. Desire to be assessed privately, away from parents or guardians.
c. Fear disfigurement and permanent injury.
Assessment/Anatomical Differences
1. Smaller airways are easily occluded. Tongue is large relative to oral cavity and can more readily
cause an obstructed airway.
2. Do not hyperextend the neck when attempting to open the airway.
3. Infants are obligate nose-breathers, suction the nasopharynx first.
4. Children can compensate well for respiratory distress for a short period of time; then
decompensate due to immature respiratory muscles that rapidly become fatigued.
5. Children will also compensate for blood loss (shock) for a longer period of time than an adult,
then quickly decompensate. Children have a high index of suspicion for life threatening injuries.
6. Children have smaller blood volumes and are less tolerant of blood loss.
7. Children sustain different types of injuries than adults; i.e., child abuse, more frequent falls, sports
injuries, bicycle injuries, etc.
8. Vital signs vary greatly for children. (See Reference #38, page 61.) Use capillary refill to assess
perfusion up to the age of three. In children over three, take a blood pressure.
9. Use pediatric-sized equipment whenever possible.
10. Child abuse is the #1 cause of death in children under the age of one year. Adapt your
assessment and management. (See Pediatric Protocol #46, page 70.)
68
Pediatric Protocol #45: Altered Mental Status
Assessment
1. Perform a Patient Assessment as in Trauma Protocols #1 and #2, pages 1 and 4 and Medical
Protocol #14, page 19.
2. Relevant history.
a. Fever or recent illness.
b. Ingestion of medications, household toxins, alcohol, recreational drugs.
c. History of diabetes, epilepsy, febrile seizures.
d. History of headaches, unexplained vomiting.
3. Physical exam.
a. Pupillary response, equality, and reactivity.
b. Signs of head trauma; palpate the fontanel gently.
c. Assess for neck stiffness if no trauma suspected.
d. Assess skin carefully for rashes and/or bruises.
e. Do serial neurologic exams using the Glasgow coma scale. (See Reference #32,
page 54.).
Treatment
1. Focus on supporting the respiratory and circulatory status of the child.
2. For a child with a fever see Pediatric Protocol #47, page 72.
3. For a child with respiratory distress see Pediatric Protocol #48, page 73.
4. For a child having seizures see Pediatric Protocol #49, page 75.
5. For the pediatric trauma patient see Pediatric Protocol #50, page 76.
6. For any other suspected emergency see the specific adult protocol.
69
Pediatric Protocol #46: Child Abuse
Assessment
1. Perform Rapid Trauma Assessment. (See Trauma Protocol #2, page 4.)
2. Physical exam.
a. Signs of head injury including bulging fontanelle, altered mental status, skull fractures,
etc.
b. Abdominal injury from blunt trauma; i.e., punching.
c. Multiple fractures or fractures in various stages of healing.
d. Soft tissue injuries.
1) Slap marks, abrasions, contusions, and/or lacerations that match the item used.
2) Bruises in various stages of healing.
3) Bite marks showing the teeth size and pattern of the adult mouth.
4) Burn marks from cigarettes, "stocking" burn marks from being dipped in hot
water, and burns with clear demarcation matching the shape of the item used.
5) Bilateral burns; i.e., burns to both hands.
e. Injury to the genitalia.
f. Indications of past injuries including poorly healing wounds, improperly healed fractures,
and scars from past burns.
3. Note while taking a history.
a. Repeated responses to provide care for the same child or children in a family.
b. Inconsistencies or vagueness concerning what caused the child's injuries.
c. Delay in seeking medical attention.
d. Parents who are hostile or distant; parents who overwhelm the EMT with explanations;
parents who do not wish to leave child alone with the EMT; parents who tell conflicting or
changing stories.
e. The child is withdrawn, passive or depressed; the child expects no comfort from the
parents; the child has little or no reaction to pain.
Treatment
1. Reassure patient and provide emotional support.
2. Administer oxygen and treat for shock if indicated.
3. See specific protocols to treat other injuries as indicated.
70
4. If sexual assault is suspected refer to Trauma Protocol #12, page 17.
5. Do not accuse the parent(s) of child abuse. Report suspicions to emergency department
personnel (the physician and/or nurse) upon arrival at the hospital. Reporting suspected child
abuse is not a legal obligation; but it is a professional and moral obligation.
6. Thoroughly document findings, using objective words and phrases. Record observations on the
physical environment where the child was found, the parent-child attitudes and interactions as
well as any physical findings.
71
Pediatric Protocol #47: Fever/Hyperthermia
Assessment
1. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
2. Record skin color and condition, and take temperature.
3. In children less than two years old, take a rectal temperature. In children over two, temperature
may be taken orally or axillary. Be sure to record method used.
4. Contraindications to rectal temperatures are rectal bleeding, abdominal distention, history of
bleeding disorder, and an uncooperative child.
5. Obtain pertinent history. Ask about administration of acetaminophen or other over-the-counter
medications.
Treatment
1. Administer 100% oxygen via non-rebreather mask.
2. Treat for shock as needed.
3. If temperature is over 102F (38.5C) orally, remove clothing and cover lightly with a sheet.
4. If temperature is over 104F (40C) orally, sponge skin with room temperature water while enroute
to the hospital. Use discretion in cold weather.
5. If patient has a seizure refer to Pediatric Protocol #49, page 75.
72
Pediatric Protocol #48: Respiratory Distress
Assessment
1. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
2. Assess and determine adequacy of airway and ventilation.
a. Mental status.
b. Skin color and condition.
c. Heart rate and respiratory rate and depth.
d. Lung sounds and expiratory grunting.
e. Use of accessory muscles and "see-saw" breathing.
f. Nasal flaring and intercostal retractions.
g. Position.
3. Obtain a history.
a. Abrupt or gradual onset.
b. Fever or other infectious symptoms.
c. Difficulty swallowing, voice change, drooling.
d. Previous medical history; i.e., asthma, prematurity, heart disease.
e. Playing with small objects/eating.
Treatment
Possible Foreign Body Obstruction
1. Follow "foreign body airway obstruction management" per American Heart Association
Standards.
Epiglottitis/Croup
1. Minimize the child's anxiety as much as possible by allowing parent to hold child and allowing
child to sit upright or in position of comfort.
2. Administer high-flow oxygen to the child, preferably by non-rebreather mask. Use blow-by
technique if necessary. Cool, humidified oxygen will relieve some of the distress associated with
croup.
3. Minimize interventions (oral airway, suctioning, visualizing the throat) to avoid laryngospasm and
complete airway obstruction.
4. If child becomes completely obstructed, attempt bag-valve-mask ventilation with 100% oxygen
using the two-rescuer technique. This usually provides adequate air exchange.
73
Asthma
1. Administer oxygen by non-rebreather mask at 15 LPM or as tolerated by the child.
2. If the child has a prescribed inhaler, assist with administration. (See Medical Protocol #23b,
page 40.)
74
Pediatric Protocol #49: Seizures
Assessment
1. Perform Patient Assessment. (See Medical Protocol #14, page 19.)
2. Physical exam assessment.
a. Bulging fontanel, stiff neck, rash (all suggestive of meningitis).
b. Signs of head trauma.
c. Focal seizure activity, eye deviation, weakness or paralysis of an extremity during the
postictal period (suggestive of an intracranial hematoma or tumor).
3. Relevant history.
a. Fever and previous seizures with fever.
b. Recent head trauma.
c. Most recent ingestion. List all medications found at the scene.
d. Diabetes or epilepsy. Taking medications as prescribed.
Treatment
1. Establish airway and administer oxygen per non-rebreather as tolerated.
2. Protect child during seizure by moving objects away from the patient.
3. Place patient in recovery position and be prepared to suction.
4. For a febrile seizure refer to Pediatric Protocol #47, page 72.
75
Pediatric Protocol #50: Trauma
Assessment
1. Perform Rapid Trauma Assessment for adults. (See Trauma Protocol #2, page 4.)
2. Be aware of anatomical and developmental differences in children.
a. Head: Head injuries cause over half of pediatric trauma deaths and 75% of all pediatric
trauma involves head injury. The head is larger in proportion to the rest of the body and
children are more likely to have cerebral swelling than adults.
b. Chest: The chest wall is more elastic; therefore, a child can have significant internal
injury with no obvious external injury. Rib fractures are less common; pulmonary
contusions more common.
c. Abdomen: The liver and spleen are proportionately larger and are less protected by the
rib cage, and therefore more susceptible to injury.
d. Extremities: Because bone growth is still occurring in children, long bone injuries can
result in serious disability if not managed properly. Long bone fractures and pelvis
injuries can result in blood loss that is proportionately greater than in an adult.
Treatment
1. Support respiratory and circulatory status. (See Trauma Protocol #11, page 16.)
a. Use modified jaw thrust to open airway, administer 100% oxygen per non-rebreather,
suction; assist ventilations as needed.
b. Control bleeding and treat for shock.
c. If MAST are used, use the appropriate pediatric size; do not inflate the abdominal
compartment.
2. Provide spinal immobilization.
a. Use appropriate sized cervical collars and immobilization equipment.
1) If collar does not fit, immobilize with towel rolls.
2) When using an adult backboard, pad under child from shoulders to heels in order
to compensate for large occipital area of head. Use adequate padding to fill
gaps and voids; provide adequate immobilization.
b. Remove the child from the car seat if
1) The car seat is cracked, bent or otherwise damaged.
2) There are major injuries; i.e., full arrest, respiratory distress, serious head or
chest injury, uncontrolled bleeding.
c. Use of the car seat for immobilization.
1) Apply a collar or towel roll to stabilize the neck and use manual in-line
immobilization.
2) Stabilize the thoracic and lumbar spine using towels or blankets taped in place.
76
77
3) Immobilize the head using towel rolls taped in place.
4) Secure the car seat to the cot or captain's chair facing the rear of the ambulance
if the patient is under 20 lbs and facing the front of the ambulance if the patient is
over 20 lbs. NEVER place the car seat on the bench, as car seats are not
designed to sustain lateral forces.
Das könnte Ihnen auch gefallen
- GINA 2016 Teaching Slide SetDokument171 SeitenGINA 2016 Teaching Slide SetAndra DaNoch keine Bewertungen
- Laporan Kesehatan KebudayaanDokument8 SeitenLaporan Kesehatan KebudayaanAnonymous hvOuCjNoch keine Bewertungen
- 0,546 (P 0, 05) and Odds Ratio (OR) 1,385 To The 2 Hours Post Meal Blood Glucose LevelDokument1 Seite0,546 (P 0, 05) and Odds Ratio (OR) 1,385 To The 2 Hours Post Meal Blood Glucose LevelAnonymous hvOuCjNoch keine Bewertungen
- Physician Checklist: Stemi AlertDokument6 SeitenPhysician Checklist: Stemi AlertAnonymous hvOuCjNoch keine Bewertungen
- Book Reviews: Barrow-in-FurnessDokument2 SeitenBook Reviews: Barrow-in-FurnessAnonymous hvOuCjNoch keine Bewertungen
- Transam in It IsDokument56 SeitenTransam in It IsAnonymous hvOuCjNoch keine Bewertungen
- GINA PediatricPocket 2015 PDFDokument26 SeitenGINA PediatricPocket 2015 PDFAnonymous hvOuCjNoch keine Bewertungen
- Not Eke Pulau AnDokument67 SeitenNot Eke Pulau AnAnonymous hvOuCjNoch keine Bewertungen
- Family QuetionnaireDokument80 SeitenFamily QuetionnaireAnonymous hvOuCjNoch keine Bewertungen
- Progress in Understanding The Immunoathogenesis of Psoriasis PDFDokument17 SeitenProgress in Understanding The Immunoathogenesis of Psoriasis PDFAnonymous hvOuCjNoch keine Bewertungen
- Jurnal PsikiatriDokument82 SeitenJurnal PsikiatriTimotius SumampouwNoch keine Bewertungen
- Brainsci 03 00642 PDFDokument28 SeitenBrainsci 03 00642 PDFAnonymous hvOuCjNoch keine Bewertungen
- Approach Considerations MALARIADokument3 SeitenApproach Considerations MALARIAAnonymous hvOuCjNoch keine Bewertungen
- CH 09 SM10cDokument13 SeitenCH 09 SM10ciisisiisNoch keine Bewertungen
- Neurobiology of Suicide PDFDokument10 SeitenNeurobiology of Suicide PDFAnonymous hvOuCjNoch keine Bewertungen
- WHO Disability Grading Operational Definition PDFDokument8 SeitenWHO Disability Grading Operational Definition PDFAnonymous hvOuCjNoch keine Bewertungen
- Expression of Antigen Processing and Presenting Mollecules by Schwann Cell in Inflamatory NeuropathyDokument21 SeitenExpression of Antigen Processing and Presenting Mollecules by Schwann Cell in Inflamatory NeuropathyAnonymous hvOuCjNoch keine Bewertungen
- Clinical Evidence of Leprosy PDFDokument15 SeitenClinical Evidence of Leprosy PDFAnonymous hvOuCjNoch keine Bewertungen
- Annals of The 680: Rheumatic DiseasesDokument2 SeitenAnnals of The 680: Rheumatic DiseasesAnonymous hvOuCjNoch keine Bewertungen
- Psoriasis Geneticsbreking The BarrierDokument17 SeitenPsoriasis Geneticsbreking The BarrierAnonymous hvOuCjNoch keine Bewertungen
- Health and Quality of Life OutcomesDokument11 SeitenHealth and Quality of Life OutcomesAnonymous hvOuCjNoch keine Bewertungen
- Veen, Natasja Hye Jung Van - BewerktDokument162 SeitenVeen, Natasja Hye Jung Van - BewerktAnonymous hvOuCjNoch keine Bewertungen
- Qlis - Development of A Schizophrenia-Specific Quality-Of-Life ScaleDokument12 SeitenQlis - Development of A Schizophrenia-Specific Quality-Of-Life ScaleAnonymous hvOuCjNoch keine Bewertungen
- 2patients With Leprosy and The Suddn Appearance of Inflamation in TH Skin and New Sensory LossDokument5 Seiten2patients With Leprosy and The Suddn Appearance of Inflamation in TH Skin and New Sensory LossAnonymous hvOuCjNoch keine Bewertungen
- Carpal Tunnel Release 2010Dokument3 SeitenCarpal Tunnel Release 2010Anonymous hvOuCjNoch keine Bewertungen
- Reductions in Self-Injury Produced by Transcutaneous Electrical Nerve StimulationDokument4 SeitenReductions in Self-Injury Produced by Transcutaneous Electrical Nerve StimulationAnonymous hvOuCjNoch keine Bewertungen
- Wrist - Carpal Tunnel Syndrome OTDokument14 SeitenWrist - Carpal Tunnel Syndrome OTشاهين قريشيNoch keine Bewertungen
- WJR 6 284Dokument18 SeitenWJR 6 284Anonymous hvOuCjNoch keine Bewertungen
- 17 Outpatient Physical and Occupational Therapy Protocol Guidlines PDFDokument7 Seiten17 Outpatient Physical and Occupational Therapy Protocol Guidlines PDFAnonymous hvOuCjNoch keine Bewertungen
- 17 Outpatient Physical and Occupational Therapy Protocol Guidlines PDFDokument7 Seiten17 Outpatient Physical and Occupational Therapy Protocol Guidlines PDFAnonymous hvOuCjNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- SR Gpa DefinitionsDokument15 SeitenSR Gpa DefinitionsravishangkarNoch keine Bewertungen
- Nursing Manag BURNDokument34 SeitenNursing Manag BURNumi margi rahayuNoch keine Bewertungen
- Medscape Hypovolemic ShockDokument14 SeitenMedscape Hypovolemic ShockSarah Ovinitha100% (1)
- Tiki Taka CK SurgeryDokument50 SeitenTiki Taka CK SurgeryEmad MerganNoch keine Bewertungen
- Log Book NDOP-Oral Surgery Book 1BDokument22 SeitenLog Book NDOP-Oral Surgery Book 1BAmira Md Ludin50% (2)
- Interplay Between Disability Support and Damage Settlements Can Be ConfusingDokument1 SeiteInterplay Between Disability Support and Damage Settlements Can Be ConfusingBob NigolNoch keine Bewertungen
- Rp0807 - Perform Splinting Techniques Learning ObjectivesDokument7 SeitenRp0807 - Perform Splinting Techniques Learning ObjectivesMuhammad ZubairNoch keine Bewertungen
- Correlated Report and Action Plan - FinalDokument30 SeitenCorrelated Report and Action Plan - FinalOpenFileCGYNoch keine Bewertungen
- Ctas 1Dokument2 SeitenCtas 1Timie Navarro ReyesNoch keine Bewertungen
- GHGK SDokument48 SeitenGHGK SAnonymous Syr2mlNoch keine Bewertungen
- American College of Surgeons Committee On TraumaDokument10 SeitenAmerican College of Surgeons Committee On TraumaMauricio Castro AspeNoch keine Bewertungen
- Injury Prevention and Trauma Care DivisionDokument8 SeitenInjury Prevention and Trauma Care DivisionMohammedNoch keine Bewertungen
- Closed Intramedullary Nailing of Femoral Fractures PDFDokument12 SeitenClosed Intramedullary Nailing of Femoral Fractures PDFAnuta GiurgiNoch keine Bewertungen
- Abdominal TraumaDokument34 SeitenAbdominal Traumalaurz95Noch keine Bewertungen
- Oms - New WhoDokument77 SeitenOms - New WhoLuis Ferdinand Dacera-Gabronino Gamponia-NonanNoch keine Bewertungen
- Base ExcessDokument10 SeitenBase ExcessOrion JohnNoch keine Bewertungen
- Management of Musculoskeletal DisordersDokument69 SeitenManagement of Musculoskeletal DisordersJSeasharkNoch keine Bewertungen
- MCQs Surgery 1Dokument4 SeitenMCQs Surgery 1Asim NiazNoch keine Bewertungen
- New Initial Management in TraumaDokument69 SeitenNew Initial Management in TraumaSanthanu SukumaranNoch keine Bewertungen
- Traumatic Punctured Wound of Crop in A PigeonDokument2 SeitenTraumatic Punctured Wound of Crop in A PigeonArif K BashaNoch keine Bewertungen
- Initial Assessment and ManagementDokument13 SeitenInitial Assessment and ManagementterriNoch keine Bewertungen
- Stress Ulcer ProphylaxisDokument24 SeitenStress Ulcer ProphylaxisredyhataNoch keine Bewertungen
- 300 20Dokument3 Seiten300 20Christian JohnsonNoch keine Bewertungen
- Chapter 12, Transfer To Definitive CareDokument13 SeitenChapter 12, Transfer To Definitive CareDeka Dharma PutraNoch keine Bewertungen
- ATS Description NewDokument2 SeitenATS Description NewQuality Department Al Amal HospitalNoch keine Bewertungen
- ATLSDokument4 SeitenATLSTerri Sandi Susyanto73% (11)
- 2016 EMS Protocols IOWADokument104 Seiten2016 EMS Protocols IOWATasi'ah Nashirah NurNoch keine Bewertungen
- Nutrition Support in Critically Ill PatientDokument19 SeitenNutrition Support in Critically Ill PatienttantoNoch keine Bewertungen
- Case 1: Maxillofacial Trauma AND Airway in Maxillofacial TraumaDokument37 SeitenCase 1: Maxillofacial Trauma AND Airway in Maxillofacial Traumapolin timiselaNoch keine Bewertungen
- Police Magazine 2016 Buyers GuideDokument46 SeitenPolice Magazine 2016 Buyers GuidejasonNoch keine Bewertungen