Das könnte Ihnen auch gefallen
- Emergency DrugsDokument10 SeitenEmergency DrugsRoland Mark Rodel LagosNoch keine Bewertungen
- Heart of the Field "Refresher & Nha Certification Quick Notes"Von EverandHeart of the Field "Refresher & Nha Certification Quick Notes"Noch keine Bewertungen
- Dimensional Analysis For Nursing StudentsVon EverandDimensional Analysis For Nursing StudentsNoch keine Bewertungen
- Opioid Analgesics: T. Binder Department of PharmacologyDokument36 SeitenOpioid Analgesics: T. Binder Department of PharmacologywwwrgrobinNoch keine Bewertungen
- Haemodynamic Monitoring & Manipulation: an easy learning guideVon EverandHaemodynamic Monitoring & Manipulation: an easy learning guideNoch keine Bewertungen
- PMS-morphine clinical worksheetDokument1 SeitePMS-morphine clinical worksheetMichael Kuzbyt100% (1)
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingVon EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNoch keine Bewertungen
- Project On SamsungDokument39 SeitenProject On SamsungAbbas0% (1)
- Pain Management in Surgical PatientsDokument35 SeitenPain Management in Surgical Patientssuleman2009100% (1)
- FentanylDokument2 SeitenFentanylKatie McPeek63% (8)
- Line Sets in Oracle Order ManagementDokument9 SeitenLine Sets in Oracle Order ManagementS S PatelNoch keine Bewertungen
- Client Information Sheet (CIS)Dokument10 SeitenClient Information Sheet (CIS)Christine RombawaNoch keine Bewertungen
- Task Based Risk Assesment FormDokument2 SeitenTask Based Risk Assesment FormKolluri SrinivasNoch keine Bewertungen
- Proposed Construction of New Kutulo Airstrip - RetenderDokument112 SeitenProposed Construction of New Kutulo Airstrip - RetenderKenyaAirportsNoch keine Bewertungen
- Oxycodone Acetaminophen PercocetDokument1 SeiteOxycodone Acetaminophen PercocetENoch keine Bewertungen
- Drug MetoprololDokument1 SeiteDrug MetoprololSrkocher0% (1)
- DilaudidDokument2 SeitenDilaudidAdrianne Bazo100% (2)
- Tramadol Drug StudyDokument3 SeitenTramadol Drug StudyAnn Michelle Tarrobago100% (1)
- SEDATION and ANALGESIA in The PICU - Bijapur - Dr. Anand BhutadaDokument64 SeitenSEDATION and ANALGESIA in The PICU - Bijapur - Dr. Anand BhutadacrplzNoch keine Bewertungen
- 15 04 06 SCDokument30 Seiten15 04 06 SCSugarNoch keine Bewertungen
- TIVA - Copy (2) - Copy-1Dokument34 SeitenTIVA - Copy (2) - Copy-1Keerthikumar Parvatha100% (2)
- Employee Training and DevelopmentDokument33 SeitenEmployee Training and DevelopmentMoogii50% (2)
- Sedation in Critically IllDokument32 SeitenSedation in Critically IllSamantha Deshapriya100% (1)
- PCA For ICUDokument41 SeitenPCA For ICUMarina ShliginNoch keine Bewertungen
- Pca PP Revised 6 4 14 v6Dokument12 SeitenPca PP Revised 6 4 14 v6api-244230664Noch keine Bewertungen
- Postoperative AnalgesiaDokument38 SeitenPostoperative AnalgesiaKomella PrakasamNoch keine Bewertungen
- ICU Sedation and Analgesia GuideDokument10 SeitenICU Sedation and Analgesia GuideAvi CNoch keine Bewertungen
- Factors Influencing PainDokument81 SeitenFactors Influencing Painlorella_abejuelaNoch keine Bewertungen
- Patient Controlled AnalgesiaDokument35 SeitenPatient Controlled AnalgesiamochkurniawanNoch keine Bewertungen
- 5 Dosages, Solution & CalculationDokument50 Seiten5 Dosages, Solution & CalculationPrince Rener Velasco PeraNoch keine Bewertungen
- Patient Controlled AnalgesiaDokument26 SeitenPatient Controlled AnalgesiaSabah AlungalNoch keine Bewertungen
- COX-2 Inhibitors: Examples Parecoxib (Dynastat) Celecoxib (Celebrex) Etoricoxib (Arcoxia)Dokument31 SeitenCOX-2 Inhibitors: Examples Parecoxib (Dynastat) Celecoxib (Celebrex) Etoricoxib (Arcoxia)Ben Man JunNoch keine Bewertungen
- Spontaneous Awakening Trial PDFDokument1 SeiteSpontaneous Awakening Trial PDFyonoNoch keine Bewertungen
- Catapres Clonidine Drug CardDokument1 SeiteCatapres Clonidine Drug CardSheri490Noch keine Bewertungen
- Pca PP Revised 7 7 14 v7Dokument12 SeitenPca PP Revised 7 7 14 v7api-244230664Noch keine Bewertungen
- MEDICATION: Generic: Albuterol Trade: Proventil HFA, Ventolin DiskusDokument2 SeitenMEDICATION: Generic: Albuterol Trade: Proventil HFA, Ventolin Diskuszhulieta angovaNoch keine Bewertungen
- Phenergan (Promethazine)Dokument1 SeitePhenergan (Promethazine)E100% (1)
- Intro Anesthesia 2019 Drugs WebDokument38 SeitenIntro Anesthesia 2019 Drugs WebAbiNoch keine Bewertungen
- Nclex 3 With RationaleDokument13 SeitenNclex 3 With RationaleMsPocketbook HoarderNoch keine Bewertungen
- Patient Management Flow Chart: Appt W/ Bronchoscopist PFT/ P&H/StabilityDokument7 SeitenPatient Management Flow Chart: Appt W/ Bronchoscopist PFT/ P&H/StabilityKinnari PatelNoch keine Bewertungen
- Sedation and Analgesia ProtocolDokument5 SeitenSedation and Analgesia ProtocolBoston GunawanNoch keine Bewertungen
- NCP and RX StudyDokument13 SeitenNCP and RX StudyBinhafez Camlian DalhaniNoch keine Bewertungen
- XopenexDokument1 SeiteXopenexKatie McPeekNoch keine Bewertungen
- Ventilator Management ProtocolDokument15 SeitenVentilator Management Protocolihtisham1Noch keine Bewertungen
- Pain MXDokument7 SeitenPain MXRezaul KarimNoch keine Bewertungen
- Med Name: Mechanism of Action: Dosage: 10 MG Daily Priority Med Specific Patient TeachingDokument6 SeitenMed Name: Mechanism of Action: Dosage: 10 MG Daily Priority Med Specific Patient TeachingBrittany BennettNoch keine Bewertungen
- Managing pain with PercocetDokument2 SeitenManaging pain with PercocetKay TaylorNoch keine Bewertungen
- Patient Controlled AnalgesiaDokument129 SeitenPatient Controlled AnalgesiamehranerezvaniNoch keine Bewertungen
- DYSNEA ASSESSMENTDokument2 SeitenDYSNEA ASSESSMENTKang Opik TaufikNoch keine Bewertungen
- Med Template - Hydro Morph One Hydro Chloride (Hydromorphone Contin, Dilaudid)Dokument2 SeitenMed Template - Hydro Morph One Hydro Chloride (Hydromorphone Contin, Dilaudid)Ashlee KeeferNoch keine Bewertungen
- Practice - Exam - .Docx 8Dokument1 SeitePractice - Exam - .Docx 8jaloaliniskiNoch keine Bewertungen
- Naloxone (Narcan)Dokument2 SeitenNaloxone (Narcan)Adrianne BazoNoch keine Bewertungen
- Case Study 1Dokument3 SeitenCase Study 1Amberly BohackNoch keine Bewertungen
- DarvacetDokument1 SeiteDarvacetAdrianne BazoNoch keine Bewertungen
- NCP PROPER Pain and Decreased Cardiac OutputDokument3 SeitenNCP PROPER Pain and Decreased Cardiac OutputErienne Lae Manangan - CadalsoNoch keine Bewertungen
- JCI Accreditation Presentation 3Dokument77 SeitenJCI Accreditation Presentation 3Osama MarzoukNoch keine Bewertungen
- Ketamine Infusion For CRPS or Opioid Weaning GuidelineDokument14 SeitenKetamine Infusion For CRPS or Opioid Weaning GuidelineAlia SandoQaNoch keine Bewertungen
- Night Float VADokument9 SeitenNight Float VAkirNoch keine Bewertungen
- Drug Study: PART 1: To Be Completed Prior To Clinical ExperienceDokument5 SeitenDrug Study: PART 1: To Be Completed Prior To Clinical ExperienceFrozanSNoch keine Bewertungen
- Epidurals & PCAs: Understanding Pain Management OptionsDokument19 SeitenEpidurals & PCAs: Understanding Pain Management OptionsAdrian RodriguezNoch keine Bewertungen
- MEDICAL MANAGEMENTDokument12 SeitenMEDICAL MANAGEMENTMaricris Tubig LeritNoch keine Bewertungen
- DrugsDokument5 SeitenDrugsnurse_nurseNoch keine Bewertungen
- Symph A To Mimetic SDokument27 SeitenSymph A To Mimetic Sjl frusaNoch keine Bewertungen
- Neonatal Icu Skills ChecklistDokument5 SeitenNeonatal Icu Skills ChecklistsparticuslivesNoch keine Bewertungen
- Today 5Dokument1 SeiteToday 5sparticuslivesNoch keine Bewertungen
- CEN Brochure SAFH InformationDokument3 SeitenCEN Brochure SAFH InformationsparticuslivesNoch keine Bewertungen
- Expense Analysis WorksheetDokument2 SeitenExpense Analysis WorksheetsparticuslivesNoch keine Bewertungen
- Expense Analysis WorksheetDokument2 SeitenExpense Analysis WorksheetsparticuslivesNoch keine Bewertungen
- CEN Brochure SAFH InformationDokument3 SeitenCEN Brochure SAFH InformationsparticuslivesNoch keine Bewertungen
- Expense Analysis WorksheetDokument2 SeitenExpense Analysis WorksheetsparticuslivesNoch keine Bewertungen
- Expense Analysis WorksheetDokument2 SeitenExpense Analysis WorksheetsparticuslivesNoch keine Bewertungen
- Cardiovascular ReviewDokument8 SeitenCardiovascular ReviewsparticuslivesNoch keine Bewertungen
- EndocrineDokument2 SeitenEndocrinesparticuslivesNoch keine Bewertungen
- Expense Analysis WorksheetDokument2 SeitenExpense Analysis WorksheetsparticuslivesNoch keine Bewertungen
- Cardiovascular ReviewDokument8 SeitenCardiovascular ReviewsparticuslivesNoch keine Bewertungen
- EndocrineDokument2 SeitenEndocrinesparticuslivesNoch keine Bewertungen
- EndocrineDokument2 SeitenEndocrinesparticuslivesNoch keine Bewertungen
- EndocrineDokument2 SeitenEndocrinesparticuslivesNoch keine Bewertungen
- Criteria For INACTIVE MRSA StatusDokument2 SeitenCriteria For INACTIVE MRSA StatussparticuslivesNoch keine Bewertungen
- Cardiovascular ReviewDokument8 SeitenCardiovascular ReviewsparticuslivesNoch keine Bewertungen
- Cardiovascular ReviewDokument8 SeitenCardiovascular ReviewsparticuslivesNoch keine Bewertungen
- Explanation of AbbreviationsDokument1 SeiteExplanation of AbbreviationssparticuslivesNoch keine Bewertungen
- Vascular Disorders CH 38Dokument6 SeitenVascular Disorders CH 38sparticuslives100% (1)
- Vascular Disorders CH 38Dokument6 SeitenVascular Disorders CH 38sparticuslives100% (1)
- Explanation of AbbreviationsDokument1 SeiteExplanation of AbbreviationssparticuslivesNoch keine Bewertungen
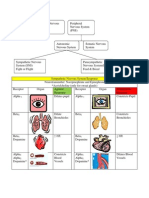
- CNS PNS Autonomic Nervous Systems SNS PNS Receptors ResponsesDokument3 SeitenCNS PNS Autonomic Nervous Systems SNS PNS Receptors ResponsesKara Dawn MasonNoch keine Bewertungen
- Vascular Disorders CH 38Dokument6 SeitenVascular Disorders CH 38sparticuslives100% (1)
- ANS ChartDokument3 SeitenANS ChartsparticuslivesNoch keine Bewertungen
- CNS PNS Autonomic Nervous Systems SNS PNS Receptors ResponsesDokument3 SeitenCNS PNS Autonomic Nervous Systems SNS PNS Receptors ResponsesKara Dawn MasonNoch keine Bewertungen
- PCA and Epidural Presentation Outline 2014Dokument10 SeitenPCA and Epidural Presentation Outline 2014sparticuslives100% (1)
- Explanation of AbbreviationsDokument1 SeiteExplanation of AbbreviationssparticuslivesNoch keine Bewertungen
- Explanation of AbbreviationsDokument1 SeiteExplanation of AbbreviationssparticuslivesNoch keine Bewertungen
- Refractomax 521 Refractive Index Detector: FeaturesDokument2 SeitenRefractomax 521 Refractive Index Detector: FeaturestamiaNoch keine Bewertungen
- Chapter 4-Ohm's LawDokument12 SeitenChapter 4-Ohm's LawErin LoveNoch keine Bewertungen
- Mid Semester ExaminationDokument2 SeitenMid Semester ExaminationMOHAMMED RIHANNoch keine Bewertungen
- Piroxicam (Wikipedia)Dokument4 SeitenPiroxicam (Wikipedia)Adrian ArnasaputraNoch keine Bewertungen
- MCQ 14 Communication SystemsDokument21 SeitenMCQ 14 Communication SystemsXeverus RhodesNoch keine Bewertungen
- Daa M-4Dokument28 SeitenDaa M-4Vairavel ChenniyappanNoch keine Bewertungen
- GE's Two-Decade Transformation: Jack Welch's Leadership: Amanda Rodriguez Patricia Robledo Brittany Culberson Yue JiangDokument34 SeitenGE's Two-Decade Transformation: Jack Welch's Leadership: Amanda Rodriguez Patricia Robledo Brittany Culberson Yue JiangRishendra Singh RathourNoch keine Bewertungen
- OTA710C User ManualDokument32 SeitenOTA710C User ManualEver Daniel Barreto Rojas100% (2)
- 7 ways to improve energy efficiency of pumpsDokument1 Seite7 ways to improve energy efficiency of pumpsCharina Malolot VillalonNoch keine Bewertungen
- Lecture 2 Leader-Centred PerspectivesDokument24 SeitenLecture 2 Leader-Centred PerspectivesLIVINGSTONE CAESARNoch keine Bewertungen
- Project IGI 2 Cheat Codes, Hints, and HelpDokument4 SeitenProject IGI 2 Cheat Codes, Hints, and Helppadalakirankumar60% (5)
- What Is Propaganda DeviceDokument3 SeitenWhat Is Propaganda DeviceGino R. Monteloyola100% (1)
- Holmes 1993Dokument8 SeitenHolmes 1993Rumaisa KrubaNoch keine Bewertungen
- Smart Card PresentationDokument4 SeitenSmart Card PresentationNitika MithalNoch keine Bewertungen
- 2021 A Review of Image Based Pavement Crack Detection AlgorithmsDokument7 Seiten2021 A Review of Image Based Pavement Crack Detection Algorithmsgandhara11Noch keine Bewertungen
- Rural Perception of SUV CarsDokument29 SeitenRural Perception of SUV CarsritusinNoch keine Bewertungen
- Siemens ProjectDokument17 SeitenSiemens ProjectMayisha Alamgir100% (1)
- Indian companies involved in trade dispute caseDokument15 SeitenIndian companies involved in trade dispute caseakshay daymaNoch keine Bewertungen
- How To Block Facebook in Mikrotik Using L7 Protocols (Layer 7) - Lazy Geek - )Dokument11 SeitenHow To Block Facebook in Mikrotik Using L7 Protocols (Layer 7) - Lazy Geek - )oscar_198810Noch keine Bewertungen
- Dhabli - 1axis Tracker PVSYSTDokument5 SeitenDhabli - 1axis Tracker PVSYSTLakshmi NarayananNoch keine Bewertungen
- Rheomix 141Dokument5 SeitenRheomix 141Haresh BhavnaniNoch keine Bewertungen
- Understanding Nominal Pipe Sizes (NPS) and Pipe DimensionsDokument39 SeitenUnderstanding Nominal Pipe Sizes (NPS) and Pipe DimensionsprathikNoch keine Bewertungen
- Consumer Preference and Demand For Rice Grain QualityDokument38 SeitenConsumer Preference and Demand For Rice Grain QualityIRRI_SSDNoch keine Bewertungen
- Sys Admin Guide Xerox WorkCentre 7775Dokument185 SeitenSys Admin Guide Xerox WorkCentre 7775dankorzon1Noch keine Bewertungen