Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- IV CannulationDokument22 SeitenIV Cannulationnaveen kumarNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Quick Reference Guide IAB Insertion CS300 Operation ENDokument36 SeitenQuick Reference Guide IAB Insertion CS300 Operation ENCatherine MorrisNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Royal Government of Bhutan Jigme Dorji Wangchuk National Referral Hospital Patient Discharge FormDokument2 SeitenRoyal Government of Bhutan Jigme Dorji Wangchuk National Referral Hospital Patient Discharge FormSuman Pradhan 2803Noch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Enfermedad MicrovascularDokument13 SeitenEnfermedad MicrovascularWindar BaqueroNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- ##Default - Genres.article## 28348 2 10 20210116Dokument14 Seiten##Default - Genres.article## 28348 2 10 20210116Vega VirlyNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Transport in Humans: 8.1 Need For Transport SystemDokument11 SeitenTransport in Humans: 8.1 Need For Transport Systemka klklklNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Differential Diagnosis of The Diseases With Systolic MurmursDokument2 SeitenDifferential Diagnosis of The Diseases With Systolic MurmursXiang Yun TanNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Hubungan Hipertensi Dengan Stroke Pada Pasien Poliklinik Neurologi RSUP Sanglah DenpasarDokument4 SeitenHubungan Hipertensi Dengan Stroke Pada Pasien Poliklinik Neurologi RSUP Sanglah DenpasarlidawatiNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- ECG Diagnosis: Right Ventricular Myocardial Infarction: Clinical MedicineDokument2 SeitenECG Diagnosis: Right Ventricular Myocardial Infarction: Clinical MedicineNadyaindriati96Noch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Taking Blood PressureDokument3 SeitenTaking Blood PressureApril Iren Claire BalabalaNoch keine Bewertungen
- NCP Anaphylactic ShockDokument6 SeitenNCP Anaphylactic ShockKirstin del CarmenNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Pathophysiology LeptospirosisDokument1 SeitePathophysiology Leptospirosisjeoffrey_castro100% (3)
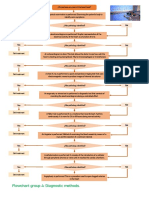
- Flowchart Group 4 Diagnostic Methods.Dokument1 SeiteFlowchart Group 4 Diagnostic Methods.Grupo 4 CardiologiaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Abdominal Vascular Injury - UpToDateDokument3 SeitenAbdominal Vascular Injury - UpToDateAnca StanNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Ineffective Tissue Perfusion - NCPDokument7 SeitenIneffective Tissue Perfusion - NCPVianah Eve EscobidoNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Model Nursing Early Warning System Score (Newss) Dengan Aplikasi Tehnologi Informasi Sebagai Pengkajian Deteksi Kegawatan Pada Klien Stroke Di Rs Kabupaten TangerangDokument12 SeitenModel Nursing Early Warning System Score (Newss) Dengan Aplikasi Tehnologi Informasi Sebagai Pengkajian Deteksi Kegawatan Pada Klien Stroke Di Rs Kabupaten Tangeranganggita putriNoch keine Bewertungen
- Anatomy MCQ - Abdomen - 2Dokument15 SeitenAnatomy MCQ - Abdomen - 2ahsan gujjarNoch keine Bewertungen
- Physiology Summary Chapter 20Dokument9 SeitenPhysiology Summary Chapter 20gail01850% (2)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- ESRD PathophysiologyDokument2 SeitenESRD PathophysiologyMark Ronhel Gallardo PerenalNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Sherif Mokhtar, MD: Professor of Cardiology, Professor of Critical Care Medicine Cairo UniversityDokument85 SeitenSherif Mokhtar, MD: Professor of Cardiology, Professor of Critical Care Medicine Cairo UniversityShimmering MoonNoch keine Bewertungen
- Diagnosis and Treatment of Peripheral Arterial DiseaseDokument5 SeitenDiagnosis and Treatment of Peripheral Arterial Diseasedrpiratheepan4274Noch keine Bewertungen
- What Is Angina?Dokument30 SeitenWhat Is Angina?Bentoys Street100% (1)
- Intracranial Aneurysms: An OverviewDokument12 SeitenIntracranial Aneurysms: An OverviewAnand KumarNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The UP-Philippine General Hospital Acute Coronary Events at The Emergency Room Registry (UP PGH-ACER)Dokument11 SeitenThe UP-Philippine General Hospital Acute Coronary Events at The Emergency Room Registry (UP PGH-ACER)Camille MalilayNoch keine Bewertungen
- Intracranial HemorrhageDokument34 SeitenIntracranial HemorrhageNaemanGötzNoch keine Bewertungen
- Rainer Kozlik-Feldmann, Georg Hansmann, Damien Bonnet, Dietmar Schranz, Christian Apitz, Ina Michel-BehnkeDokument7 SeitenRainer Kozlik-Feldmann, Georg Hansmann, Damien Bonnet, Dietmar Schranz, Christian Apitz, Ina Michel-BehnkeHerdinadNoch keine Bewertungen
- AHA Examination Auscultation Part IVDokument42 SeitenAHA Examination Auscultation Part IVHananya ManroeNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Krok 5Dokument53 SeitenKrok 5Wolf WolforNoch keine Bewertungen
- Acute Heart Failure WORKBOOKDokument28 SeitenAcute Heart Failure WORKBOOKFadhlan ABNoch keine Bewertungen
- Cyanotic Congenital Heart DiseaseDokument22 SeitenCyanotic Congenital Heart DiseaseRaviNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)