Das könnte Ihnen auch gefallen
- Writing Committee:: Guidelines For All Doctors in The Diagnosis and Management of Migraine and Tension-Type Headache 2004Dokument53 SeitenWriting Committee:: Guidelines For All Doctors in The Diagnosis and Management of Migraine and Tension-Type Headache 2004Yan Agus AchtiarNoch keine Bewertungen
- Dapus 2Dokument4 SeitenDapus 2Yan Agus AchtiarNoch keine Bewertungen
- Interpreting Chest X-Rays: Illustrated With 100 CasesDokument5 SeitenInterpreting Chest X-Rays: Illustrated With 100 CasesYan Agus AchtiarNoch keine Bewertungen
- Midland College Syllabus Fall 2008 RSPT 1307 Cardiopulmonary Anatomy and Physiology (3-0-0) Course DescriptionDokument6 SeitenMidland College Syllabus Fall 2008 RSPT 1307 Cardiopulmonary Anatomy and Physiology (3-0-0) Course DescriptionYan Agus AchtiarNoch keine Bewertungen
- Dapus 3Dokument10 SeitenDapus 3Yan Agus AchtiarNoch keine Bewertungen
- Jurnal Yan Agus FK UjDokument5 SeitenJurnal Yan Agus FK UjYan Agus AchtiarNoch keine Bewertungen
- Kedokteran 092010101002 Bambang PrabawigunaDokument6 SeitenKedokteran 092010101002 Bambang PrabawigunaYan Agus AchtiarNoch keine Bewertungen
- List Game Goman PC GamesDokument321 SeitenList Game Goman PC GamesYan Agus AchtiarNoch keine Bewertungen
- Abnormal Labor-ModifiedDokument8 SeitenAbnormal Labor-ModifiedListya NormalitaNoch keine Bewertungen
- Gyeke Et Al Paper 1 Vol 17 4Dokument18 SeitenGyeke Et Al Paper 1 Vol 17 4Yan Agus AchtiarNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- DH VSCC Intern Manual 4th Edition - WEB PDFDokument124 SeitenDH VSCC Intern Manual 4th Edition - WEB PDFXyzNoch keine Bewertungen
- GQ USA - March 2023Dokument120 SeitenGQ USA - March 2023davidtorrez1988Noch keine Bewertungen
- Neuroimaging Advances in Holoprosencephaly: Re Ning The Spectrum of The Midline MalformationDokument13 SeitenNeuroimaging Advances in Holoprosencephaly: Re Ning The Spectrum of The Midline Malformationfamiliesforhope100% (1)
- Intensive Care Unit (ICU)Dokument36 SeitenIntensive Care Unit (ICU)ruind99hjhkj100% (1)
- ACLSDokument275 SeitenACLSShajahan SideequeNoch keine Bewertungen
- Vasospasm: Endothelial Cell InjuryDokument4 SeitenVasospasm: Endothelial Cell InjuryPuja ArgaNoch keine Bewertungen
- Nutrition and AIDSDokument250 SeitenNutrition and AIDSLies Pramana SariNoch keine Bewertungen
- CAREGIVING NC II Lecture Week 6and 7Dokument15 SeitenCAREGIVING NC II Lecture Week 6and 7Ivy MagdayNoch keine Bewertungen
- Kanukula 2019Dokument7 SeitenKanukula 2019Dianne GalangNoch keine Bewertungen
- Sarcoidosis y UveitisDokument10 SeitenSarcoidosis y UveitisJavier Infantes MolinaNoch keine Bewertungen
- Preeclampsia and EclampsiaDokument24 SeitenPreeclampsia and EclampsiaAngel Marie TeNoch keine Bewertungen
- B Arab Board For Community Medicine Examination Edited 6 1Dokument115 SeitenB Arab Board For Community Medicine Examination Edited 6 1Sarah Ali100% (2)
- Bimanual Vaginal Examination - OSCE Guide - Geeky MedicsDokument6 SeitenBimanual Vaginal Examination - OSCE Guide - Geeky MedicsJahangir AlamNoch keine Bewertungen
- Correction of Severe Bimaxillary ProtrusionDokument37 SeitenCorrection of Severe Bimaxillary ProtrusionRobbyRamadhonieNoch keine Bewertungen
- NearfatalasthmaDokument8 SeitenNearfatalasthmaHeath HensleyNoch keine Bewertungen
- Pengaruh Pemberian Ropivakain Infiltrasi Terhadap Tampilan Kolagen Di Sekitar Luka Insisi Pada Tikus WistarDokument10 SeitenPengaruh Pemberian Ropivakain Infiltrasi Terhadap Tampilan Kolagen Di Sekitar Luka Insisi Pada Tikus WistarKunni MardhiyahNoch keine Bewertungen
- ThyrotoxicosisDokument16 SeitenThyrotoxicosisFiorella Peña MoraNoch keine Bewertungen
- 5.respiratory Distress Dental LectureDokument40 Seiten5.respiratory Distress Dental LecturehaneeneeNoch keine Bewertungen
- Case Study #3 Renal 1. LabDokument9 SeitenCase Study #3 Renal 1. Labapi-207971474Noch keine Bewertungen
- Blood Donation RequirementsDokument29 SeitenBlood Donation RequirementsMaria Cecilia FloresNoch keine Bewertungen
- Seattle Angina QuestionnaireDokument6 SeitenSeattle Angina QuestionnaireAmelia SianiparNoch keine Bewertungen
- Camh Suicide Prevention HandbookDokument96 SeitenCamh Suicide Prevention Handbook873810skah100% (3)
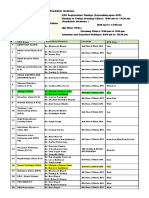
- OPD Schedule DoctorsDokument3 SeitenOPD Schedule DoctorssahilNoch keine Bewertungen
- b53 Swasa Kosa Mudra 07Dokument3 Seitenb53 Swasa Kosa Mudra 07shadowfalcon03Noch keine Bewertungen
- Assessment Diagnosis Goals and Objectives Planning Intervention Rationale EvaluationDokument3 SeitenAssessment Diagnosis Goals and Objectives Planning Intervention Rationale EvaluationCrissa AngelNoch keine Bewertungen
- English Drama ScriptDokument7 SeitenEnglish Drama ScriptNadia ASNoch keine Bewertungen
- Appenndix C CompleteDokument2 SeitenAppenndix C Completebrooksey2Noch keine Bewertungen
- Burns and ScaldsDokument14 SeitenBurns and ScaldsMuhamad IqbalNoch keine Bewertungen
- Manual Lifegain INGLESDokument207 SeitenManual Lifegain INGLESNicolás Di LulloNoch keine Bewertungen
- Symptoms: Products & ServicesDokument20 SeitenSymptoms: Products & ServicesLany T. CataminNoch keine Bewertungen