Das könnte Ihnen auch gefallen
- Relaxation ExercisesDokument14 SeitenRelaxation Exercisesnosheen murtazaNoch keine Bewertungen
- Hip Pain TreatmentDokument19 SeitenHip Pain TreatmentLev KalikaNoch keine Bewertungen
- 2020 Draft HSE Plan Ucd CampDokument17 Seiten2020 Draft HSE Plan Ucd Campbilo198450% (2)
- Check List - Air Compressor InspectionDokument1 SeiteCheck List - Air Compressor Inspectiondndudc100% (4)
- Acute Radiation SyndromeDokument18 SeitenAcute Radiation SyndromekitsilcNoch keine Bewertungen
- 059 Vacuum Truck SafetyDokument6 Seiten059 Vacuum Truck Safetyichal_zaidanNoch keine Bewertungen
- 360 MedSpa Client Information FormDokument3 Seiten360 MedSpa Client Information FormV Thomas PaulNoch keine Bewertungen
- Calcium Hypochlorite MSDSDokument5 SeitenCalcium Hypochlorite MSDStradeasiagroupNoch keine Bewertungen
- Lifting Hoisting Hazard HuntDokument1 SeiteLifting Hoisting Hazard Hunt曹庆园100% (1)
- Rigging Safety in Cranes PDFDokument170 SeitenRigging Safety in Cranes PDFLuis AcuaNoch keine Bewertungen
- SOP Excavation and PermittingDokument4 SeitenSOP Excavation and PermittingTengku & Wan ResourcesNoch keine Bewertungen
- Spill Kit HandlingDokument2 SeitenSpill Kit HandlingHanan SarwarNoch keine Bewertungen
- Forklift Jha Move Pallets Loads Around YardDokument5 SeitenForklift Jha Move Pallets Loads Around YardAhsan IqbalNoch keine Bewertungen
- Hydro Blasting 3Dokument6 SeitenHydro Blasting 3Robinson Ysasis100% (1)
- Safe Refueling ProcedureDokument8 SeitenSafe Refueling ProcedureABDUL RISHAD Kunduthode100% (1)
- Jsa FormDokument3 SeitenJsa Formmiaicarba100% (1)
- Pollution PortDokument49 SeitenPollution PortCorto MalteseNoch keine Bewertungen
- Driving and Journey Management ProcedureDokument6 SeitenDriving and Journey Management ProcedureRonny FitriadiNoch keine Bewertungen
- PD Reviewer 1st QuarterDokument5 SeitenPD Reviewer 1st Quarterandrian diazNoch keine Bewertungen
- Waste Management PolicyDokument16 SeitenWaste Management PolicyImran MahmudNoch keine Bewertungen
- 5 - Technical Specifications For Sand & Murrum Filling Works - Pile Foundation For Tanks - ParadeepDokument21 Seiten5 - Technical Specifications For Sand & Murrum Filling Works - Pile Foundation For Tanks - ParadeepArup NathNoch keine Bewertungen
- Jsa - LPG GasDokument8 SeitenJsa - LPG GasAsan IbrahimNoch keine Bewertungen
- HSEP 13 8 A1 Fall Prevention System Requirement Rev 5Dokument5 SeitenHSEP 13 8 A1 Fall Prevention System Requirement Rev 5mojgfdNoch keine Bewertungen
- Safety Manual HPWJDokument24 SeitenSafety Manual HPWJgshdavidNoch keine Bewertungen
- H2S Contingency PlanDokument33 SeitenH2S Contingency PlanAnonymous JMuM0E5YO100% (1)
- Plant Commissioning Start Up ProcedureDokument100 SeitenPlant Commissioning Start Up Proceduremsaad292% (124)
- Construction Presentation - Container Terminal PDFDokument60 SeitenConstruction Presentation - Container Terminal PDFdndudc100% (1)
- Oil+Spill+Response+and+Preparedness EngDokument19 SeitenOil+Spill+Response+and+Preparedness EngEdward Pitts100% (1)
- Nursing Care Plans All PresentationsDokument23 SeitenNursing Care Plans All PresentationsKaren Joyce Costales Magtanong100% (3)
- Cold Work PermitDokument11 SeitenCold Work PermitMuneeb Ur Rehman100% (1)
- National Energy Group of Companies: Project HSE PlanDokument4 SeitenNational Energy Group of Companies: Project HSE PlanalinkarrnyaNoch keine Bewertungen
- Rhino-FESS Carny Procedure-Guide en 42042Dokument64 SeitenRhino-FESS Carny Procedure-Guide en 42042Rijal SaputroNoch keine Bewertungen
- Hse Guide: Statement of Policy On Health, Safety and EnvironmentDokument2 SeitenHse Guide: Statement of Policy On Health, Safety and EnvironmenttissaanuradhaNoch keine Bewertungen
- Confind SpaceDokument11 SeitenConfind Spacesolomonbeg100% (1)
- Functional Specification Export Gas Compressor PDFDokument7 SeitenFunctional Specification Export Gas Compressor PDFdndudcNoch keine Bewertungen
- Pages 191 201 KressDokument11 SeitenPages 191 201 KressErik VenegasNoch keine Bewertungen
- Unity Health Safety ManualDokument19 SeitenUnity Health Safety ManualKakaraparti SatishNoch keine Bewertungen
- Study of Breakwaters Constructed With One Layer of Armor Stone PDFDokument58 SeitenStudy of Breakwaters Constructed With One Layer of Armor Stone PDFdndudcNoch keine Bewertungen
- Job Hazard Analysis Worksheet: Cold Cutting in Open AreaDokument2 SeitenJob Hazard Analysis Worksheet: Cold Cutting in Open AreaAbdul Hakam Mohamed Yusof0% (1)
- Quay Wall Construction PDFDokument8 SeitenQuay Wall Construction PDFdndudcNoch keine Bewertungen
- 2013 HSE Annual Report Web FINALDokument74 Seiten2013 HSE Annual Report Web FINALThiếu Nhiều Thứ100% (1)
- Wate ManagementDokument35 SeitenWate ManagementREMYANoch keine Bewertungen
- Gastroenterology Best RDokument23 SeitenGastroenterology Best RfrabziNoch keine Bewertungen
- Ras Abu Aboud Stadium & Precinct Project: Chemical Name Coshh MsdsDokument1 SeiteRas Abu Aboud Stadium & Precinct Project: Chemical Name Coshh Msdssharon Aisha malroy100% (1)
- Offshore Pipelaying Dynamic PDFDokument150 SeitenOffshore Pipelaying Dynamic PDFdndudcNoch keine Bewertungen
- Check List For Hse Marine Rig SurveyDokument5 SeitenCheck List For Hse Marine Rig SurveynadyNoch keine Bewertungen
- Quay Construction With Concrete Caisson PDFDokument5 SeitenQuay Construction With Concrete Caisson PDFdndudcNoch keine Bewertungen
- Environment ManagementDokument16 SeitenEnvironment ManagementMohamed HadjkacemNoch keine Bewertungen
- Job Hazard Analysis: Task/Procedure Hazard Safe ProcedureDokument2 SeitenJob Hazard Analysis: Task/Procedure Hazard Safe ProcedureKhairul MuzamilNoch keine Bewertungen
- Ra02 - Container OffloadingDokument3 SeitenRa02 - Container OffloadingSamNoch keine Bewertungen
- Anchor Handling Tug Pre-Mob InspectionDokument8 SeitenAnchor Handling Tug Pre-Mob Inspectiondndudc100% (1)
- Job Hazard Analysis (Jha) Worksheet: Installation/Facility Job Activity Location Description of Activity NoteDokument3 SeitenJob Hazard Analysis (Jha) Worksheet: Installation/Facility Job Activity Location Description of Activity NoteganeshkanthNoch keine Bewertungen
- Environmental TrainingDokument45 SeitenEnvironmental Trainingali128100% (1)
- SWP Lifting Operations and Lifting Equipment 22-12-10 v1 06Dokument7 SeitenSWP Lifting Operations and Lifting Equipment 22-12-10 v1 06Joozza MandaNoch keine Bewertungen
- Fall Protection Survey of RIG 40Dokument3 SeitenFall Protection Survey of RIG 40Kevin Josh Bonales100% (1)
- CD Manual 09Dokument99 SeitenCD Manual 09Matthew Ho100% (2)
- 1.9 - HSE Performance Monitoring Process & RecordsDokument5 Seiten1.9 - HSE Performance Monitoring Process & RecordsUnachukwu Sopulu SopsyNoch keine Bewertungen
- JHA Vessel EntryDokument2 SeitenJHA Vessel EntryRiyadh SalehNoch keine Bewertungen
- Hitra Procedure Kz01 CG Pro 53 0113 A02Dokument41 SeitenHitra Procedure Kz01 CG Pro 53 0113 A02odeinat100% (1)
- Offshore Personnel Transfer Safety ProceduresDokument24 SeitenOffshore Personnel Transfer Safety Proceduresegy pureNoch keine Bewertungen
- Offshore Book 2010Dokument117 SeitenOffshore Book 2010Mos Woraphon100% (1)
- Construction Quality ManualDokument42 SeitenConstruction Quality ManualBob Madlener100% (7)
- 185 Eng PDFDokument1 Seite185 Eng PDFHaleem Ur Rashid BangashNoch keine Bewertungen
- 9.0 HSSE Risk ManagementDokument10 Seiten9.0 HSSE Risk Managementsinghal.ns4497Noch keine Bewertungen
- Malaria Control Program (Hard Copy)Dokument10 SeitenMalaria Control Program (Hard Copy)JacqColumnaNoch keine Bewertungen
- Critical Path Method (CPM) in Project ManagementDokument11 SeitenCritical Path Method (CPM) in Project ManagementdndudcNoch keine Bewertungen
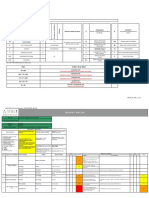
- Quality Procedure Technical Queries PDFDokument7 SeitenQuality Procedure Technical Queries PDFdndudc100% (2)
- PE001-Environment ManagementDokument14 SeitenPE001-Environment ManagementOgunwa EmmanuelNoch keine Bewertungen
- Functional Specification Diesel Fuel System PDFDokument5 SeitenFunctional Specification Diesel Fuel System PDFdndudcNoch keine Bewertungen
- The Neuroscience of Mindfulness Meditation.Dokument13 SeitenThe Neuroscience of Mindfulness Meditation.Peter van Kan100% (1)
- P-LUS-OCEMP-000: Overall Construction Environment Management PlanDokument158 SeitenP-LUS-OCEMP-000: Overall Construction Environment Management PlanRafzeena100% (1)
- Hygiene and Industrial ProcedureDokument4 SeitenHygiene and Industrial ProcedureNovida Rosalia Sinaga0% (1)
- Pre Mobilisation Checklist For Offshore TravellDokument3 SeitenPre Mobilisation Checklist For Offshore TravellUzair AhmedNoch keine Bewertungen
- Equipment Register - Pat Testing Original CertificateDokument3 SeitenEquipment Register - Pat Testing Original CertificateSayed AbbasNoch keine Bewertungen
- Ggupd-Nesma Sa4-Subcon-Safety Meeting - Week# 40Dokument9 SeitenGgupd-Nesma Sa4-Subcon-Safety Meeting - Week# 40Alok SinghNoch keine Bewertungen
- JSA - 003 - Tripod Rig Erection, Operation and DismantlingDokument2 SeitenJSA - 003 - Tripod Rig Erection, Operation and DismantlingAbhijit JanaNoch keine Bewertungen
- HSE Management Summary.Dokument2 SeitenHSE Management Summary.min thantNoch keine Bewertungen
- COVID-19 Prevention PlanDokument12 SeitenCOVID-19 Prevention PlanZubair KhanNoch keine Bewertungen
- REDACTED VERSION Oil Spill Contingency Plan (Approved by MCA) - Valid Until 17.05.2017Dokument102 SeitenREDACTED VERSION Oil Spill Contingency Plan (Approved by MCA) - Valid Until 17.05.2017gummy_langNoch keine Bewertungen
- Njqs Core Audit Module - Rev1.6cDokument14 SeitenNjqs Core Audit Module - Rev1.6cNene UmohNoch keine Bewertungen
- ED2 SampleDokument53 SeitenED2 SampleadelNoch keine Bewertungen
- Hsem-Sp-0014 Nidaa Journey ManagementDokument6 SeitenHsem-Sp-0014 Nidaa Journey ManagementAhmed Imtiaz RaoNoch keine Bewertungen
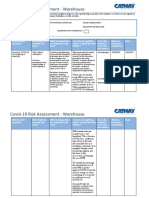
- Covid-19 RiskAssessmentWarehouseDokument11 SeitenCovid-19 RiskAssessmentWarehouseBalgo BalgobinNoch keine Bewertungen
- Details Required For ESIADokument2 SeitenDetails Required For ESIAbhaskarNoch keine Bewertungen
- HIRA in Process Safety PDFDokument16 SeitenHIRA in Process Safety PDFAlvin AlfiyansyahNoch keine Bewertungen
- JSA For Hydrojetting (Gun With Rigid Lance) at Jetting YardDokument23 SeitenJSA For Hydrojetting (Gun With Rigid Lance) at Jetting YardSHAH NAWAZ SAEEDNoch keine Bewertungen
- Cathodic Protection 2007Dokument141 SeitenCathodic Protection 2007arsssyNoch keine Bewertungen
- Primavera (P6)Dokument316 SeitenPrimavera (P6)Abde Ali83% (6)
- Metode Konstruksi Reklamasi PantaiDokument55 SeitenMetode Konstruksi Reklamasi PantaiHosea Luahambowo100% (1)
- Study of Reflection of New Low-Reflectivity Quay Wall Caisson PDFDokument11 SeitenStudy of Reflection of New Low-Reflectivity Quay Wall Caisson PDFdndudcNoch keine Bewertungen
- Behaviour of Reinforced Earth Behind Quay Walls PDFDokument9 SeitenBehaviour of Reinforced Earth Behind Quay Walls PDFdndudcNoch keine Bewertungen
- Congenital Malformations of The Genital Tract andDokument19 SeitenCongenital Malformations of The Genital Tract andabhinay_1712100% (1)
- Miliue Therapy Skill PDFDokument1 SeiteMiliue Therapy Skill PDFRosalinda SalvadorNoch keine Bewertungen
- UntitledDokument33 SeitenUntitledapi-257817850Noch keine Bewertungen
- LOCSINDokument15 SeitenLOCSINJham JhamNoch keine Bewertungen
- Jawt 11 I 2 P 48Dokument3 SeitenJawt 11 I 2 P 48Irma NoviantiNoch keine Bewertungen
- DR - Gold Created by SiraDokument26 SeitenDR - Gold Created by SiraMohamed ElhabetNoch keine Bewertungen
- PDF SMR OperationDokument64 SeitenPDF SMR OperationRizqulloh Taufiqul Hakim BarsahNoch keine Bewertungen
- The Hospital Team Week 1 12557Dokument25 SeitenThe Hospital Team Week 1 12557gladz25Noch keine Bewertungen
- Proses Persalinan Normal Eb1Dokument43 SeitenProses Persalinan Normal Eb1Cici RahmaNoch keine Bewertungen
- Chapter 1. History and Physical Examination - Art and ScienceDokument3 SeitenChapter 1. History and Physical Examination - Art and SciencecarolineNoch keine Bewertungen
- The American College of Radiology BI-RADS Atlas 5 Edition: Frequently Asked QuestionsDokument18 SeitenThe American College of Radiology BI-RADS Atlas 5 Edition: Frequently Asked QuestionssatanioNoch keine Bewertungen
- Adrenergic Antagonists EditedDokument60 SeitenAdrenergic Antagonists EditedJohn Benedict VocalesNoch keine Bewertungen
- AAMI Alarm - Compendium - 2015 PDFDokument68 SeitenAAMI Alarm - Compendium - 2015 PDFJJ MMNoch keine Bewertungen
- AcinobacterDokument2 SeitenAcinobacterAllyson Layaoen CollierNoch keine Bewertungen
- Internship of Summer Training ON Study of Opd Services in A Hospital Submitted By:-Salony Saha REGISTRATION NO.:-1476020 (FROM-1 July To 31Th August)Dokument14 SeitenInternship of Summer Training ON Study of Opd Services in A Hospital Submitted By:-Salony Saha REGISTRATION NO.:-1476020 (FROM-1 July To 31Th August)yugalkishorNoch keine Bewertungen
- Was Metrohealth Board Member Warned of Corruption - Medcity Newsmedcity NewsDokument7 SeitenWas Metrohealth Board Member Warned of Corruption - Medcity Newsmedcity Newsapi-303782712Noch keine Bewertungen
- First Tutorial: Brain StormingDokument3 SeitenFirst Tutorial: Brain Stormingsemicircularis0% (1)
- Daily Patient Assignment SheetDokument1 SeiteDaily Patient Assignment SheetSheferely BayauaNoch keine Bewertungen
- N N Burdenko Journal of Neurosurgery 2016-06Dokument108 SeitenN N Burdenko Journal of Neurosurgery 2016-06amereNoch keine Bewertungen