Beruflich Dokumente
Kultur Dokumente
The Effectiveness of Cigarette Regulations in Reducing Cases of Sudden Infant Death Syndrome
Hochgeladen von
Eugenio MartinezOriginalbeschreibung:
Originaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
The Effectiveness of Cigarette Regulations in Reducing Cases of Sudden Infant Death Syndrome
Hochgeladen von
Eugenio MartinezCopyright:
Verfügbare Formate
Journal of Health Economics 27 (2008) 106133
Available online at www.sciencedirect.com
The effectiveness of cigarette regulations in reducing
cases of Sudden Infant Death Syndrome
Sara Markowitz
Department of Economics, Rutgers University, 360 Dr. Martin Luther King Jr. Blvd.,
Newark and NBER, Newark NJ 07102, United States
Received 17 August 2006; received in revised form 26 March 2007; accepted 28 March 2007
Available online 8 April 2007
Abstract
Sudden Infant Death Syndrome (SIDS) is a leading cause of mortality among infants and is responsible
for thousands of infant deaths every year. Prenatal smoking and postnatal environmental smoke have been
identied as strong risk factors for SIDS. Given the link between smoking and SIDS, this paper examines
the direct effects of cigarette prices, taxes and clean indoor air laws in explaining changes in the incidence of
SIDS over time in the United States. State-level counts of SIDS cases are generated from death certicates
for 19732003. After controlling for some observed and unobserved confounding factors, the results show
that higher cigarette prices and taxes are associated with reductions in SIDS cases. Stronger restrictions on
smoking in workplaces, restaurants and child care centers are also effective in reducing SIDS deaths.
2007 Elsevier B.V. All rights reserved.
JEL classication: I0; J1
Keywords: SIDS; Infant health; Smoking; Cigarette taxes; Clean indoor air laws
1. Introduction
Sudden Infant Death Syndrome (SIDS) is the unexplained, sudden death of an infant under
1 year of age. SIDS is the leading cause of mortality among infants ages 112 months, and is
responsible for thousands of infant deaths every year (CDC, 2006a). Although much research has
been conducted on the correlates of SIDS and related risk factors, the underlying biologic causes
of SIDS are currently unknown (USDHHS, 2006). SIDS cases are usually identied through an
Tel.: +1 973 353 5350.
E-mail address: smarkow@rutgers.edu.
0167-6296/$ see front matter 2007 Elsevier B.V. All rights reserved.
doi:10.1016/j.jhealeco.2007.03.006
S. Markowitz / Journal of Health Economics 27 (2008) 106133 107
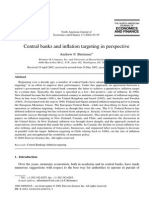
Fig. 1. National SIDS rates and cigarette prices.
autopsy that rules out other identiable causes of death. The standard denition of the syndrome
is the sudden death of an infant under 1 year of age, which remains unexplained after a thorough
case investigation, including performance of a complete autopsy, examination of the death scene,
and a review of the clinical history. (American Academy of Pediatrics [AAP] Task Force on
SIDS 2005, p. 1245).
Rates of SIDS in the United States have been steadily declining since 1980 (Fig. 1). Since
then, the number of SIDS cases has fallen from 1.53 per 1000 live births in 1980 to 0.53 per 1000
live births in 2003. The difculty in identifying the causes of SIDS makes it difcult to attribute
reasons for the decline. The Back to Sleep campaign, which recommends that infants should
be put to sleep in a supine position, has been widely cited for achieving signicant reductions in
SIDS in the U.S. (Willinger et al., 1998; Pickett et al., 2005; Anderson et al., 2005). However,
given that this campaign began in the mid-1990s, there is still much unknown about the trends,
causes, and prevention of this syndrome.
Suspected biological based causes of SIDS include abnormalities in the brains serotonin
system, abnormalities in autonomic regulation, and other genetic risk factors (Paterson et al., 2006;
Hunt and Hauck, 2006). Viral respiratory infections and complications during pregnancy, such
as placental abnormalities may also be contributing factors (Mage, 2004; Getahun et al., 2004).
Some researchers believe that the actual risk of SIDS results from a combination of biologic and
environmental or modiable risk factors (Filiano and Kinney, 1994; Hunt and Hauck, 2006). Much
of the current research on SIDS focuses on identifying the specic modiable risk factors that
are consistently observed to be associated with elevated risks of SIDS. The Centers for Disease
Control (CDC) summarizes seven primary risk factors: (1) tummy or side sleeping; (2) soft sleep
surfaces; (3) loose bedding; (4) overheating; (5) smoking; (6) bed sharing; and (7) preterm and
low birth weight (CDC, 2006b). The AAP adds that the use of paciers may reduce the risk and
young maternal age increases it (AAP Task Force on SIDS, 2005).
For many of the modiable risk factors, public education campaigns may be the only way
to encourage the behaviors that will reduce SIDS. For smoking, however, policy makers have a
108 S. Markowitz / Journal of Health Economics 27 (2008) 106133
variety of tools besides public education that can be used. Cigarette taxes and laws regulating
indoor smoking are known to be strong predictors of smoking behaviors among all adults and
pregnant women(Evans andRingel, 1999; Chaloupka andWarner, 2000; Tauras, 2006). If smoking
is truly a causal determinant of SIDS, whether it be direct or in conjunction with biologic factors,
then policies that reduce smoking should have the added benet of reducing SIDS cases. The
purpose of this paper, therefore, is to examine the direct effects of changes in cigarette prices,
taxes and clean indoor air laws in explaining changes in the incidence of SIDS over time in the
United States.
2. Smoking and SIDS
A number of studies from the U.S. and other countries around the world have established both
prenatal and postnatal smoking as major preventable risk factors for SIDS. In a comprehensive
review of this literature, Anderson and Cook (1997) nd that maternal smoking doubles the risk
of SIDS. They conclude the relationship is almost certainly causal. (p. 1003) The U.S. Surgeon
Generals 2006 report on the Health Consequences of Involuntary Exposure to Tobacco Smoke
concurs: The evidence is sufcient to infer a causal relationship between exposure to secondhand
smoke and Sudden Infant Death Syndrome. (p. 194).
The mechanism through which smoking inuences SIDS is not clear, although it is believed
that the immediate cause of death is through the cardiorespiratory system (Anderson and
Cook, 1997). During pregnancy, smoking may directly alter fetal oxygenation and development
(Schoendorf and Kiely, 1992), or it may affect birth weight, which can have a separate effect
on SIDS (CDC, 1991). After birth, smoking may lead to an irritation of the airway or respi-
ratory infections, and nicotine may affect ventilatory response functions (Anderson and Cook,
1997).
The literature on prenatal smoking and SIDS shows that the risk of dying from SIDS is much
higher for infants of mothers who smoked during pregnancy than for those with mothers who did
not smoke (Mitchell et al., 1993; Blair et al., 1996; Getahun et al., 2004; Anderson et al., 2005).
Anderson et al. (2005) attribute a range of 4880 percent of the observed SIDS deaths to prenatal
maternal smoking, even after controlling for other factors, such as birth weight, gestational age,
and certain maternal characteristics.
Postnatal smoking by either the mother or other household members also has been shown to
be a risk factor for SIDS. For example, case-control studies on maternal smoking postpartum
by Schoendorf and Kiely (1992), Mitchell et al. (1993), Klonoff-Cohen et al. (1995), Blair et
al. (1996) and others all nd a positive relationship between smoking and SIDS, even after
controlling for other risk factors, such as maternal characteristics, prenatal smoking, and, in some
studies, sleep position. The risk of death is also found to rise with increasing levels of smoking
(Mitchell et al., 1993; Blair et al., 1996). Anderson and Cook (1997) conducted a meta-analysis
of postnatal maternal smoking and found that smoking after pregnancy increases the risk of SIDS
by 94 percent. Klonoff-Cohen et al. (1995) specically examine maternal smoking in the same
room as the infant show even larger increases in the risk of SIDS over mothers who do not
smoke.
Smoking by fathers and other household members is also believed to be associated with an
increased risk of SIDS, although the evidence is not consistent across studies (USDHHS, 2006).
Controlling for maternal prenatal smoking, Klonoff-Cohen et al. (1995) and Blair et al. (1996) nd
that children in households with a non-smoking mother but a smoking father have a higher risk
of SIDS than children in households with non-smoking parents. Mitchell et al. (1993) also show
S. Markowitz / Journal of Health Economics 27 (2008) 106133 109
an increased risk for children in households where household members other than the mother or
father smoke, but this result does not hold in models that also include smoking by the parents.
However, studies by Brooke et al. (1997), Mitchell et al. (1997) and Alm et al. (1998) show
statistically insignicant effects for fathers smoking.
The above mentioned studies are all case-controlled studies that match families of infants who
died to a sample of control families with similar characteristics. Many studies are population
based, but often have small sample sizes and focus on restricted geographic areas. The results
of the multivariate studies may be biased if the smoking behaviors examined are correlated with
other unmeasured risky behaviors that remain in the error term. For example, if people who
smoke are less likely to follow the advice of doctors, then it is plausible that they might also
ignore the advice to put babies in the supine position for sleeping. The endogeneity problem is
particularly prevalent in studies of SIDS in the U.S. that use national level data, such as death
certicates or the National Maternal and Infant Health Survey, and do not contain information
on sleep position or other sleep-related behaviors (Schoendorf and Kiely, 1992; Getahun et al.,
2004).
None of the above mention studies analyzes a long time series of SIDS deaths in the United
States in an attempt to explain trends over time in the syndrome and the factors associated with
changes in the trends. The paper attempts to ll this void in the literature, and does so while
avoiding the problems of the endogeneity of smoking behaviors. To my knowledge, this is the
rst paper that associates long-termtrends in smoking and the exogenous determinants of smoking
to population based SIDS rates in the United States.
3. Cigarette prices and smoking
Research in economics has well established the negative relationship between the price of
cigarettes and the quantity demanded. Price elasticity estimates of cigarette sales data range
from 0.14 to 1.23, with a large number of the estimates falling in a narrower range of
0.20 to 0.50 (USDHHS, 1994). Estimates from individual-level data yield similar estimates,
with a consensus price elasticity of demand for adult smoking of 0.4 (Chaloupka and Warner,
2000).
In addition to estimating own-price effects, several econometric studies have examined the
effects of smoke free air laws on adult smoking behavior. A majority of these studies nd an
inverse relationship between the implementation of these laws and smoking (Wasserman et al.,
1991; Chaloupka, 1992; Evans et al., 1999; Ohsfeldt et al., 1999; Czart et al., 2001; Gallet, 2004).
Tauras (2006) nds that more restrictive smoke free air laws decreases average quantities for adult
smokers, but have no effects on the prevalence of smoking.
The smoking behaviors of pregnant women are also susceptible to changes in cigarette prices.
Using national natality les, Evans and Ringel (1999) and Ringel and Evans (2001) examine the
demand for cigarettes among pregnant women and nd that higher cigarette taxes are associated
with a reduced probability of smoking during pregnancy. They estimate participation price elas-
ticities of 0.5 and 0.7, respectively. Lien and Evans (2005) conrm these participation results
using recent natality data from four states that experienced large cigarette tax changes. Gruber
and Koszegi (2001) also use natality data and nd negative price effects on the average quantity
of cigarettes smoked daily by pregnant women.
Bradford (2003) uses data from the National Maternal and Infant Survey and follow-up to
examine the relationships between cigarette prices and smoking behaviors for pregnant and non-
pregnant women. He nds that while higher prices are negatively associated with the probability
110 S. Markowitz / Journal of Health Economics 27 (2008) 106133
of smoking and the quantity of cigarettes smoked, there is no different in the magnitudes of the
effects for pregnant and non-pregnant women. Colman et al. (2003) show that higher cigarette
taxes are negatively related to the probabilities of smoking before, during and after pregnancy.
This study also examines quit and relapse behavior of pregnant women and nds that higher
taxes are associated with increased probabilities of quitting prior to pregnancy and quitting before
delivery. Higher taxes also decrease the probability that a woman will resume smoking after
delivery.
4. Methods and data
The empirical specication is based on the notion that smoking may lead to SIDS. Therefore,
the exogenous determinants of cigarette consumption, for example cigarette prices andregulations,
are hypothesized to reduce SIDS cases through decreased consumption. The model is specied
as follows:
S
jt
= f(P
jt
, X
jt
, r
t
, q
t
, a
j
). (1)
Eq. (1) shows that the number of SIDS cases (S) in a state (j) for a given year and quarter (t) is a
function of the full price of cigarettes (P
jt
), which includes monetary prices and laws regulating
smoking, other determinants of SIDS (X
jt
), year effects (r
t
), seasonal effects (q
t
), and state effects
(a
j
). The principal hypothesis tested is whether or not changes in the full price of cigarettes can
explain the changes in the number of SIDS cases over time.
Eq. (1) represents a reduced form equation which models SIDS as a direct function of the
full price of cigarettes rather than as a function of consumption of cigarettes. The reduced form
model has two advantages. The rst is that the results will suggest viable policy tools, such as
increases in cigarette taxes, that may be effective in reducing SIDS. The second is that the results
can provide evidence for or against the causal relationship between smoking and SIDS. The
exogenous determinants of consumption, such as prices, are not expected to affect SIDS except
through consumption; thus any result showing that higher prices reduce SIDS is consistent with a
causal explanation. The reduced form is a useful strategy for detecting causality when estimates
of the structural relationship are biased due to correlation of smoking behaviors and unobserved
factors in the error term.
The variables used in Eq. (1) are described in detail below. The unit of observation is at
the state level, and data for each state is observed quarterly for the years 19732003. Quar-
terly data are used so that the variables representing the full price of smoking (prices, taxes,
and smoke free air laws) are matched fairly closely to the actual date of death. However,
as discussed above, the harm from smoking may occur both from prenatal maternal smoking
and from postnatal environmental smoke. These two sources of smoke imply that the cigarette
prices, taxes, and regulations that existed in both time periods are relevant for this study. There-
fore, a second model is considered that includes a 1 year lag of the cigarette policy variables.
A lag of 1 year is chosen since the majority of SIDS cases occur in the second and third
month of life (AAP Task Force on SIDS 2005). The lagged variables will therefore represent
the policies that existed at or near the beginning of the pregnancy for many of the cases of
SIDS. This timing is appropriate as most women make their smoking decisions at the begin-
ning of their pregnancy (Evans and Ringel, 1999). Lagged and current values of prices and
laws are not included in the same models because of the high degree of collinearity across
time.
S. Markowitz / Journal of Health Economics 27 (2008) 106133 111
Given that SIDS cases are counts, I use Fixed Effects Poisson (FEP) to estimate the models
(Wooldridge, 2002; Cameron and Trivedi, 1998). This estimator is a quasi-maximum likelihood
estimator that includes parameters or xed effects to account for unobserved heterogeneity
across the units of observation (states). Estimates are consistent regardless of whether the counts
actually have a Poisson distribution (Wooldridge, 2002). To permit overdispersion, a common
feature of count data that is not accommodated by the Poisson maximum likelihood estimator,
standard errors are adjusted for heteroskedasticity of unknown form that includes a within-state
cluster correlation (Cameron and Trivedi, 2005; Bertrand et al., 2004). Each model includes
the log of the number of live births in the state for each year and quarter as a right hand
side variable to normalize for exposure. The coefcient on log births is constrained to equal
one.
1
4.1. SIDS data
Data on SIDS cases come from the 19732003 Multiple Cause of Death Files provided by
the National Center for Health Statistics (NCHS). SIDS cases rst appear in 1973 because there
was no specic ICD code for SIDS prior to then (Malloy and MacDorman, 2005). In the early
years of the data, ICD-8 code 795.0 identies SIDS cases. From 1979 to 1998, ICD-9 code
798.0 identies the cases. Data from 1999 on uses the ICD-10 code of R95 to identify SIDS
cases.
Differences in reporting practices across time and states may inuence the quarterly SIDS
counts. For example, in 1996, the CDC issued a new reporting form for SIDS along with new
guidelines regarding the death scene investigation (CDC, 1996). This change was implemented
because prior practices for case investigation varied greatly among reporting jurisdictions. Recent
changes in the ICDcodes and coding practices may also be responsible for altering the numbers of
reported cases. In 1999, a variable signifying pending investigation was added to the mortality
les. This change allows certiers to list a tentative cause of death along with the pending inves-
tigation designation. Updates to these cases in the natality les are not always received and many
cases remain without a cause of death listed (Malloy and MacDorman, 2005; Shapiro-Mendoza
et al., 2006). There was also a change in the classication rules for SIDS that occurred when
switching from the ICD-9 to ICD-10 that may have resulted in a shift in case classications away
fromSIDS, towards other unknown/unspecied causes and accidental suffocation or strangulation
in bed (Shapiro-Mendoza et al., 2006).
While the reporting issues may affect the observed trends in SIDS, these factors should not
inuence the conclusions regarding smoking policies in the multivariate analysis. First, changes
in the reporting that is uniform to all states at one time can be accounted for by dichotomous
indicators for years in the models. Second, so long as the measurement error in the dependent
variable is uncorrelated with the explanatory variables of interest, this will raise the standard
errors on the coefcients but still produce consistent estimates. The estimated coefcients could
be affected if the changes in the reporting practices were systematically related to changes in
cigarette prices and policies, however, this possibility seems highly unlikely.
1
Results of alternative estimation techniques are shown in Appendix Table A1. The top panel shows results using a
log-linear model of SIDS rates instead of counts. The bottompanel shows results using Negative Binomial regression with
xed effects. Results are very similar to those presented in the main tables. Note that the FEP models are preferred because
the FEP estimates are consistent under much weaker distributional assumptions than the Negative Binomial estimates.
112 S. Markowitz / Journal of Health Economics 27 (2008) 106133
4.2. Cigarette variables
Cigarette prices and taxes are used as alternative measures of the monetary price of cigarettes.
Cigarette price and tax data come from the annual Tax Burden on Tobacco (Orzechowski and
Walker, 2005). The prices are weighted averages for a pack of 20 cigarettes and are inclu-
sive of state excise taxes. Because the price published is as of November 1 of each year,
the prices were adjusted to create a state-level average quarterly price. Quarterly taxes are
determined using the effective date of legislated tax changes. Cigarette prices and taxes are
deated by the national Consumer Price Index published by the Bureau of Labor Statistics
(19821984 =100).
A number of variables representing the degree of smoking restrictions in certain places are
included as additional measures of the full price of cigarettes. I use smoke free air (SFA) laws per-
taining to private workplaces, restaurants, and child care centers. These variables were obtained
from Gary Giovino at the Roswell Park Cancer Institute who created these variables for project
ImpacTeen (http://www.impacteen.org/tobaccodata.htm).
2
The laws are appended to the SIDS
data by state, year, and quarter, based on the effective dates of the laws. Even though states
have SFA laws regarding many different establishments, these three are the focus of this paper
because private workplace and restaurant restrictions are very common and research has show
there to be an inuence of these individual laws on smoking behaviors (Evans et al., 1999;
Tauras, 2004). Restrictions in child care facilities are included because of the relevance to
SIDS.
The laws for private workplaces and restaurants are grouped in four categories: (1) no provi-
sions; (2) laws that restrict smoking to designated areas or areas with separate ventilation with
exemptions for the size of the establishment; (3) laws that restrict smoking to areas with separate
ventilation or imposes a ban, with exemptions; and (4) smoking bans that are present at all times.
I create dichotomous indicators for each category and site (workplaces and restaurants) to include
in the regressions. The category of no provisions serves as the omitted reference group. In the
tables, the variable SFA-1 refers to the laws designating smoking areas (category 2 above), SFA-2
refers to the laws with separate ventilation requirements (category 3 above), and SFA-3 refers to
the full ban (category 4 above).
The laws for child care facilities are grouped in six categories: (1) no provisions; (2) laws
that restrict smoking to designated areas; (3) laws that restrict smoking to areas with separate
ventilation or imposes a ban when children are present, with exemptions; (4) a ban when children
are present for commercial day care sites; (5) a ban when children are present for commercial
and home-based day care sites; and (6) a ban at all times for all types of day care arrangements.
Again, dichotomous indicators are created for these groups with the category of no provisions
serving as the omitted reference group. The variables SFA-1 through SFA-5 referring to laws in
categories 2 through 6, respectively.
Because of the high degree of collinearity between the regulations, each group of SFA laws
is included separately in the regressions according to the site. The collinearity arises because
many states pass SFA laws applicable to different facilities at the same time. If these laws are
considered as simple indexes (i.e. one variable with values 1 through 4 or 1 through 6), the
simple correlations between restrictions in private workplaces and restaurants is 0.66, between
2
Information on SFA laws with effective dates prior to 1991 was obtained by consulting the National Cancer Institutes
State Cancer Legislative Database and state statutes.
S. Markowitz / Journal of Health Economics 27 (2008) 106133 113
private workplaces and child care centers is 0.40, and between restaurants and child care centers
is 0.46.
An alternative model is also presented in the tables. Termed smoking ban count, a new
variable is created to count the number of bans present in the state in all three sites. That is, this
variable counts the number of times a full ban appears for the private workplace, restaurant, and
child care centers within given state, year and quarter. The top three categories for child care
centers are considered to be full bans here. For example, if none of the locations has a ban in
effect then the smoking ban measure takes on a value of zero. If all three locations have a ban,
then the measure takes on a value of three. In addition to showing the effects of having strict bans
on the SIDS counts, this variable may also help account for some of the unobserved sentiment
towards smoking in the state since states with the most comprehensive SFA laws will have higher
values for this count.
4.3. Temporal and state variables
As mentioned above, the Back to Sleep campaign has been widely cited as the primary
cause for the recent reductions in SIDS cases. In 1992, the American Academy of Pediatrics
recommended a side or back sleeping position as a way to reduce SIDS. The national Back to
Sleep campaign began in 1994 and continues today. In 1996, the AAP advised that the back is
the preferred sleep position, as new evidence revealed an increased risk of SIDS for side-sleepers
relative to back-sleepers (AAP, 2005). It is difcult to know the rate at which the dissemination
of information regarding sleep position reached individuals in different states. Therefore, annual
time dummies will be used to represent the effects of the campaign. Quarterly time indicators are
also included to represent seasonal changes in SIDS rates. Models were also tested that include
indicators for each unique year and quarter, and the results do not change. These results are
available upon request. The model with separate year and quarter indicators is preferred since the
effects of the post-1992 AAP recommendations can be clearly seen with annual time dummies.
Also, within each year there is a strong seasonal trend to SIDS with more deaths occurring in the
rst and fourth quarters of the year.
Each model includes some other state-level time varying variables to account for additional
factors which may be associated with the number of SIDS cases over time. Maternal characteris-
tics, such as low income, low education, and young maternal age are all strongly correlated with
an increased the risk of SIDS (Anderson and Cook, 1997; Spencer and Logan, 2004; Hunt and
Hauck, 2006). To represent SES status, I include the annual state unemployment rate, the annual
real per capita income, and the quarterly average level of education of new mothers in all models.
Education is represented as the percentage of mothers giving birth in each state and quarter who
have less than a high school education (the omitted reference category), a high school education,
some college, or a college degree or higher.
3
The quarterly average age of rst-time mothers is
also included. It should be noted that the low SES is not believed to be a causal factor of SIDS,
but rather a distal factor that acts through some of the other known risk factors, such as low
birth weight, smoking, or prone sleeping. Unemployment rates and per capita income come from
Department of Labor, Bureau of Labor Statistics and the Department of Commerce, Bureau of
3
Ten states have missing values for education in various years of the data prior to 1992. These observations represents
5 percent of the sample. To preserve the observations, the sample means replace the missing values. Models were also
tested that exclude the education variables and results for the cigarette policies remain unchanged.
114 S. Markowitz / Journal of Health Economics 27 (2008) 106133
Economic Analysis, respectively. The average age of the mother at rst live birth and the average
education of new mothers are generated from the National Center for Health Statistics Natality
les, 19732003.
Infant characteristics, such as male gender, non-white race, and low birth weight are also
associated with a higher risk of SIDS (Anderson and Cook, 1997; Pickett et al., 2005; Getahun
et al., 2004). State-level rates of new births representing these characteristics are included in the
models.
4
The percentages of births that are male, low birth weight (less than 2500 g but greater
than 1500 g), and very low birth weight (less than 1500 g) are generated from the NCHS Natality
les for each state and quarter. Note that the low birth weight variables may be problematic in
the models since birth weight is also an outcome of prenatal smoking. This issues is examined
in further detail below. The percentages of births born to mothers who are identied as black
and Native Americans are also included in all models. Lastly, all models also include state xed
effects to account for unmeasured, time invariant characteristics unique to each state.
In the models below, low birth weight, gender and the seasonal indicators may also capture
some of the suspected biological based causes of SIDS discussed in the introduction. For example,
the study by Paterson et al. (2006) provides neurochemical evidence as to why the prevalence of
SIDS is higher in boys. To the extent that respiratory infections peak in the winter months, the
indicators for the quarter of the year will capture this trend.
5. Results
Fig. 1 shows rates of SIDS cases over time plotted along with average cigarette prices in the
United States. Even this crude picture clearly shows a strong negative relationship between the
two variables. SIDS cases per 1000 live births increase fromthe initial year of 1973 until 1980 and
thereafter fall almost continuously until 2003. There are two slight increases in 1983 and 2002.
By contrast, real cigarette prices decrease until 1981, after which they rise almost continuously,
with a brief decline between 1992 and 1994.
Table 1 shows means and standard deviations for all included variables. Columns 1 and 2
shows the statistics for the entire period, while columns 23 and 45 show the statistics for the
beginning and ending periods, 1973 and 2003, respectively. Over this 31 year period, there are an
average of 21 cases of SIDS every quarter. The real average price of a pack of cigarettes is $1.15,
while the real average state excise tax on a pack is $0.20. Smoke free air laws are somewhat lax
over the full period with no restrictions in any state in 1973 to a majority of states having some
kind of restriction in 2003.
5.1. Cigarette sales and smoking during pregnancy
To demonstrate the positive correlation between smoking and SIDS, I rst estimate a structural
model where the SIDS count is regressed on measures of cigarette smoking and the other state-
4
Better estimates of the relationships between the maternal and infant characteristics and SIDS can be obtained by
using individual-level data such as the linked birthdeath records from the National Center for Health Statistics. I chose
not to use individual level data because the cigarette variables are reported at the state level, and there is no gain to
using individual-level data for the estimation of these coefcients. Also, the linked birth and death data are currently only
available from 1983 to 1991 and 1995 to 2001 providing far fewer years of data than the Multiple Cause of Death Files.
Some of these years do not include information on the death month which would prevent the merge of cigarette variables
by quarter and result in a less precise match of the cigarette policies with the date of death.
S. Markowitz / Journal of Health Economics 27 (2008) 106133 115
Table 1
Means and standard deviations
All years (n =6324) First year: 1973
(n =204)
Last year: 2003
(n =204)
Mean Standard
deviation
Mean Standard
deviation
Mean Standard
deviation
SIDS count 20.96 24.74 16.00 16.55 10.60 10.76
Real cigarette price 1.15 0.39 0.92 0.11 2.06 0.32
Real cigarette tax 0.20 0.12 0.26 0.10 0.37 0.26
SFA-1: private workplace 0.22 0.00 0.35
SFA-2: private workplace 0.01 0.00 0.05
SFA-3: private workplace 0.01 0.00 0.08
SFA-1: restaurant 0.32 0.00 0.49
SFA-2: restaurant 0.01 0.00 0.02
SFA-3: restaurant 0.02 0.00 0.10
SFA-1: child care center 0.07 0.00 0.15
SFA-2: child care center 0.01 0.00 0.04
SFA-3: child care center 0.07 0.00 0.19
SFA-4: child care center 0.08 0.00 0.28
SFA-5: child care center 0.01 0.00 0.04
Smoking ban count 0.18 0.44 0.00 0.00 0.69 0.78
Maternal age at rst birth 23.54 1.44 21.42 0.70 25.00 1.28
High school degree 0.39 0.06 0.44 0.05 0.30 0.07
Some college 0.21 0.05 0.17 0.05 0.22 0.06
College or more 0.19 0.07 0.12 0.04 0.26 0.09
Black 0.14 0.15 0.13 0.15 0.13 0.14
Native American 0.02 0.04 0.02 0.04 0.02 0.05
Other race 0.03 0.09 0.02 0.09 0.05 0.09
Female baby 0.49 0.01 0.49 0.01 0.49 0.01
Low birth weight 0.06 0.01 0.06 0.01 0.07 0.01
Very low birth weight 0.01 0.00 0.01 0.00 0.01 0.00
State unemployment 6.05 2.07 4.83 1.45 5.65 1.04
State real income per capita (in $1000s) 13.75 2.78 11.46 1.70 16.71 2.64
State per capita cigarette sales (in packs) 109.86 33.98 132.32 35.15 75.29 31.02
Maternal smoking during pregnancy 0.16 0.05 0.13 0.05
Note: The unit of observation is a state in each year and quarter of the data. See text for denitions of the levels of smoke
free air (SFA) restrictions. Higher levels indicate more stringent restrictions.
level variables described above. Estimates of the structural model are not the main focus of
this paper because the reduced form, not the structural model, is directly applicable to policy, and
because the aggregate cigarette consumption data I use are not the best for estimating the structural
equation. For example, individual-level smoking behavior from the linked birthdeath les from
the National Center for Health Statistics could be used to examine the direct effect of maternal
prenatal smoking on the probability of a child dying of SIDS. These data, however, are available
for far fewer years than the Multiple Cause of Death Files I use and have other disadvantages for
the reduced form estimation.
The literature linking smoking and SIDS discussed above cites smoking as a causal factor for
SIDS, nevertheless, in a structural model, the coefcient on smoking can be biased if smoking
behaviors are correlated with other unobserved or unmeasured factors that also inuence the
occurrence of SIDS. To address this, models that account for the potential endogeneity of smoking
116 S. Markowitz / Journal of Health Economics 27 (2008) 106133
are also presented using the approach described by Wooldridge (2002) for count models with
endogenous right hand side variables. This is a two-step procedure that rst runs a rst stage
model via OLS. Here, the cigarette price and all dichotomous indicators of the smoke free air
laws are used as instruments for the measures of smoking. The residuals from the rst stage
regression are then predicted and included as an additional covariate in the second stage structural
model, which is estimated by Poisson regression. Standard errors are adjusted to be panel-robust
(correlated among states). The resulting estimates are consistent. F-tests of the instruments are
presented, and the endogeneity of the consumption measures are tested by examining the t-statistic
on the rst stage residuals in the second equation.
Two measures of smoking are considered. The rst is the per capita number of packs of
cigarettes sold annually in each state as of June 30, and the second is the percentage of women in
each quarter who gave birth and reported smoking during pregnancy. These measures are chosen
to represent postnatal and prenatal smoking, the two ways smoking can affect child health. In the
absence of data on childrens direct exposure to environmental smoke, sales data provide a crude
representation of the possible presence of secondhand smoke.
The sales data come from the Tax Burden on Tobacco (Orzechowski and Walker, 2005). Since
these data are as of June 30 of each year, a given years sales data is matched to the SIDS counts
for the rst and second quarter of the same year and the third and fourth quarter of the previous
year. These results are in the rst and second columns of Table 2. However, since there is no
quarterly variation in the sales data, an alternative specication is shown in columns 3 and 4 of
Table 2 in which the quarterly SIDS data have been aggregated to annual data. In these models,
the dependent variable is the total SIDS counts for the rst and second quarter of the current year
and the third and forth quarter of the previous year. The other right hand side variables are all
averages over the relevant quarters.
Rates of smoking during pregnancy based on the mothers state of residency are calculated
from the NCHS Natality les for each state and quarter beginning in 1989, the rst year that
questions were asked on tobacco used during pregnancy.
5
Any live birth in a given quarter is at
risk for SIDS, so estimates of the structural model using this smoking measure will tell the effects
of higher proportions of women giving birth who smoked during pregnancy on the current SIDS
counts.
Table 2 shows the results of the structural models. Consumption is treated as exogenous in odd
numbered columns and as endogenous in the even numbered columns. Columns 1 through 4 show
that the coefcients on per capita sales are positive and statistically signicant. The coefcients
and marginal effects are much larger when smoking is treated as endogenous. For example, the
results in column 3 and 4 show that an increase in one pack of per capita cigarettes sold is
associated with 0.21 and 0.48 more annual SIDS deaths, respectively.
6
Note that an increase in
sales of one pack represents about one percent of the average total sales per capita. In columns
2 and 4, the F-tests indicate that the instruments are valid, and the hypothesis of exogeneity
of smoking can be rejected. The results of the structural model using aggregate sales provides
evidence that smoking behaviors are likely to correlated with unobserved factors in a structural
model of SIDS, and even after taking this into account, environmental smoke is an important
contributor to SIDS.
5
Information on tobacco use is not collected on the birth certicates in California, Indiana, NewYork, and South Dakota
in various years. These states are omitted from the sample in the relevant years.
6
The estimates of the structural models may be overstated if sales underreports actual consumption due to smuggling
or internet sales of cigarettes.
S
.
M
a
r
k
o
w
i
t
z
/
J
o
u
r
n
a
l
o
f
H
e
a
l
t
h
E
c
o
n
o
m
i
c
s
2
7
(
2
0
0
8
)
1
0
6
1
3
3
1
1
7
Table 2
SIDS counts on cigarette sales and smoking during pregnancy
Cigarette consumption Exogenous (1) Endogenous (2) Exogenous (3) Endogenous (4) Exogenous (5) Endogenous (6)
Annual per capita cigarette
sales
0.005 (4.46) [0.069] 0.012 (3.67) [0.148] 0.004 (3.94) [0.212] 0.010 (3.20) [0.477]
Smoking during pregnancy 2.534 (2.79) [25.105] 0.151 (0.03) [1.499]
Maternal age at rst birth 0.103 (1.72) 0.029 (0.44) 0.101 (1.86) 0.013 (0.18) 0.130 (1.95) 0.089 (0.91)
High school degree 0.093 (0.26) 0.197 (0.53) 0.209 (0.59) 0.270 (0.72) 0.598 (0.90) 0.512 (0.78)
Some college 0.204 (0.20) 0.241 (0.23) 0.139 (0.13) 0.217 (0.20) 2.632 (1.85) 3.195 (1.74)
College or more 0.919 (1.06) 0.978 (1.20) 0.377 (0.37) 0.419 (0.42) 0.002 (0.00) 0.213 (0.19)
Black 0.285 (0.28) 0.074 (0.07) 0.750 (0.56) 0.400 (0.29) 0.606 (0.41) 0.547 (0.37)
Native American 4.298 (1.58) 3.746 (1.48) 6.128 (2.19) 5.619 (2.25) 9.574 (2.87) 9.922 (2.80)
Other race 4.444 (3.57) 4.522 (4.28) 4.998 (3.85) 5.158 (4.30) 4.917 (1.73) 5.717 (1.81)
Female baby 0.129 (0.14) 0.231 (0.25) 2.542 (0.96) 2.529 (0.95) 1.064 (0.78) 1.096 (0.81)
Low birth weight 0.123 (0.05) 3.018 (1.06) 8.427 (1.66) 3.644 (0.65) 0.992 (0.38) 0.007 (0.002)
Very low birth weight 3.345 (0.71) 1.041 (0.24) 16.394 (1.36) 14.016 (1.21) 4.806 (0.77) 6.246 (0.86)
State unemployment 0.001 (0.12) 0.009 (1.14) 0.004 (0.49) 0.015 (1.59) 0.017 (1.45) 0.016 (1.30)
State real income per capita 0.051 (1.76) 0.060 (2.26) 0.030 (0.87) 0.040 (1.22) 0.009 (0.33) 0.012 (0.43)
First stage residuals (t-test is
a test for exogeneity)
0.008 (2.59) 0.007 (2.28) 2.749 (0.58)
F-test on instruments
[p-value]
25.510 [0.000] 17.380 [0.000] 5.970 [0.000]
N 6324 6324 1632 1632 2872 2872
Note: t-statistics in parentheses, and intercept not shown. Columns 1, 3 and 5 are estimated using the Fixed Effects Poisson and assume cigarette consumption is exogenous. Columns 2, 4 and 6 are
estimated using a two-step procedure for exponential regression models as described by Wooldridge (2002) and assume cigarette consumption is endogenous. Instruments include the real cigarette price
and the eleven indicator variables for the different smoke free air laws. Italic brackets show marginal effects; the change in the average quarterly SIDS count from a one unit change in the independent
variable. Coefcients on continuous variables can be interpreted as the percentage change in the average quarterly SIDS count from a one unit change in the independent variable. Columns 1 and 2
use quarterly data from 1973 to 2003, columns 3 and 4 use annual data from 1973 to 2003, and columns 5 and 6 uses quarterly data from 1989 to 2003. All models also include year and state dummy
variables. Columns 1, 2, 5 and 6 also include quarterly dummies.
118 S. Markowitz / Journal of Health Economics 27 (2008) 106133
The coefcient in column 5 on the percentage of women giving birth who smoked during
pregnancy is also positive and statistically signicant. This result disappears once smoking is
treated as endogenous, however, it is not clear how much faith can be placed in this estimate
as the F-statistic on the instruments is low, although signicant, and the exogeneity of maternal
smoking cannot be rejected. The marginal effect in column 5 shows that every one percentage
point increase in the proportion of mothers who smoked during pregnancy is associated with an
average increase in 25.1 SIDS deaths. The magnitude of this effect is quite large considering
a quarterly average SIDS death count of 15.77 per state from the period 19891993. However,
the total number of babies born during this period is also very large (about 60 million). To put
these numbers into context, in 2003 the average rate of maternal smoking across all states was
12.5%. An additional percentage point increase in this smoking translates to an additional 40,900
babies born to mothers who smoke during that year. Twenty-ve more SIDS deaths represents
0.06 percent of the 40,900 births.
5.2. Cigarette policy results
Estimates of the reduced form models are presented in Tables 35 . Table 3 includes the price
of cigarettes, while Table 4 includes instead the state excise tax on cigarettes. Table 5 presents
results from models that include the lagged values of the cigarette variables. Five models are
presented in each table. The rst includes the monetary price measure along with the state-level
maternal and infant characteristics, the unemployment rate and real income per capita, state xed
effects, year xed effects, and quarter xed effects. For brevity, the coefcients on state xed
effects are not shown in Table 3, and the coefcients on all xed effects are not shown in the
subsequent tables. The alternative specications in each table build on the rst model and include
separately in columns 25 the three sets of dichotomous indicators for the smoke free air laws
and the smoking ban count.
Since price and tax are continuous measures, these coefcients from the Poisson regression
can be directly interpreted as semi-elasticities, that is, the percentage change in SIDS cases from
a one unit change in the independent variable. I also present an alternative marginal effect in
brackets which shows the absolute change in the number of SIDS cases from a one dollar change
in the price variable. Elasticity estimates are presented for cigarette prices and taxes at the bottom
of each table. To get a semi-elasticity for the dichotomous indicators, a transformation of the
coefcients (exp(B)-1) is necessary (not shown). For ease of interpretation, I also present the
marginal effect in brackets which show the absolute change in the number of SIDS cases from
the dummy variable taking on a value of 1.
The rst row in Table 3 shows the coefcients, t-statistics and marginal effects for the real
price of cigarettes. The results show across all models that higher cigarette prices are associated
with a reduction in SIDS deaths. A $1 increase in the price of cigarettes is associated with an
average reduction of 7.68.3 SIDS deaths. In elasticity terms, a ten percent increase in the real
price of cigarettes reduces SIDS deaths by a range of 6.97.6 percent.
7
7
The presence of alternative sources of lower priced cigarettes (internet sales, sales from Indian reservations or smug-
gling) may lower the actual average price paid in the states, resulting in an overstatement of the observed price of cigarettes.
In the reduced form, the SIDS counts reects actual consumption, not reported sales, so reporting bias on the consumption
side not a factor here. For a given change in the SIDS counts, the change in average prices in the presence of smuggling is
overestimated, so the reduced form effects of prices are underestimated and the results represent lower bound estimates.
S
.
M
a
r
k
o
w
i
t
z
/
J
o
u
r
n
a
l
o
f
H
e
a
l
t
h
E
c
o
n
o
m
i
c
s
2
7
(
2
0
0
8
)
1
0
6
1
3
3
1
1
9
Table 3
SIDS counts on cigarette prices and smoke free air laws
(1) (2) (3) (4) (5)
Real cigarette price 0.659 (4.24) [8.343] 0.642 (4.56) [8.137] 0.620 (4.80) [7.851] 0.605 (4.10) [7.662] 0.598 (4.42) [7.583]
SFA-1: private workplace 0.056 (1.19) [0.694]
SFA-2: private workplace 0.323 (5.72) [3.512]
SFA-3: private workplace 0.171 (1.26) [2.364]
SFA-1: restaurant 0.070 (1.85) [0.872]
SFA-2: restaurant 0.271 (4.65) [3.934]
SFA-3: restaurant 0.390 (4.45) [4.123]
SFA-1: child care center 0.059 (0.90) [0.731]
SFA-2: child care center 0.130 (2.31) [1.750]
SFA-3: child care center 0.091 (1.24) [1.108]
SFA-4: child care center 0.138 (2.07) [1.657]
SFA-5: child care center 0.099 (1.58) [1.191]
Smoking ban count 0.119 (3.02) [1.510]
Maternal age at rst birth 0.121 (1.88) 0.090 (1.50) 0.091 (1.59) 0.102 (1.74) 0.102 (1.86)
High school degree 0.448 (1.13) 0.447 (1.05) 0.382 (0.97) 0.384 (1.04) 0.372 (1.03)
Some college 0.481 (0.50) 0.546 (0.60) 0.404 (0.47) 0.356 (0.40) 0.206 (0.23)
College or more 0.596 (0.74) 0.306 (0.40) 0.445 (0.62) 0.739 (1.05) 0.793 (1.13)
Black 1.159 (1.33) 0.983 (1.10) 0.969 (1.08) 1.222 (1.43) 1.289 (1.53)
Native American 4.663 (1.78) 4.236 (1.53) 4.146 (1.44) 5.178 (1.93) 4.638 (1.55)
Other race 4.269 (4.38) 3.373 (3.65) 3.282 (3.66) 3.976 (4.19) 3.732 (3.98)
Female baby 0.052 (0.06) 0.079 (0.09) 0.074 (0.08) 0.067 (0.07) 0.034 (0.04)
Low birth weight 0.811 (0.31) 0.309 (0.13) 0.537 (0.23) 0.197 (0.08) 0.115 (0.05)
Very low birth weight 1.669 (0.37) 0.721 (0.16) 0.104 (0.02) 1.893 (0.42) 2.002 (0.44)
State unemployment 0.005 (0.64) 0.005 (0.68) 0.006 (0.91) 0.006 (0.70) 0.006 (0.76)
State real income per capita 0.045 (1.58) 0.057 (2.16) 0.068 (2.66) 0.052 (2.05) 0.059 (2.48)
1974 0.129 (2.49) 0.121 (2.50) 0.120 (2.54) 0.127 (2.51) 0.126 (2.56)
1975 0.244 (3.36) 0.231 (3.36) 0.234 (3.47) 0.241 (3.33) 0.239 (3.45)
1976 0.311 (5.15) 0.296 (5.12) 0.302 (5.53) 0.306 (5.08) 0.306 (5.36)
1977 0.389 (5.41) 0.372 (5.55) 0.380 (5.93) 0.380 (5.45) 0.382 (5.79)
1978 0.468 (6.20) 0.447 (6.35) 0.463 (6.84) 0.459 (6.40) 0.464 (6.75)
1979 0.474 (5.27) 0.447 (5.45) 0.463 (5.90) 0.461 (5.36) 0.464 (5.77)
1980 0.455 (4.72) 0.419 (4.72) 0.436 (5.25) 0.440 (4.84) 0.442 (5.26)
1981 0.440 (4.11) 0.398 (3.97) 0.416 (4.49) 0.422 (4.26) 0.424 (4.57)
1982 0.482 (4.07) 0.432 (3.99) 0.451 (4.53) 0.458 (4.15) 0.460 (4.50)
1983 0.619 (4.77) 0.566 (4.89) 0.587 (5.50) 0.588 (4.99) 0.591 (5.37)
1
2
0
S
.
M
a
r
k
o
w
i
t
z
/
J
o
u
r
n
a
l
o
f
H
e
a
l
t
h
E
c
o
n
o
m
i
c
s
2
7
(
2
0
0
8
)
1
0
6
1
3
3
Table 3 (Continued)
(1) (2) (3) (4) (5)
1984 0.650 (5.00) 0.599 (5.06) 0.625 (5.63) 0.616 (5.22) 0.623 (5.61)
1985 0.677 (5.05) 0.628 (5.09) 0.656 (5.63) 0.642 (5.21) 0.652 (5.60)
1986 0.725 (5.25) 0.679 (5.26) 0.708 (5.81) 0.688 (5.52) 0.699 (5.82)
1987 0.737 (5.13) 0.690 (5.15) 0.719 (5.61) 0.695 (5.34) 0.708 (5.62)
1988 0.816 (5.24) 0.768 (5.27) 0.802 (5.73) 0.772 (5.46) 0.786 (5.71)
1989 0.856 (5.28) 0.814 (5.43) 0.852 (5.94) 0.817 (5.55) 0.832 (5.83)
1990 0.819 (4.75) 0.778 (4.92) 0.817 (5.36) 0.785 (4.97) 0.799 (5.22)
1991 0.864 (4.91) 0.821 (5.11) 0.859 (5.63) 0.826 (5.13) 0.838 (5.39)
1992 0.830 (4.46) 0.788 (4.50) 0.828 (4.98) 0.791 (4.65) 0.804 (4.85)
1993 0.749 (4.11) 0.709 (4.10) 0.752 (4.51) 0.718 (4.23) 0.731 (4.40)
1994 0.605 (3.22) 0.569 (3.21) 0.613 (3.61) 0.609 (3.33) 0.623 (3.55)
1995 0.458 (2.50) 0.458 (2.63) 0.512 (3.15) 0.464 (2.62) 0.498 (2.92)
1996 0.376 (1.92) 0.376 (2.01) 0.431 (2.47) 0.380 (1.99) 0.417 (2.26)
1997 0.397 (1.86) 0.400 (1.95) 0.458 (2.37) 0.400 (1.91) 0.438 (2.16)
1998 0.417 (2.00) 0.427 (2.13) 0.489 (2.62) 0.418 (2.06) 0.459 (2.34)
1999 0.580 (2.43) 0.581 (2.55) 0.637 (3.04) 0.563 (2.46) 0.602 (2.74)
2000 0.676 (2.51) 0.676 (2.64) 0.730 (3.11) 0.649 (2.54) 0.687 (2.82)
2001 0.611 (2.23) 0.608 (2.33) 0.663 (2.77) 0.579 (2.24) 0.617 (2.48)
2002 0.735 (2.50) 0.733 (2.61) 0.779 (3.05) 0.698 (2.51) 0.734 (2.74)
2003 0.709 (2.36) 0.694 (2.38) 0.764 (2.90) 0.675 (2.34) 0.720 (2.60)
First quarter 0.293 (11.54) 0.294 (11.84) 0.295 (12.15) 0.296 (11.69) 0.295 (11.70)
Second quarter 0.519 (21.28) 0.520 (21.04) 0.518 (20.85) 0.519 (21.40) 0.519 (21.09)
Third quarter 0.029 (1.89) 0.033 (2.00) 0.031 (1.89) 0.031 (1.99) 0.030 (1.85)
Price elasticity 0.757 0.737 0.712 0.695 0.687
Note: t-statistics in parentheses, and intercept not shown. Brackets show marginal effects; the change in the average quarterly SIDS count from a one unit change in the independent variable.
Coefcients on continuous variables can be interpreted as the percentage change in the average quarterly SIDS count from a one unit change in the independent variable. All models also
include state dummy variables. N=6324.
S
.
M
a
r
k
o
w
i
t
z
/
J
o
u
r
n
a
l
o
f
H
e
a
l
t
h
E
c
o
n
o
m
i
c
s
2
7
(
2
0
0
8
)
1
0
6
1
3
3
1
2
1
Table 4
SIDS counts on cigarette tax and smoke free air laws
(1) (2) (3) (4) (5)
Real cigarette tax 0.922 (4.21) [11.664] 0.849 (4.55) [10.763] 0.820 (4.64) [10.381] 0.842 (4.11) [10.665] 0.811 (4.36) [10.277]
SFA-1: private workplace 0.049 (1.04) [0.611]
SFA-2: private workplace 0.276 (4.87) [3.061]
SFA-3: private workplace 0.179 (1.26) [2.483]
SFA-1: restaurant 0.064 (1.74) [0.801]
SFA-2: restaurant 0.292 (4.82) [4.290]
SFA-3: restaurant 0.353 (3.79) [3.793]
SFA-1: child care center 0.070 (1.09) [0.863]
SFA-2: child care center 0.125 (2.19) [1.689]
SFA-3: child care center 0.089 (1.20) [1.082]
SFA-4: child care center 0.121 (1.98) [1.452]
SFA-5: child care center 0.115 (1.80) [1.378]
Smoking ban count 0.106 (2.84) [1.349]
Maternal age at rst birth 0.117 (1.86) 0.094 (1.57) 0.094 (1.62) 0.100 (1.70) 0.102 (1.82)
High school degree 0.518 (1.29) 0.493 (1.14) 0.430 (1.07) 0.429 (1.16) 0.426 (1.16)
Some college 0.440 (0.47) 0.536 (0.59) 0.422 (0.49) 0.355 (0.40) 0.210 (0.23)
College or more 0.648 (0.83) 0.391 (0.51) 0.499 (0.69) 0.763 (1.09) 0.823 (1.18)
Black 1.116 (1.28) 0.927 (1.05) 0.899 (1.02) 1.166 (1.35) 1.230 (1.45)
Native American 3.911 (1.43) 3.661 (1.27) 3.596 (1.19) 4.554 (1.64) 4.018 (1.30)
Other race 4.288 (4.30) 3.622 (3.76) 3.479 (3.79) 4.071 (4.18) 3.875 (4.03)
Female baby 0.068 (0.07) 0.091 (0.10) 0.086 (0.09) 0.079 (0.08) 0.049 (0.05)
Low birth weight 0.908 (0.36) 0.058 (0.02) 0.223 (0.09) 0.393 (0.16) 0.142 (0.06)
Very low birth weight 1.591 (0.36) 0.875 (0.20) 0.227 (0.05) 1.853 (0.42) 1.981 (0.44)
State unemployment 0.008 (0.90) 0.007 (0.94) 0.008 (1.15) 0.008 (0.90) 0.008 (0.99)
State real income per
capita
0.053 (1.92) 0.062 (2.30) 0.072 (2.77) 0.057 (2.27) 0.064 (2.63)
Tax elasticity 0.184 0.169 0.163 0.168 0.162
Note: t-statistics in parentheses, and intercept not shown. Brackets show marginal effects; the change in the average quarterly SIDS count from a one unit change in the independent variable.
Coefcients on continuous variables can be interpreted as the percentage change in the average quarterly SIDS count from a one unit change in the independent variable. All models also
include year, quarter, and state dummy variables. N=6324.
1
2
2
S
.
M
a
r
k
o
w
i
t
z
/
J
o
u
r
n
a
l
o
f
H
e
a
l
t
h
E
c
o
n
o
m
i
c
s
2
7
(
2
0
0
8
)
1
0
6
1
3
3
Table 5
SIDS counts on lagged cigarette price, tax and smoke free air laws
(1) (2) (3) (4) (5)
Panel A
Lagged cigarette price 0.752 (4.38) [0.837] 0.733 (5.00) [9.287] 0.696 (4.72) [8.825] 0.689 (4.36) [8.730] 0.682 (4.50) [8.649]
Lagged SFA-1: private workplace 0.056 (1.15) [0.697]
Lagged SFA-2: private workplace 0.308 (5.07) [3.363]
Lagged SFA-3: private workplace 0.285 (4.79) [4.179]
Lagged SFA-1: restaurant 0.068 (1.74) [0.846]
Lagged SFA-2: restaurant 0.252 (4.09) [3.632]
Lagged SFA-3: restaurant 0.377 (3.75) [3.998]
Lagged SFA-1: child care center 0.061 (0.94) [0.757]
Lagged SFA-2: child care center 0.131 (1.91) [1.768]
Lagged SFA-3: child care center 0.103 (1.43) [1.251]
Lagged SFA-4: child care center 0.132 (1.88) [1.578]
Lagged SFA-5: child care center 0.104 (1.74) [1.256]
Lagged Smoking ban count 0.118 (2.93) [1.494]
Price elasticity 0.837 0.815 0.775 0.767 0.759
Panel B
Lagged cigarette tax 1.029 (4.28) [13.030] 0.969 (4.74) [12.278] 0.914 (4.38) [11.588] 0.946 (4.22) [11.986] 0.912 (4.27) [11.566]
Lagged SFA-1: private workplace 0.050 (1.02) [0.623]
Lagged SFA-2: private workplace 0.257 (4.08) [2.877]
Lagged SFA-3: private workplace 0.308 (4.83) [4.564]
Lagged SFA-1: restaurant 0.062 (1.65) [0.778]
Lagged SFA-2: restaurant 0.275 (4.18) [4.009]
Lagged SFA-3: restaurant 0.334 (3.14) [3.619]
Lagged SFA-1: child care center 0.073 (1.17) [0.897]
Lagged SFA-2: child care center 0.127 (1.83) [1.719]
Lagged SFA-3: child care center 0.102 (1.41) [1.236]
Lagged SFA-4: child care center 0.113 (1.75) [1.360]
Lagged SFA-5: child care center 0.123 (2.01) [1.471]
Lagged Smoking ban count 0.104 (2.69) [1.316]
Tax elasticity 0.202 0.190 0.179 0.185 0.179
Note: t-statistics in parentheses, and intercept not shown. Brackets show marginal effects; the change in the average quarterly SIDS count from a one unit change in the independent variable. All models
also include maternal, infant and state characteristics, and year, quarter, and state dummy variables. N=6324.
S. Markowitz / Journal of Health Economics 27 (2008) 106133 123
The marginal effects are a little difcult to interpret since a one dollar increase represents an
87 percent increase over the mean real price of $1.15. Using the price elasticity from column 5, a
10 percent increase in the average price (11.5 cents) is associated with a reduction in the average
quarterly SIDS count of 6.87 percent. To put this in perspective, in 2003, for example, there were
4.09 million births and 2162 SIDS deaths nationally, for a death rate of 0.53 per 1000 births. In
this year, a 10 percent increase in cigarette prices nationally would reduce the number of deaths
by 148.5 resulting in a death rate of 0.49 deaths per 1000 births.
The coefcients on the smoke free air laws are for the most part negative indicating that smoking
restrictions and bans are associated with decreases in the SIDS counts. For private workplaces,
the intermediate level restrictions (separate ventilation or else a ban) has the largest impact over
no provisions, and is associated is with a reduction of 3.5 SIDS deaths on average. The total
ban on smoking in workplaces has no statistically signicant effect. By contrast, the intermediate
level restriction in restaurants has a positive and statistically signicant association with the SIDS
count over no provisions. Note that only four states have the separate ventilation requirement for
restaurants. Total bans and designated smoking area restrictions are both negatively associated
with SIDS. Total bans in smoking in restaurants have the largest effect, and are associated with
four fewer SIDS deaths on average.
As with restaurants, the requirement for separate ventilation in child care centers is positively
associated with SIDS counts, while all other levels of restrictions are negatively associated. The
ban when children are present (SFA-4) has the largest inuence, and is associated with a reduction
of 1.65deaths onaverage. Note that if the topthree categories for smokingindaycare are combined
(a ban when children are present for commercial day care sites; a ban when children are present for
commercial and home day care sites; a ban at all times for all types of day care arrangements), the
coefcient on this ban is negative and statistically signicant, and results in an average decrease
in 1.4 deaths.
Lastly, column 5 of Table 3 shows that the number of total bans in all three sits is negative and
statistically signicant. Here, each additional smoking ban is associated with an average reduction
of 1.5 SIDS deaths.
Table 4 shows the results where the tax on cigarettes is included instead of the price. The
tax results are qualitatively very similar to those presented in Table 3, with the coefcients on
cigarette taxes all negative and statistically signicant. In addition, the direction and magnitudes of
the smoke free air coefcients are also very similar to those in Table 3. The tax elasticities presented
here are much lower than the price elasticities and reveal that every one percent increase in the
real tax on cigarettes reduces SIDS deaths by a range of 0.160.18 percent. Using a calculation
similar to that described above for price, an average tax increase of 10 percent (2 cents) would
reduce the national death rate in 2003 from 0.53 to 0.52 per 1000 births.
The different magnitudes of the price and tax elasticities shown in Tables 3 and 4 is to be
expected because of the value at which the effects are estimated. However, comparable estimates
can be calculated. It can be shown mathematically that the tax elasticity with regards to the SIDS
count is equal to the price elasticity multiplied by the share of tax in the price and by the rate
at which price changes when tax changes. In my data, average state taxes are 17 percent of the
average price. Using state-level data from 1960 to 1990, Keeler et al. (1996) estimate that a one
cent increase in the cigarette tax leads to a 1.11 cent increase in the price. Using these numbers
and the price elasticity of 0.687 from column 5 of Table 3, the implied tax elasticity is 0.13.
This is fairly close to the estimated tax elasticity of 0.16 from column 5 of Table 4.
The results in Table 5 show the effect of the 1 year lags of cigarette prices, taxes and smoke
free air laws on the current year SIDS counts. Lagging these variables does little to alter the
124 S. Markowitz / Journal of Health Economics 27 (2008) 106133
results. The lagged price and tax coefcients remain negative and statistically signicant, and the
smoke free air law indicators retain the same pattern seen previously. The one exception is that
the total ban on smoking in private workplaces is now positively associated with SIDS deaths.
The purpose of lagging the variables is to try to test the hypothesis that prenatal smoking affects
SIDS deaths. The results in Table 5 do provide some evidence that prenatal smoking matters since
the previous years cigarette policies are generally negatively associated with current year SIDS
rates. I caution, however, that these results are merely suggestive since the cigarette variables tend
to be correlated over time, particularly the SFA laws, which change infrequently.
To help show that the results of the cigarette policy variables are not spurious, I examine the
effects of the cigarette variables on two outcomes that should not be related to smoking: (1)
infant deaths resulting from motor vehicle accidents and (2) infant deaths from drowning. These
two outcomes are chosen because they are potentially inuenced by risky parental behaviors, as
SIDS might be, yet logically should not be causally related to cigarette smoking. Any result here
showing that cigarette policies are related to these outcomes could indicate that omitted variables
are problematic for the SIDS models. These fatality counts come from NCHSs Multiple Cause
of Death Files for the same years as the SIDS data.
The results of these counterfactual models are presented in Table 6. The results for motor
vehicle fatalities are in the rst three columns. Column 1 shows the structural model and includes
the annual per capita sales of cigarettes, on which the coefcient is positive and statistically sig-
nicant. Sales are treated as exogenous here to demonstrate the positive correlation with fatalities.
It is difcult to explain why higher cigarette sales would directly lead to more infants dying in
automobile accidents, so an omitted third factor is likely confounding this result. The results of
the reduced form conrm this and show no statistically signicant effects for the cigarette prices,
taxes, or the smoking ban count. The results for drowning are shown in the last three columns of
Table 6. Here, none of the cigarette variables are statistically signicant, as expected, implying
that unobservables are not inuencing the cigarette policy results.
5.3. Year indicator results
As mentioned above, the Back to Sleep campaign has often been credited for dramatically
reducing the incidence of SIDS. The coefcients on the year indicators in the models provide
some measure of the effectiveness of this campaign. Table 2 shows the coefcients for all the time
dummies, and Fig. 2 summarizes these results by plotting the predicted SIDS death counts over
time. For each year (t), a predicted SIDS count (
S
t
) is calculated by the following formula:
S
t
= exp( xb
1
+rb
2
), (2)
where b
1
is a vector of coefcients for all of the independent variables excluding the year dummies,
x is the sample means of these independent variables, b
2
is the vector of year coefcients and r
takes on a value of 1 for the year in question and zero otherwise.
8
The coefcients are taken from
the model in column 5 of Table 3 that includes the price of cigarettes along with the smoking ban
count.
The strict interpretation of Fig. 2 is that it shows the trends in SIDS that occur after account-
ing for the observable factors that include cigarette policies, and the maternal, infant, and state
characteristics. That is, Fig. 2 shows the variation in SIDS that is attributed to unobserved annual
8
The calculation also includes the log of the average number of live births with a coefcient of one.
S
.
M
a
r
k
o
w
i
t
z
/
J
o
u
r
n
a
l
o
f
H
e
a
l
t
h
E
c
o
n
o
m
i
c
s
2
7
(
2
0
0
8
)
1
0
6
1
3
3
1
2
5
Table 6
Infant motor vehicle and drowning fatalities, select coefcients
Motor vehicle fatalities Drowning fatalities
(1) (2) (3) (4) (5) (6)
Annual per capita
cigarette sales
0.004(3.09) [0.002] 0.002(0.42) [0.0003]
Real cigarette
price
0.204 (0.94) [0.116] 0.243 (0.89) [0.043]
Real cigarette tax 0.206 (0.72) [0.117] 0.356 (0.96) [0.063]
Smoking ban
count
0.016 (0.39) [0.009] 0.018 (0.44) [0.010] 0.051 (0.78) [0.009] 0.058 (0.86) [0.010]
Note: t-statistics in parentheses, intercept not shown, and marginal effects in brackets. Columns 1 and 4 use annual data and n =1632. Columns 2, 3, 5 and 6 uses quarterly data and n =6324.
All models also include maternal, infant and state characteristics, year and state dummy variables. Quarterly dummies are included in Columns 2, 3, 5, and 6.
126 S. Markowitz / Journal of Health Economics 27 (2008) 106133
Fig. 2. Predicted vs. actual annual average SIDS counts.
trends that are common to all states. More generally, this picture shows the trends that can be
attributed to the national Back to Sleep campaign, along with trends in reporting practices that are
common across the country. For reference, the actual unadjusted average annual SIDS counts are
plotted against the annual average predicted counts in Fig. 2. Note that the actual average state
count is not adjusted for the population of live births, however, actual average state rates show a
similar pattern.
The predicted trend that is shown in Fig. 2 is different from the actual trend in some important
ways. First there is an initial increase in predicted SIDS cases. This could be due to increased
awareness and reporting of SIDS cases that followed the introduction of the ICD code for SIDS
in 1973. This initial increase is followed by as slight decline from 1979 to 1981, after which SIDS
increased again. This decline is not observed in the unadjusted data until 1980. The predicted
values hit a peak in 1989, the same year as the unadjusted data, and then decline until 1996, with
one slight increase in 1991. After 1996, the predicted SIDS counts increase until 2000. Again,
this increase is not observed in the unadjusted data. The predicted averages decrease, increase and
slightly decrease again in 2001, 2002 and 2003, respectively. It is interesting to note that 1996
was the year when the CDC issued a new reporting form for SIDS along with new guidelines
regarding the death scene investigation. It is likely that these practices are responsible for the
increase in predicted SIDS after 1996.
9
It is not clear from Fig. 2 that the Back to Sleep campaign is responsible for the downward
trend in SIDS cases that began in 1991 and continued through 1996. Recall that while the AAP
made its initial recommendation in 1992, the national campaign began in 1994. Some other
unobserved factors have to be responsible for the early years of the downturn. Note also that
in 1996 the AAP made its recommendation regarding the back only, rather than the side, as
9
I also tested models that exclude the year dummies and include instead sets of mutually exclusive groups of years along
with a linear time trend and the trend squared. The new variables indicate the following year groupings: (1) 19731978
(omitted reference category, which represents when ICD-8 codes were used); (2) 19791990 (ICD-9 codes rst used);
(3) 19911995 (ICD-9 codes plus autopsy required); (4) 19961998 (ICD-9 codes plus new reporting requirements);
(5) 19992003 (ICD-10 codes used). Including these new variables does not have an appreciable effect on the price and
smoke free air laws. Relative to the base group, the indicators for all other year groupings are negative and all but the
19992003 indicators are statistically signicant. The magnitude of the decline also increases until 19992003.
S
.
M
a
r
k
o
w
i
t
z
/
J
o
u
r
n
a
l
o
f
H
e
a
l
t
h
E
c
o
n
o
m
i
c
s
2
7
(
2
0
0
8
)
1
0
6
1
3
3
1
2
7
Table 7
Alternative SIDS models
(1) (2) (3) (4) (5)
Real cigarette price 0.664 (4.31) [8.409] 0.601 (4.54) [7.613]
Real cigarette tax 0.928 (4.25) [11.743] 0.815 (4.44) [10.325]
Smoking ban count 0.119 (3.02) [1.510] 0.107 (2.84) [1.350]
Maternal age at rst birth 0.155 (2.43) 0.122 (1.87) 0.102 (1.85) 0.119 (1.85) 0.102 (1.81)
High school degree 0.032 (0.08) 0.442 (1.10) 0.366 (1.00) 0.512 (1.25) 0.419 (1.12)
Some college 0.790 (0.76) 0.514 (0.52) 0.225 (0.24) 0.475 (0.49) 0.235 (0.25)
College or more 0.727 (0.80) 0.590 (0.73) 0.789 (1.12) 0.643 (0.82) 0.819 (1.17)
Black 0.844 (0.94) 1.211 (1.37) 1.294 (1.51) 1.172 (1.33) 1.248 (1.45)
Native American 5.553 (1.76) 4.612 (1.76) 4.620 (1.54) 3.853 (1.41) 3.988 (1.29)
Other race 5.995 (4.35) 4.273 (4.35) 3.741 (3.97) 4.294 (4.28) 3.884 (4.01)
Female baby 0.067 (0.07) 0.042 (0.05) 0.014 (0.01) 0.060 (0.07) 0.031 (0.03)
Low birth weight 2.573 (0.86)
Very low birth weight 3.901 (0.81)
State unemployment 0.006 (0.74) 0.005 (0.65) 0.006 (0.76) 0.008 (0.92) 0.008 (1.00)
State real income per capita 0.032 (0.97) 0.045 (1.56) 0.058 (2.44) 0.053 (1.90) 0.064 (2.60)
Price/tax elasticity 0.763 0.690 0.185 0.162
Note: t-statistics in parentheses, and intercept not shown. Brackets showmarginal effects; the change in the average quarterly SIDS count froma one unit change in the independent
variable. Coefcients on continuous variables can be interpreted as the percentage change in the average quarterly SIDS count froma one unit change in the independent variable.
All models also include year, quarter, and state dummy variables. N=6324.
128 S. Markowitz / Journal of Health Economics 27 (2008) 106133
the preferred sleep position. Any resulting reductions in SIDS likely have been masked by the
reporting changes issued by the CDCin the same year. In summary, it is impossible to disentangle
the effects of the Back to Sleep campaign from other nationwide factors that affected the SIDS
rates. Other time series data with more information about exposure to the information and sleeping
practices are necessary to adequately evaluate the campaign.
5.4. Maternal and infant characteristics
The results of the other included variables in Tables 35 are somewhat consistent with the
ndings of previous research on the predictors of SIDS, with a few notable exceptions. Older
maternal age is associated with lower SIDS death counts, as is higher per capita income. For
both of these variables, however, statistical signicance varies somewhat depending on the
model considered, but if signicance is achieved, it generally ranges between the 5 and 10
percent levels. The education variables, however, show no differences in having larger percent-
ages of the state population with high school or college degrees compared to no high school
degree.
Previous research has also found that children of non-whites are more likely to die of SIDS. This
result is duplicated here for states with larger percentages of mothers who are Native American,
but not for states with larger percentages of mothers who are black. It is interesting to note that
of all the racial and ethnic groups in the U.S., American Indians and Alaska Natives adults have
the highest rates of tobacco use (USDHHS, 1998). Previous research has also found low birth
weight and male gender to be risk factors for SIDS. Again, these results are not duplicated here.
The coefcients on gender, low birth weight, and very low birth weight are all statistically no
different from zero in all models.
One must be cautious in interpreting the coefcients for birth weight because along with
SIDS, low birth weight is a possible outcome of prenatal smoking. In fact, birth weights have
been used in previous research as dependent variables in models examining the effects of higher
cigarette taxes in increasing birth weights (Lien and Evans, 2005; Evans and Ringel, 1999).
This problem is explored in more depth in Table 7. The rst column presented here shows
results for the maternal and infant characteristics in a model that excludes the cigarette price
and policy measures. This is done specically to examine the coefcients on low birth weight
and very low birth weight. By excluding the cigarette policy variables from the model, the
coefcients on low birth weight and very low birth weight are positive and become larger in
magnitude. However, the standard errors are also high making these coefcients statistically
insignicant.
Given the potential relationship between the cigarette policy variables and birth weights, addi-
tional models are shown in Table 7 that exclude low birth weight and very low birth weight. The
results of the cigarette price, tax and SFA laws are all very similar to those shown in the previous
tables. For brevity, only results for the current price, tax and the smoking ban count are shown
here. Excluding the low birth weight variables also does not affect any of the other coefcients.
These results should not be surprising given that the birth weight variables do not contribute much
to the models.
6. Conclusions
Despite years of research, the causes of SIDS and related prevention strategies have been
elusive to researchers and to the public health community. To date, several risk factors have
S. Markowitz / Journal of Health Economics 27 (2008) 106133 129
been identied and a national campaign seeks to inform caretakers about the risky practices that
may lead to SIDS. While the primary message of the campaign is to put babies in a supine
position for sleep, the campaign also stresses the importance of a safe sleep surface and surround-
ings, which includes a smoke free environment. While SIDS rates have declined substantially
since the early 1990s, thousands of children still die suddenly each year from this unexplained
syndrome.
This paper takes a new approach to studying the prevention of SIDS by combining lessons
from epidemiology and economics. Epidemiological studies have shown that prenatal maternal
smoking and postnatal environmental smoke are major risk factors for SIDS deaths. Research in
economics has shown that smoking is inuenced by the determinants of the demand for cigarettes,
including the monetary price and restrictions on smoking in public places. By combining these
two relationships, I show that more stringent cigarette regulations have a distinct and direct
impact in reducing SIDS deaths. The largest reduction comes from changes in the monetary
price of cigaretteseach 10 percent increase in the real price of cigarettes reduces the average
number of SIDS deaths by a range of 6.97.6 percent. A ten percent increase in the real taxes on
cigarettes reduces SIDS deaths by a range of 1.61.8 percent. The difference in the magnitude
of the price and tax effects is not surprising since taxes make up only a proportion of cigarette
prices.
Restrictions on smoking in public places also may be life-saving to babies. For private
workplaces, the restriction requiring separate ventilation has the largest effect of all the work-
place regulations and is associated with a reduction of 3.5 SIDS deaths on average. Total
bans in smoking in restaurants are associated with four fewer SIDS deaths on average, and
bans on smoking in child care centers result in an average decrease in 1.4 deaths. The
effectiveness of higher cigarette prices and taxes and more stringent restrictions on smok-
ing in public places holds whether these factors are evaluated contemporaneously with the
SIDS cases, or lagged 1 year to represent the prices policies that existed during the prenatal
period.
The results of this paper also contribute to the evidence for the causal relationship between
smoking and SIDS, while avoiding the potential biased caused by omitted unobserved variables.
Models that estimate the direct effect of smoking using instrumental variables show a positive
relationship between aggregate measures of smoking and SIDS. The reduced form conrms this
result. Since the exogenous determinants of cigarette smoking should not directly affect SIDS
except through consumption, the ndings that higher cigarette prices and stricter clean indoor
air policies reduces SIDS is consistent with the theory that smoking causes SIDS. In sum, this
research highlights the message that a smoke free environment is very important for the health
and well-being of infants.
Acknowledgements
I would like to thank Andy Racine, Ted Joyce, Pinka Chatterji, Michael Grossman, Michael
Morrisey, Richard Frank, and two anonymous referees for extremely helpful comments and
suggestions. I would also like to thank Frank Chaloupka for providing me with some of the
data.
Appendix A
See Table A1.
1
3
0
S
.
M
a
r
k
o
w
i
t
z
/
J
o
u
r
n
a
l
o
f
H
e
a
l
t
h
E
c
o
n
o
m
i
c
s
2
7
(
2
0
0
8
)
1
0
6
1
3
3
Table A1
Alternative estimation techniques
(1) (2) (3) (4) (5)
Ordinary least squares regression: Dependent variable =SIDS rate
Cigarette price 0.331 (1.86) 0.330 (1.92) 0.306 (1.72) 0.274 (1.64) 0.286 (1.61)
SFA-1: private workplace 0.026 (0.34)
SFA-2: private workplace 0.171 (1.71)
SFA-3: private workplace 0.129 (1.23)
SFA-1: restaurant 0.069 (1.18)
SFA-2: restaurant 0.123 (1.29)
SFA-3: restaurant 0.197 (1.89)
SFA-1: child care center 0.096 (1.10)
SFA-2: child care center 0.207 (3.53)
SFA-3: child care center 0.043 (0.45)
SFA-4: child care center 0.173 (2.08)
SFA-5: child care center 0.159 (1.82)
Smoking ban count 0.087 (1.87)
Price elasticity 0.299 0.297 0.276 0.247 0.258
Negative binomial regressions: Dependent variable =SIDS count
Cigarette price 0.611 (4.10) [7.770] 0.615 (4.32) [7.822] 0.586 (4.47) [7.445] 0.572 (3.79) [7.278] 0.574 (4.08) [7.298]
SFA-1: private workplace 0.049 (0.88) [0.617]
SFA-2: private workplace 0.328 (5.33) [3.561]
SFA-3: private workplace 0.217 (1.81) [3.069]
SFA-1: restaurant 0.067 (1.69) [0.838]
SFA-2: restaurant 0.289 (4.72) [4.241]
SFA-3: restaurant 0.431 (3.84) [4.477]
SFA-1: child care center 0.064 (1.02) [0.793]
SFA-2: child care center 0.165 (2.80) [2.272]
SFA-3: child care center 0.058 (0.69) [0.718]
SFA-4: child care center 0.102 (1.45) [1.244]
SFA-5: child care center 0.092 (1.42) [1.118]
Smoking ban count 0.089 (1.80) [1.136]
Price elasticity 0.702 0.707 0.674 0.658 0.659
Note: t-statistics in parentheses, and intercept not shown. Coefcients in the OLS estimates show the absolute change in the SIDS count per 1000 live births from a one unit change in the
independent variable. Coefcients on continuous variables in the negative binomial regressions can be interpreted as the percentage change in the average quarterly SIDS count from a one
unit change in the independent variable. Brackets show marginal effects for the negative binomial regressions; the change in the average quarterly SIDS count from a one unit change in the
independent variable. All models also include maternal, infant and state characteristics, and year, quarter, and state dummy variables. N=6324.
S. Markowitz / Journal of Health Economics 27 (2008) 106133 131
References
Alm, B., Milerad, J., Wennergren, G., Skjaerven, R., Oyen, N., Norvenius, G., Daltveit, A.K., Helweg-Larsen, K.,
Markestad, T., Irgens, L.M., 1998. A case-control study of smoking and sudden infant death syndrome in the Scan-
dinavian countries 1992 to 1995: the Nordic Epidemiological SIDS Study. Archives of Disease in Childhood 78 (4),
329334.
American Academy of Pediatrics (AAP), 2005. The changing concept of sudden infant death syndrome: diagnostic coding
shifts, controversies regarding the sleeping environment, and new variables to consider in reducing risk. Pediatrics
116, 12451255.
Anderson, H.R., Cook, D.G., 1997. Passive smoking and sudden infant death syndrome: review of the epidemiological
evidence. Thorax 52, 10031009.
Anderson, M.E., Johnson, D.C., Batal, H.A., 2005. Sudden infant death syndrome and prenatal maternal smoking: rising
attributed risk in the back to sleep era. BMC Medicine 3 (4), 17.
Bertrand, M., Duo, E., Mullainathan, S., 2004. Howmuch should we trust differences-in-differences estimates? Quarterly
Journal of Economics 119 (1), 249275.
Blair, P.S., Fleming, P.J., Bensley, D., Smith, I., Bacon, C., Taylor, E., Berry, J., Golding, J., Tripp, J., 1996. Smoking and
the sudden infant death syndrome: results from 19935 case-control study for condential inquiry into stillbirths and
deaths in infancy. British Medical Journal 313 (7051), 195198.
Bradford, W.D., 2003. Pregnancy and the demand for cigarettes. American Economic Review 93 (5), 17521763.
Brooke, H., Gibson, A., Tappin, D., Brown, H., 1997. Case-control study of sudden infant death syndrome in Scotland
19925. British Medical Journal 314 (7093), 15161520.
Cameron, C.A., Trivedi, P.K., 1998. Regression Analysis of Count Data. Econometric Society Monograph No. 30.
Cambridge University Press.
Cameron, C.A., Trivedi, P.K., 2005. Microeconometrics Methods and Applications. Cambridge University Press, New
York.
Centers for Disease Control, March 3, 2006. Notice to readers: release of sudden, unexplained infant death investigation
reporting form. Morbidity and Mortality Weekly Report 55 (No. 8), 212213.
Centers for Disease Control (CDC), 2006b. Sudden infant death syndrome (SIDS): risk factors, http://www.cdc.gov/
SIDS/riskfactors.htm. Accessed July 21, 2006.
Centers for Disease Control, 1996. Guidelines for death scene investigation of sudden, unexplained infant deaths: recom-
mendations of the interagency panel on sudden infant death syndrome. Morbidity and Mortality Weekly Report 45
(RR10), 122.
Centers for Disease Control (CDC), October 25, 1991. Current trends cigarette smoking among reproductive-aged
womenbehavioral risk factor surveillance system, 1989. Morbidity and Mortality Weekly Report 40 (MM42),
719723.
Chaloupka, F.J., 1992. Clean Indoor air laws, addiction, and cigarette smoking. Applied Economics 24 (2), 193
205.
Chaloupka, F.J., Warner, K.E., 2000. The economics of smoking. In: Anthony, J., Cuyler, Joseph, P., Newhouse
(Eds.), The Handbook of Health Economics. North-Holland, Elsevier Science B.V, New York, pp. 1539
1627.
Colman, G., Michael, G., Ted, J., 2003. The effect of cigarette excise taxes on smoking before, during and after pregnancy.
Journal of Health Economics 22 (6), 10531072.
Czart, C., Pacula, R.L., Chaloupka, F.J., Wechsler, H., 2001. The impact of prices and control policies on cigarette smoking
among college students. Contemporary Economic Policy 19 (2), 135149.
Evans, W.N., Farrelly, M.C., Montgomery, E., 1999. Do workplace smoking bans reduce smoking. American Economic
Review 89 (4), 728747.
Evans, W.N., Ringel, J., 1999. Can higher cigarette taxes improve birth outcomes? Journal of Public Economic 72,
135154.
Filiano, J.J., Kinney, H.C., 1994. A perspective on neuropathologic ndings in victims of sudden infant death syndrome:
the triple-risk model. Biology of the Neonate 65 (34), 194197.
Gallet, C.A., 2004. The efcacy of state-level antismoking laws: demand and supply considerations. Journal of Economics
and Finance 28 (3), 404412.
Getahun, D., Amre, D., Rhoads, G.G., Demissie, K., 2004. Maternal and obstetric risk factors for sudden infant death
syndrome in the United States. Obstetrics and Gynecology 103 (4), 646652.
Gruber, J., Koszegi, B., 2001. Is addiction Rational? Theory and evidence. The Quarterly Journal of Economics 116
(4), 12611303.
132 S. Markowitz / Journal of Health Economics 27 (2008) 106133
Hunt, C.E., Hauck, F.R., June 20, 2006. Sudden infant death syndrome. Canadian Medical Association Journal 174 (13),
18611869.
Keeler, T.E., Hu, T., Barnett, P.G., Manning, W.G., Sung, H., 1996. Do cigarette producers price-discriminate by
state? An empirical analysis of local cigarette pricing and taxation. Journal of Health Economics 15 (4), 499
512.
Klonoff-Cohen, H.S., Edelstein, S.L., Lefkowitz, E.S., Srinivasan, I.P., Kaegi, D., Chang, J.C., Wiley, K.J., 1995. The
effect of passive smoking and tobacco exposure through breast milk on sudden infant death syndrome. Journal of the
American Medical Association 273 (10), 795798.
Lien, D.S., Evans, N.W., 2005. Estimating the impact of large cigarette tax hikes: the case of maternal smoking and low
birth weight. Journal of Human Resources 40 (2), 373392.
Mage, D.T., 2004. Seasonal variation of sudden infant death syndrome in Hawaii. Journal of Epidemiology and Community
Health 58 (11), 912916.
Malloy, M.H., MacDorman, M., 2005. Changes in the classication of sudden unexpected infant deaths: United States
19922001. Pediatrics 115, 12471253.
Mitchell, E.A., Ford, R.P., Stewart, A.W., Taylor, B.J., Becroft, D.M., Thompson, J.M., Scragg, R., Hassall, I.B., Barry,
D.M., Allen, E.M., 1993. Smoking and the sudden infant death syndrome. Pediatrics 91 (5), 893896.
Mitchell, E.A., Tuohy, P.G., Brunt, J.M., Thompson, J.M., Clements, M.S., Stewart, A.W., Ford, R.P., Taylor, B.J., 1997.
Risk factors for sudden infant death syndrome following the prevention campaign in New Zealand: a prospective
study. Pediatrics 100 (5), 835840.
National Center for Health Statistics Data File Documentations, Natality, 19732003 (machine readable data le and
documentation, CD-ROM). National Center for Health Statistics, Hyattsville, Maryland.
National Center for Health Statistics. Data File Documentations, Multiple Cause-of-Death, 19732003 (machine readable
data le and documentation, CD-ROM). National Center for Health Statistics, Hyattsville, Maryland.
Ohsfeldt, R.L., Boyle, R.G., Capilouto, E.L., 1999. Tobacco taxes, smoking restrictions, and tobacco use. In: Frank, C.,
Michael, G., Warren, B., Henry, S. (Eds.), The Economic Analysis of Substance Use and Abuse: an Integration of
Econometric and Behavioral Economic Research. The University of Chicago Press, Chicago, pp. 1530.
Orzechowski, Walker, 2005. Tax Burden on Tobacco: Historical Compilation.
Paterson, D.S., Trachtenberg, F.L., Thompson, E.G., Belliveau, R.A., Beggs, A.H., Darnall, R., Chadwick, A.E., Krous,
H.F., Kinney, H.C., November 1, 2006. Multiple serotonergic brainstemabnormalities insuddeninfant deathsyndrome.
Journal of the American Medical Association 296 (17), 21242132.
Pickett, K.E., Luo, Y., Lauderdale, D.S., 2005. Widening social inequalities in risk for sudden infant death syndrome.
American Journal of Public Health 95 (11), 19761981.
Ringel, J.S., Evans, W.N., 2001. Cigarette taxes and maternal smoking. American Journal of Public Health 91 (11),
18511856.
Schoendorf, K.C., Kiely, J.L., 1992. Relationship of sudden infant death syndrome to maternal smoking during and after
pregnancy. Pediatrics 90 (6), 905908.
Shapiro-Mendoza, C.K., Tomashek, K.M., Anderson, R.N., Wingo, J., 2006. Recent national trends in sudden, unexpected
infant deaths: more evidence supporting a change in classication or reporting. American Journal of Epidemiology
163 (8), 762769.
Spencer, N., Logan, S., 2004. Sudden unexpected death in infancy and socioeconomic status: a systematic review. Journal
of Epidemiology and Community Health 58 (5), 366373.
Tauras, J.A., 2004. Public policy and some-day smoking among adults. Journal of Applied Economics 7 (1), 137162.
Tauras, J.A., 2006. Smoke free air laws, cigarette prices, and adult cigarette demand. Economic Inquiry 44 (2), 333
342.
U.S. Dept. of Health and Human Services, 2006. The Health Consequences of Involuntary Exposure to Tobacco Smoke: a
Report of the Surgeon General. U.S. Dept. of Health and Human Services, Centers for Disease Control and Prevention,
Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion,
Ofce on Smoking and Health, Atlanta, Ga.
U.S. Department of Health and Human Services, 1998. Tobacco Use Among U.S. Racial/Ethnic Minority Groups-African
Americans, American Indians and Alaska Natives, Asian Americans and Pacic Islanders and Hispanics: a Report of
the Surgeon General. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention,
National Center for Chronic Disease Prevention and Health Promotion, Ofce on Smoking and Health, Atlanta,
Georgia.
U.S. Department of Health and Human Services, 1994. Preventing Tobacco Use Among Young People: A Report of the
Surgeon General. Public Health Service, Center for Disease Control and Prevention, National Center for Chronic
Disease Prevention and Health Promotion, Ofce on Smoking and Health, Atlanta, Georgia.
S. Markowitz / Journal of Health Economics 27 (2008) 106133 133
Wasserman, J., Manning, W.G., Newhouse, J.P., Winkler, J.D., 1991. The effects of excise taxes and regulations on
cigarette smoking. Journal of Health Economics 10 (1), 4364.
Willinger, M., Hoffman, H.J., Wu, K.-T., Hou, J.-R., Kessler, R.C., Ward, S.L., Keens, T.G., Corwin, M.J., 1998. Factors
associated with the transition to nonprone sleep positions of infants in the United States: the national infant sleep
position study. Journal of the American Medical Association 280, 329335.
Wooldridge, J.M., 2002. Econometric Analysis of Cross Section and Panel Data. MIT Press, Cambridge, MA.
Das könnte Ihnen auch gefallen
- MULTIPLE CHOICE. Choose The One Alternative That Best Completes The Statement or Answers The QuestionDokument65 SeitenMULTIPLE CHOICE. Choose The One Alternative That Best Completes The Statement or Answers The QuestionJamaica DavidNoch keine Bewertungen
- Jehle Solutions PDFDokument5 SeitenJehle Solutions PDFzsadiqueNoch keine Bewertungen
- Jhe Asthma LTDokument11 SeitenJhe Asthma LTdinna_dinunNoch keine Bewertungen
- Prevalence of Asthma in Australian ChildrenDokument4 SeitenPrevalence of Asthma in Australian Childrenoktha_pohanNoch keine Bewertungen
- Demographic Research: Volume 32, Article 4, Pages 107 Published 9 January 2015Dokument42 SeitenDemographic Research: Volume 32, Article 4, Pages 107 Published 9 January 2015paaztiiNoch keine Bewertungen
- Maternal Lifestyle Factors in Pregnancy and Congenital Heart Defects in Offspring: Review of The Current EvidenceDokument11 SeitenMaternal Lifestyle Factors in Pregnancy and Congenital Heart Defects in Offspring: Review of The Current EvidenceIkrimahNoch keine Bewertungen
- Cancer in Working-Age Is Not Associated With Childhood AdversitiesDokument6 SeitenCancer in Working-Age Is Not Associated With Childhood AdversitiesBadger6Noch keine Bewertungen
- Review: Developing Asthma in Childhood From Exposure To Secondhand Tobacco Smoke: Insights From A Meta-RegressionDokument8 SeitenReview: Developing Asthma in Childhood From Exposure To Secondhand Tobacco Smoke: Insights From A Meta-RegressionJules IuliaNoch keine Bewertungen
- Smoking InfertilityDokument8 SeitenSmoking Infertilityjames.armstrong35Noch keine Bewertungen
- Higher Education and Health Investments: Does More Schooling Affect Preventive Health Care Use?Dokument33 SeitenHigher Education and Health Investments: Does More Schooling Affect Preventive Health Care Use?Sarmad AslamNoch keine Bewertungen
- The Determinants of The Health of The PeopleDokument19 SeitenThe Determinants of The Health of The PeopleDina KaraNoch keine Bewertungen
- Association Between Maternal Age and Birth Defects of Unknown Etiology United States, 1997 2007Dokument18 SeitenAssociation Between Maternal Age and Birth Defects of Unknown Etiology United States, 1997 2007Rizka RamadaniNoch keine Bewertungen
- Families Family Policy and The SDGs (1) - 102-129Dokument28 SeitenFamilies Family Policy and The SDGs (1) - 102-129Sylvia MaharanyNoch keine Bewertungen
- TC Record PDFDokument17 SeitenTC Record PDFPeter MuennigNoch keine Bewertungen
- The Global Burden of Neonatal Hypothermia: Systematic Review of A Major Challenge For Newborn SurvivalDokument11 SeitenThe Global Burden of Neonatal Hypothermia: Systematic Review of A Major Challenge For Newborn SurvivalE=MC2Noch keine Bewertungen
- Edited Peds-Neonates Research Paper Sids Research Class - FinalDokument6 SeitenEdited Peds-Neonates Research Paper Sids Research Class - Finalapi-733590799Noch keine Bewertungen
- E A W P S: Conomic Nalysis Orking Aper EriesDokument26 SeitenE A W P S: Conomic Nalysis Orking Aper EriesAgus DurmanNoch keine Bewertungen
- BBLR AsmaDokument6 SeitenBBLR AsmaSeptia Pristi RahmahNoch keine Bewertungen
- Gender Matters: An Integrated Model For Understanding Men's and Women's HealthDokument11 SeitenGender Matters: An Integrated Model For Understanding Men's and Women's Healthcharming_angel1352204Noch keine Bewertungen
- Psychosocial Factors and Obstetric Complications: B.ChalmersDokument7 SeitenPsychosocial Factors and Obstetric Complications: B.ChalmersRafael BagusNoch keine Bewertungen
- Hum. Reprod.-2012-Klemetti-3315-20Dokument6 SeitenHum. Reprod.-2012-Klemetti-3315-20Putri Nilam SariNoch keine Bewertungen
- 330 FullDokument5 Seiten330 Fullshe-docNoch keine Bewertungen
- BBL, Imt, AsmaDokument7 SeitenBBL, Imt, AsmaYenny Adelia 黃梅珠Noch keine Bewertungen
- Childhood ObesityDokument42 SeitenChildhood ObesityLaTasha Ann Steven100% (3)
- Nursing Research PaperDokument19 SeitenNursing Research Paperapi-401771498Noch keine Bewertungen
- Humrep Des398 FullDokument9 SeitenHumrep Des398 FullKinjal ShahNoch keine Bewertungen
- Alcohol DrugsDokument15 SeitenAlcohol DrugsRomario JarrettNoch keine Bewertungen
- Integrative ReviewDokument17 SeitenIntegrative Reviewapi-430735052Noch keine Bewertungen
- ACE Finished - Docx1234Dokument10 SeitenACE Finished - Docx1234Nadia umwaliNoch keine Bewertungen
- Wazir Ali AssignmentDokument15 SeitenWazir Ali AssignmentMUHAMMAD AHMEDNoch keine Bewertungen
- INTRODUCTIONDokument7 SeitenINTRODUCTIONBenjamin SimwingaNoch keine Bewertungen
- Pregnancy Related Mortality in The United States,.11Dokument8 SeitenPregnancy Related Mortality in The United States,.11melisaberlianNoch keine Bewertungen
- Smoking and Blood Sugar Level: An Important Cause of Cardiovascular Diseases Among AustraliansDokument11 SeitenSmoking and Blood Sugar Level: An Important Cause of Cardiovascular Diseases Among Australiansinflibnet inflibnetNoch keine Bewertungen
- Macrosomia and Diabetic Maternal 2010Dokument12 SeitenMacrosomia and Diabetic Maternal 2010Ade Gustina SiahaanNoch keine Bewertungen
- Ijc 22717Dokument7 SeitenIjc 22717Tony DávilaNoch keine Bewertungen
- Anticipating PGDDokument10 SeitenAnticipating PGDArlin Chyntia DewiNoch keine Bewertungen
- Jurnal 4Dokument11 SeitenJurnal 4keperawatan fkNoch keine Bewertungen
- A Descriptive Model of Preventability in Maternal Morbidity and MortalityDokument6 SeitenA Descriptive Model of Preventability in Maternal Morbidity and MortalityAnnissa SyairaNoch keine Bewertungen
- Consequences of Early Parental Loss and Separation For Health and Well-Being in MidlifeDokument7 SeitenConsequences of Early Parental Loss and Separation For Health and Well-Being in MidlifeDanielle DaniNoch keine Bewertungen
- Chapter 1 Reproductive Health EpidemiologyyDokument13 SeitenChapter 1 Reproductive Health EpidemiologyyAnnisa NurrachmawatiNoch keine Bewertungen
- Maternal Smoking - NEC MortalityDokument7 SeitenMaternal Smoking - NEC MortalityGlen LazarusNoch keine Bewertungen
- Living With The Past: Evolution, Development and Patterns of Disease.Dokument5 SeitenLiving With The Past: Evolution, Development and Patterns of Disease.LQWERT100% (1)
- Risk Factor ViolenceDokument23 SeitenRisk Factor ViolenceadeNoch keine Bewertungen
- SSM 46 03 Joung PDFDokument11 SeitenSSM 46 03 Joung PDFLoredana StaniloiuNoch keine Bewertungen
- Etiology Autism Spectrum DisorderDokument11 SeitenEtiology Autism Spectrum DisorderfsaajaNoch keine Bewertungen
- Dose-Response Association Between Maternal Smoking DuringDokument13 SeitenDose-Response Association Between Maternal Smoking DuringFebi Ananta Indah CahyaniNoch keine Bewertungen
- Income Inequality and Health Status: A Nursing Issue: AuthorsDokument5 SeitenIncome Inequality and Health Status: A Nursing Issue: AuthorsWinni FebriariNoch keine Bewertungen
- dmt2 Lansia 2Dokument3 Seitendmt2 Lansia 2Lavenia JulianiNoch keine Bewertungen
- McLaren Wilde Temperature Gender 9292016Dokument8 SeitenMcLaren Wilde Temperature Gender 9292016Rishabh Naresh JainNoch keine Bewertungen
- Smoking and CHDDokument19 SeitenSmoking and CHDAnonymous NeRC5JYiSNoch keine Bewertungen
- Inflammatory Mediators in The ElderlyDokument13 SeitenInflammatory Mediators in The ElderlyCh Bilal AhmedNoch keine Bewertungen
- Diantara Dingin Malam Kau Kembali Hiasi Temaram Dengan Air Mata Remuk Redam Kau Khawatir Kisah Kita Suram Kau Dan Aku Hampir Menyerah Melepas HarapDokument5 SeitenDiantara Dingin Malam Kau Kembali Hiasi Temaram Dengan Air Mata Remuk Redam Kau Khawatir Kisah Kita Suram Kau Dan Aku Hampir Menyerah Melepas HarapYosie Yulanda PutraNoch keine Bewertungen
- How Can Primary Care Providers Manage Pediatric Obesity in The Real World?Dokument12 SeitenHow Can Primary Care Providers Manage Pediatric Obesity in The Real World?Iarias22Noch keine Bewertungen
- Preventing Low Birth WeightDokument17 SeitenPreventing Low Birth Weightpeter_mrNoch keine Bewertungen
- Nursing Research PaperDokument24 SeitenNursing Research Paperapi-455624162Noch keine Bewertungen
- Pre-Eclampsia Rates in The United States, 1980-2010: Age-Period-Cohort AnalysisDokument9 SeitenPre-Eclampsia Rates in The United States, 1980-2010: Age-Period-Cohort AnalysistiyacyntiaNoch keine Bewertungen
- Original ContributionDokument10 SeitenOriginal ContributionzzakieNoch keine Bewertungen
- Nursing Impact On Maternal and Infant Mortality in The United States.Dokument7 SeitenNursing Impact On Maternal and Infant Mortality in The United States.boniface mogisoNoch keine Bewertungen
- JDS 392Dokument10 SeitenJDS 392fifahcantikNoch keine Bewertungen
- Risk Factors For Eclampsia: A Population-Based Study in Washington State, 1987-2007Dokument7 SeitenRisk Factors For Eclampsia: A Population-Based Study in Washington State, 1987-2007Syerra Saindari PutriNoch keine Bewertungen
- The Effect of Abortion Legalization On Sexual Behavior - EvidenceDokument28 SeitenThe Effect of Abortion Legalization On Sexual Behavior - Evidenceabarroexcil7Noch keine Bewertungen
- Obesity and Lung Disease: A Guide to ManagementVon EverandObesity and Lung Disease: A Guide to ManagementAnne E. DixonNoch keine Bewertungen
- Otro Oaxaca PDFDokument6 SeitenOtro Oaxaca PDFEugenio MartinezNoch keine Bewertungen
- Grej797282.ww1 Default PDFDokument2 SeitenGrej797282.ww1 Default PDFEugenio MartinezNoch keine Bewertungen
- 1 s2.0 S000039 Main PDFDokument25 Seiten1 s2.0 S000039 Main PDFEugenio MartinezNoch keine Bewertungen
- Nirenberg PDFDokument3 SeitenNirenberg PDFEugenio MartinezNoch keine Bewertungen
- JSciRes1128-5125773 141417 PDFDokument7 SeitenJSciRes1128-5125773 141417 PDFEugenio MartinezNoch keine Bewertungen
- A Numerical Algorithm With Preference Statements To Evaluate The Performance of ScientistsDokument22 SeitenA Numerical Algorithm With Preference Statements To Evaluate The Performance of ScientistsEugenio MartinezNoch keine Bewertungen
- Beyond Traditional Citations: Leap On Clouds To Capture Virtual Metrics!Dokument2 SeitenBeyond Traditional Citations: Leap On Clouds To Capture Virtual Metrics!Eugenio MartinezNoch keine Bewertungen
- Fiscal Decentralization, Central Bank Independence and Inflation: A Panel InvestigationDokument4 SeitenFiscal Decentralization, Central Bank Independence and Inflation: A Panel InvestigationEugenio MartinezNoch keine Bewertungen
- Does Central Bank Independence Lower Inflation?: Mustafa Ismihan, F. Gulcin OzkanDokument5 SeitenDoes Central Bank Independence Lower Inflation?: Mustafa Ismihan, F. Gulcin OzkanEugenio MartinezNoch keine Bewertungen
- Journal of International Money and Finance: Sami Alpanda, Adam HonigDokument21 SeitenJournal of International Money and Finance: Sami Alpanda, Adam HonigEugenio MartinezNoch keine Bewertungen
- Central Banks and Inflation Targeting in Perspective: Andrew F. BrimmerDokument5 SeitenCentral Banks and Inflation Targeting in Perspective: Andrew F. BrimmerEugenio MartinezNoch keine Bewertungen
- Construction Incomes LAC 2011 - MarzoDokument306 SeitenConstruction Incomes LAC 2011 - MarzoEugenio MartinezNoch keine Bewertungen
- Summarizing Population Health: Fryback QALY Search BooksDokument1 SeiteSummarizing Population Health: Fryback QALY Search BooksEugenio MartinezNoch keine Bewertungen
- Unclos CasesDokument53 SeitenUnclos CasesXiaoyu ZhaoNoch keine Bewertungen
- Macion Vs GuianiDokument2 SeitenMacion Vs GuianiMark CoNoch keine Bewertungen
- The Three Fundamental Economic Questions: What To Produce, How, and For Whom?Dokument4 SeitenThe Three Fundamental Economic Questions: What To Produce, How, and For Whom?Shenel OrtegaNoch keine Bewertungen
- Financial Derivatives ON Exotic Options: Presented By: Tejas PrabhuDokument34 SeitenFinancial Derivatives ON Exotic Options: Presented By: Tejas PrabhuajayjhaitmNoch keine Bewertungen
- Market Study of Refined Edible OilDokument13 SeitenMarket Study of Refined Edible Oilmulugeta tetemkeNoch keine Bewertungen
- FM AssignmentDokument3 SeitenFM Assignmentjeaner2008Noch keine Bewertungen
- NSB B - C: Boardman, Greenberg, Vining, Weimer / Cost-Benefit Analysis, 3 Edition Instructor's Manual 1-1Dokument5 SeitenNSB B - C: Boardman, Greenberg, Vining, Weimer / Cost-Benefit Analysis, 3 Edition Instructor's Manual 1-1Elba Joy Alagao AbadNoch keine Bewertungen
- Fundamental Analysis and Technical Analysis Project Report On Power SectorDokument91 SeitenFundamental Analysis and Technical Analysis Project Report On Power Sectorgouttam pandaNoch keine Bewertungen
- CasioDokument31 SeitenCasioTanjeem100% (2)
- Children Wear in MoroccoDokument2 SeitenChildren Wear in MoroccoHicham DrifNoch keine Bewertungen
- BKM Chapter 7Dokument43 SeitenBKM Chapter 7Isha0% (1)
- Essentials of Economics 4th Edition Hubbard Solutions ManualDokument22 SeitenEssentials of Economics 4th Edition Hubbard Solutions Manualfloroncozwkk100% (22)
- Assignment 1 BUSI 3008Dokument21 SeitenAssignment 1 BUSI 3008Irena MatuteNoch keine Bewertungen
- Pricing of A Product:-: 1. Fit and Flare DressDokument5 SeitenPricing of A Product:-: 1. Fit and Flare DressAMAN RAJNoch keine Bewertungen
- Technical AnalysisDokument65 SeitenTechnical AnalysisrinekshjNoch keine Bewertungen
- Questions On Bond PricingDokument11 SeitenQuestions On Bond PricingMinji Michelle JNoch keine Bewertungen
- Chapter 2 InventoriesDokument10 SeitenChapter 2 Inventoriesvea domingoNoch keine Bewertungen
- Caf-3 CmaDokument600 SeitenCaf-3 CmaHacker No.1Noch keine Bewertungen
- The Effectiveness of Foreign Aid: A Case Study of NepalDokument359 SeitenThe Effectiveness of Foreign Aid: A Case Study of Nepalprabin ghimireNoch keine Bewertungen
- Chapter 4Dokument26 SeitenChapter 4Sozia TanNoch keine Bewertungen
- Business Plan HT 1Dokument21 SeitenBusiness Plan HT 1Nipay Vince100% (1)
- Sample Customer Satisfaction Questionnaire TemplatesDokument4 SeitenSample Customer Satisfaction Questionnaire TemplatesMuhammad Ali FiazNoch keine Bewertungen
- MR Ashin Gunasettha Sin-Rgn Date Changed TicketDokument3 SeitenMR Ashin Gunasettha Sin-Rgn Date Changed TicketGunaNoch keine Bewertungen
- Project On The Production of Woven PP BagsDokument29 SeitenProject On The Production of Woven PP BagsZeyinu Ahmed Moh100% (2)
- Chapter 7 - Inventory ManagementDokument52 SeitenChapter 7 - Inventory ManagementTrey Holton100% (2)
- All Question of Saifurs MathDokument6 SeitenAll Question of Saifurs Mathjannatul mouNoch keine Bewertungen
- Inventory Control Models: EOQ ModelDokument12 SeitenInventory Control Models: EOQ ModelArslan MunawarNoch keine Bewertungen
- Net Present Value - NPV: Capital BudgetingDokument4 SeitenNet Present Value - NPV: Capital BudgetingCris Marquez100% (1)