Das könnte Ihnen auch gefallen
- The Circulatory System-: TransportDokument13 SeitenThe Circulatory System-: TransportJerilee SoCute WattsNoch keine Bewertungen
- PDFDokument64 SeitenPDFJerilee SoCute WattsNoch keine Bewertungen
- Digestive SystemDokument48 SeitenDigestive SystemJerilee SoCute WattsNoch keine Bewertungen
- Skin Diseases Disorders ConditionsDokument104 SeitenSkin Diseases Disorders ConditionsJerilee SoCute WattsNoch keine Bewertungen
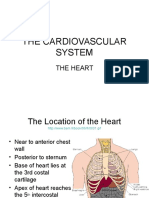
- The HeartDokument42 SeitenThe HeartJerilee SoCute WattsNoch keine Bewertungen
- SkinDokument43 SeitenSkinFhen Farrel100% (1)
- Respiration System PP TDokument57 SeitenRespiration System PP Troyanirudh99Noch keine Bewertungen
- The Digestive System Part 1Dokument28 SeitenThe Digestive System Part 1Jerilee SoCute WattsNoch keine Bewertungen
- Urinary SystemDokument105 SeitenUrinary SystemJerilee SoCute WattsNoch keine Bewertungen
- Reproductive SystemDokument80 SeitenReproductive SystemJerilee SoCute WattsNoch keine Bewertungen
- The Lymphatic SystemDokument50 SeitenThe Lymphatic SystemJerilee SoCute Watts100% (1)
- Reproduction Summary NotesDokument16 SeitenReproduction Summary NotesJerilee SoCute WattsNoch keine Bewertungen
- The Digestive System: Cont'd (From Swallowing)Dokument56 SeitenThe Digestive System: Cont'd (From Swallowing)Jerilee SoCute WattsNoch keine Bewertungen
- The Conducting System of The HeartDokument37 SeitenThe Conducting System of The HeartJerilee SoCute WattsNoch keine Bewertungen
- Pulmonary and Systemic CircuitsDokument38 SeitenPulmonary and Systemic CircuitsJerilee SoCute WattsNoch keine Bewertungen
- Reproduction and DevelopmentDokument53 SeitenReproduction and DevelopmentJerilee SoCute WattsNoch keine Bewertungen
- The Digestive System EssayDokument3 SeitenThe Digestive System EssayJerilee SoCute Watts0% (1)
- Respiratory System 1Dokument29 SeitenRespiratory System 1Jerilee SoCute WattsNoch keine Bewertungen
- Lecture 21 - Respiratory SystemDokument59 SeitenLecture 21 - Respiratory SystemSkyBirdNoch keine Bewertungen
- Review Questions - HeartDokument1 SeiteReview Questions - HeartJerilee SoCute WattsNoch keine Bewertungen
- Respiratory Centers of The BrainDokument36 SeitenRespiratory Centers of The BrainJerilee SoCute WattsNoch keine Bewertungen
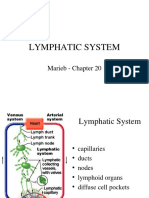
- Lymphatic System: Marieb Chapter 20Dokument22 SeitenLymphatic System: Marieb Chapter 20Jerilee SoCute WattsNoch keine Bewertungen
- Human ReproductionDokument42 SeitenHuman ReproductionAliDarimiKRNoch keine Bewertungen
- Respiratory System 2Dokument39 SeitenRespiratory System 2Jerilee SoCute WattsNoch keine Bewertungen
- Reproductive System DisordersDokument62 SeitenReproductive System DisordersJerilee SoCute Watts100% (2)
- Lecture 1 Cardiovascular SystemDokument70 SeitenLecture 1 Cardiovascular SystemJerilee SoCute WattsNoch keine Bewertungen
- Reproduction NotesDokument20 SeitenReproduction NotesMario BaemamentengNoch keine Bewertungen
- Past Papers Section2Dokument13 SeitenPast Papers Section2Jerilee SoCute Watts50% (2)
- Unit 6 OsmolarityDokument59 SeitenUnit 6 Osmolaritykrystal1994Noch keine Bewertungen
- Platelets and HemostasisDokument19 SeitenPlatelets and HemostasisJerilee SoCute WattsNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Let ReviewerDokument90 SeitenLet ReviewerRomeo BatanNoch keine Bewertungen
- Shame ErskineDokument17 SeitenShame ErskineSonja SudimacNoch keine Bewertungen
- Constructing Social Identity A Language Socialization Perspective PDFDokument21 SeitenConstructing Social Identity A Language Socialization Perspective PDFDelfa OtrNoch keine Bewertungen
- Lectura 5-Semanas 5 y 6 - Chapter 10-Basic Psychological Needs Theory. Ryan y Deci (2017)Dokument33 SeitenLectura 5-Semanas 5 y 6 - Chapter 10-Basic Psychological Needs Theory. Ryan y Deci (2017)Alvaro ZumaranNoch keine Bewertungen
- Juli Lit ReviwDokument2 SeitenJuli Lit ReviwjuliNoch keine Bewertungen
- Ashirom@post Tau Ac IlDokument32 SeitenAshirom@post Tau Ac IlkrizaricaNoch keine Bewertungen
- CBR Kls C-121-159Dokument39 SeitenCBR Kls C-121-159Azizah SyahraNoch keine Bewertungen
- Pschology Assignment G-3Dokument7 SeitenPschology Assignment G-3wudineh debebeNoch keine Bewertungen
- Sinclair, Soldat 1997Dokument21 SeitenSinclair, Soldat 1997rnuevo2Noch keine Bewertungen
- The Satisfaction With Life Scale: Journal of Personality AssessmentDokument5 SeitenThe Satisfaction With Life Scale: Journal of Personality AssessmentNaneun NabilahNoch keine Bewertungen
- Janusian Thinking As A Psychological ProcessDokument23 SeitenJanusian Thinking As A Psychological ProcessRicardo GarciaNoch keine Bewertungen
- Brown10 0Dokument183 SeitenBrown10 0infochromatikaNoch keine Bewertungen
- Career Anchors PDFDokument1.049 SeitenCareer Anchors PDFMarya Malik WaniNoch keine Bewertungen
- The Right Brain Implicit Self Lies at The Core - Allan B SchoreDokument27 SeitenThe Right Brain Implicit Self Lies at The Core - Allan B Schorepavnav72100% (2)
- Psychology - Class XII - Chapter 06Dokument23 SeitenPsychology - Class XII - Chapter 06shaannivasNoch keine Bewertungen
- 10.1016 J.elerAP.2013.01.004 Transforming Homo Economicus Into Homo Ludens A Field Experiment On Gamification in A Utilitarian Peer To Peer Trading ServiceDokument10 Seiten10.1016 J.elerAP.2013.01.004 Transforming Homo Economicus Into Homo Ludens A Field Experiment On Gamification in A Utilitarian Peer To Peer Trading ServiceElnaz NasirzadeNoch keine Bewertungen
- Judging of Dairy ProductsDokument153 SeitenJudging of Dairy ProductsTanmay ParekhNoch keine Bewertungen
- Psychological Interventions For Acute Pediatric Pain: Christina Liossi and Linda S FranckDokument16 SeitenPsychological Interventions For Acute Pediatric Pain: Christina Liossi and Linda S FranckbangkitayuNoch keine Bewertungen
- G.A.M Chapter 8Dokument40 SeitenG.A.M Chapter 8Christine100% (2)
- Motivation: Cognitive Motive Focuses On A Person's Needs For Being Oriented Towards The Environment and Achieving A SenseDokument4 SeitenMotivation: Cognitive Motive Focuses On A Person's Needs For Being Oriented Towards The Environment and Achieving A SenseUmair Nadeem100% (1)
- Happy Objects PDFDokument33 SeitenHappy Objects PDFFernando OrozcoNoch keine Bewertungen
- Negotiation Journal - Escalation and MindfulnessDokument28 SeitenNegotiation Journal - Escalation and MindfulnessvinumentisNoch keine Bewertungen
- Effects of Appraisal System On Employees' ProductivityDokument50 SeitenEffects of Appraisal System On Employees' ProductivityDaniel Obasi100% (1)
- Why We Like To Watch Sad FilmsDokument15 SeitenWhy We Like To Watch Sad FilmsΕιρηνη ΚαλογερακηNoch keine Bewertungen
- Lovebird Scale 04072023Dokument59 SeitenLovebird Scale 04072023Astha RajputNoch keine Bewertungen
- Sarah Ahmed - Happy ObjectsDokument29 SeitenSarah Ahmed - Happy ObjectsEleonora Croquer0% (1)
- Evaluating A Servicescape: The Effect of Cognition and EmotionDokument16 SeitenEvaluating A Servicescape: The Effect of Cognition and EmotionHimanshu MasandNoch keine Bewertungen
- Penner, L.A. (2002)Dokument21 SeitenPenner, L.A. (2002)noormieyNoch keine Bewertungen
- Experiences, Post Trip Destination EtcDokument10 SeitenExperiences, Post Trip Destination EtcJohn GeorgeNoch keine Bewertungen
- Consumer Behavior On Dell LaptopDokument35 SeitenConsumer Behavior On Dell LaptopNazmul Amin Aqib100% (7)