Das könnte Ihnen auch gefallen
- 04-The Cardiac Cycle - Wigger's Diagram (J Swanevelder)Dokument6 Seiten04-The Cardiac Cycle - Wigger's Diagram (J Swanevelder)Patrick WilliamsNoch keine Bewertungen
- The Cardiac CycleDokument19 SeitenThe Cardiac CycleRebi NesroNoch keine Bewertungen
- Cardiac Cycle: DR Rida Ajmal KhanDokument29 SeitenCardiac Cycle: DR Rida Ajmal KhanMooma fatimaNoch keine Bewertungen
- Cardiac CycleDokument31 SeitenCardiac CycleAdwaitha KrNoch keine Bewertungen
- Lecture On Cardiac Cycle by DR RoomiDokument43 SeitenLecture On Cardiac Cycle by DR RoomiMudassar Roomi100% (2)
- PC Cardiac CycleDokument29 SeitenPC Cardiac CycleSebontu HasenNoch keine Bewertungen
- ACUTE CHEST PAIN Normal Cardiac Cycle ExplainedDokument11 SeitenACUTE CHEST PAIN Normal Cardiac Cycle ExplainedShampa SenNoch keine Bewertungen
- Acute Severe Chest Pain: Presented By: Arwa H. Al-OnayzanDokument11 SeitenAcute Severe Chest Pain: Presented By: Arwa H. Al-OnayzanShampa SenNoch keine Bewertungen
- Electrical Conduction in The HeartDokument35 SeitenElectrical Conduction in The HeartNormasnizam Mohd NoorNoch keine Bewertungen
- Cardiac Physiology PDFDokument17 SeitenCardiac Physiology PDFAli Aborges Jr.Noch keine Bewertungen
- Cardiac Cycle Phases ExplainedDokument27 SeitenCardiac Cycle Phases ExplainedThird Year B PharmNoch keine Bewertungen
- Cardiac CycleDokument30 SeitenCardiac CycleAdel100% (1)
- Cardiac CycleDokument38 SeitenCardiac CycleKok HoongNoch keine Bewertungen
- K3 - CardiacCycle and Heart Sound Physiology-Cv13Dokument40 SeitenK3 - CardiacCycle and Heart Sound Physiology-Cv13Raka Notgoing Anywherebut AlwayseverywhereNoch keine Bewertungen
- Cvs PPT 2) BpehssDokument35 SeitenCvs PPT 2) BpehssAmbreen GhafoorNoch keine Bewertungen
- Cardiovascular Physiology: Lawrence A. Olatunji ReaderDokument46 SeitenCardiovascular Physiology: Lawrence A. Olatunji ReaderMaryam Ogunade0% (1)
- The Cardiac CycleDokument9 SeitenThe Cardiac CycleKaylababy Hamilton BlackNoch keine Bewertungen
- Study FastDokument49 SeitenStudy FastmbbsporalekhaNoch keine Bewertungen
- Cardiac Cycle CardiodynamicsDokument29 SeitenCardiac Cycle Cardiodynamicseverforyou2023Noch keine Bewertungen
- TtttttygbhbDokument4 SeitenTtttttygbhbNeeraj JainNoch keine Bewertungen
- KP 1.3.2.1 Aktivitas Mekanik Jantung (2 Jam)Dokument68 SeitenKP 1.3.2.1 Aktivitas Mekanik Jantung (2 Jam)Try MutiaraNoch keine Bewertungen
- Cardiac Cycle: The Events of the HeartbeatDokument37 SeitenCardiac Cycle: The Events of the Heartbeatindra_jeet2009Noch keine Bewertungen
- Cardiac Cycle Events & PhasesDokument12 SeitenCardiac Cycle Events & Phasesanupam manu100% (1)
- Circulatory SystemDokument304 SeitenCirculatory Systemyapyihao2100% (1)
- Cardiac CycleDokument30 SeitenCardiac CycleCarrine Liew100% (2)
- Cardiac CycleDokument5 SeitenCardiac Cyclen_nkNoch keine Bewertungen
- Cardiac Cycle - WikipediaDokument13 SeitenCardiac Cycle - WikipediaHarshal GaikwadNoch keine Bewertungen
- Cardiac Cycle - Atrial Contraction (Phase 1) : A-V Valves Open Semilunar Valves ClosedDokument10 SeitenCardiac Cycle - Atrial Contraction (Phase 1) : A-V Valves Open Semilunar Valves ClosedFatima KhanNoch keine Bewertungen
- The Cardiac Cycle ExplainedDokument18 SeitenThe Cardiac Cycle ExplainedKundan GuptaNoch keine Bewertungen
- Cardiac CycleDokument4 SeitenCardiac CycleDivya RanasariaNoch keine Bewertungen
- Jantung Sebagai PompaDokument54 SeitenJantung Sebagai PompaIndraYudhiNoch keine Bewertungen
- Cardiac Cycle - Day 4Dokument10 SeitenCardiac Cycle - Day 4PKCHRYAHOO.COMNoch keine Bewertungen
- Cardiac Cycle - Atrial Contraction (Phase 1)Dokument10 SeitenCardiac Cycle - Atrial Contraction (Phase 1)Fatima KhanNoch keine Bewertungen
- Cardiac Cycle: DR Rakesh JainDokument97 SeitenCardiac Cycle: DR Rakesh JainKemoy FrancisNoch keine Bewertungen
- Cardiac CycleDokument6 SeitenCardiac Cyclearavind kishanNoch keine Bewertungen
- Cardiac Cycle by Dr. RoomiDokument71 SeitenCardiac Cycle by Dr. RoomiMudassar Roomi100% (3)
- CardiovascularPhysiology(1)Dokument55 SeitenCardiovascularPhysiology(1)s8f2dmzdvjNoch keine Bewertungen
- Amboss - Cradiac CycleDokument18 SeitenAmboss - Cradiac CycleAllysahNoch keine Bewertungen
- Physiology of The Cardiac SystemDokument41 SeitenPhysiology of The Cardiac SystemRoh JitenNoch keine Bewertungen
- Heart As A Pump: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraDokument33 SeitenHeart As A Pump: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraXeniel AlastairNoch keine Bewertungen
- Cardiac Cycle StagesDokument19 SeitenCardiac Cycle StagesKhalid AbdullahNoch keine Bewertungen
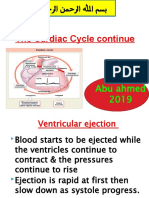
- The Cardiac Cycle Continue: Abu Ahmed 2019Dokument19 SeitenThe Cardiac Cycle Continue: Abu Ahmed 2019Khalid AbdullahNoch keine Bewertungen
- Cardiac Cycle: DR - Lalitha Shanmugam, Professor of Physiology, VMCHDokument56 SeitenCardiac Cycle: DR - Lalitha Shanmugam, Professor of Physiology, VMCHRamakrishnanNoch keine Bewertungen
- CARDIAC CYCLE-laDokument12 SeitenCARDIAC CYCLE-latehillahkabwe100Noch keine Bewertungen
- Cv-4 PHDokument28 SeitenCv-4 PHaya najemNoch keine Bewertungen
- Wiggers Diagram SlidesDokument15 SeitenWiggers Diagram SlidesKuro ShiroNoch keine Bewertungen
- Anatomy and Physiology of The HeartDokument21 SeitenAnatomy and Physiology of The HeartNina OaipNoch keine Bewertungen
- Oral PathologyDokument23 SeitenOral PathologyRuba AbbassNoch keine Bewertungen
- Cardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)Dokument21 SeitenCardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)minesh prajapatiNoch keine Bewertungen
- Cardiovascular PhysiologyDokument88 SeitenCardiovascular Physiologykhorrami4Noch keine Bewertungen
- DR Rahimah Zakaria Dept of PhysiologyDokument31 SeitenDR Rahimah Zakaria Dept of PhysiologyChokJunHoongNoch keine Bewertungen
- Cardiac CycleDokument36 SeitenCardiac Cycleanushkav443Noch keine Bewertungen
- The cardiac cycle 2Dokument7 SeitenThe cardiac cycle 2Abigail ChristisnNoch keine Bewertungen
- 4,5-Cardiac Cycle Team441Dokument29 Seiten4,5-Cardiac Cycle Team441aliusman laseNoch keine Bewertungen
- The Cardiac CycleDokument7 SeitenThe Cardiac CyclePiyush KherdeNoch keine Bewertungen
- Cardiovascular Physiology ExplainedDokument33 SeitenCardiovascular Physiology ExplainedHanaNoch keine Bewertungen
- The Cardiac Cycle ExplainedDokument15 SeitenThe Cardiac Cycle ExplainedNimisha BalakrishnanNoch keine Bewertungen
- The Cardiac Cycle ExplainedDokument15 SeitenThe Cardiac Cycle ExplainedNimisha BalakrishnanNoch keine Bewertungen
- Central Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsVon EverandCentral Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsNoch keine Bewertungen
- Effects of Air PollutionDokument3 SeitenEffects of Air PollutionKhan ArafathNoch keine Bewertungen
- Environmental Pollution and Impacts On Public HealthDokument14 SeitenEnvironmental Pollution and Impacts On Public HealthtexpectationsNoch keine Bewertungen
- Greenhouse Effect and Global WarmingDokument7 SeitenGreenhouse Effect and Global WarmingRajat BansalNoch keine Bewertungen
- Mammography Screening Program Provides Breast Cancer InfoDokument7 SeitenMammography Screening Program Provides Breast Cancer InfoVinuPrakashJ.Noch keine Bewertungen
- CH 6 - The Circulatory System PDFDokument11 SeitenCH 6 - The Circulatory System PDFAnonymous e6LINHNoch keine Bewertungen
- Agarwal and Narain 1991 GLOBAL WARMING IN AN UNEQUAL WORLDDokument36 SeitenAgarwal and Narain 1991 GLOBAL WARMING IN AN UNEQUAL WORLDJyoti NairNoch keine Bewertungen
- Mammography Screening in Switzerland: Limited Evidence From Limited DataDokument13 SeitenMammography Screening in Switzerland: Limited Evidence From Limited DataVinuPrakashJ.Noch keine Bewertungen
- Mce CODokument24 SeitenMce COMieh PacualNoch keine Bewertungen
- Mammograms and Other Breast Imaging Tests: What Is A Mammogram?Dokument26 SeitenMammograms and Other Breast Imaging Tests: What Is A Mammogram?VinuPrakashJ.Noch keine Bewertungen
- What Are Heart Disease and Stroke?Dokument2 SeitenWhat Are Heart Disease and Stroke?VinuPrakashJ.Noch keine Bewertungen
- What Is DiabetesDokument4 SeitenWhat Is DiabetesMarsiano QendroNoch keine Bewertungen
- What Is DiabetesDokument4 SeitenWhat Is DiabetesMarsiano QendroNoch keine Bewertungen
- ProspectusCBCS 2011 12Dokument49 SeitenProspectusCBCS 2011 12mamallandNoch keine Bewertungen
- Botanical NamesDokument6 SeitenBotanical NamesLawal Oluwafemi100% (1)
- Chordee CaseDokument3 SeitenChordee CaseSuhasini GazulaNoch keine Bewertungen
- Xtra Online XS-Series-Sysmex 5-Part Diff Analyser With Fluorescence TechnologyDokument5 SeitenXtra Online XS-Series-Sysmex 5-Part Diff Analyser With Fluorescence TechnologyAhmad MuzakkirNoch keine Bewertungen
- 12 - Paediatric Abdomen RadiologyDokument74 Seiten12 - Paediatric Abdomen RadiologyMaria DoukaNoch keine Bewertungen
- Herbal Vapor Rub for Headache ReliefDokument15 SeitenHerbal Vapor Rub for Headache ReliefHannah Coleen Nacion68% (19)
- Respiratory Distress in NewbornDokument52 SeitenRespiratory Distress in NewbornNadia SalwaniNoch keine Bewertungen
- Cervical ExerciseDokument16 SeitenCervical ExerciseAmit Shukla100% (2)
- Assessment of Mental RetardationDokument56 SeitenAssessment of Mental Retardationdrkadiyala2Noch keine Bewertungen
- Eylea FpiDokument8 SeitenEylea FpiZeptii PriantiNoch keine Bewertungen
- 6 Best Speech Therapy FilmsDokument8 Seiten6 Best Speech Therapy FilmsElisa Nurul LailiNoch keine Bewertungen
- Ulnar Nerve Entrapment Massage Mag Whitney LoweDokument3 SeitenUlnar Nerve Entrapment Massage Mag Whitney Lowewolfgangl70Noch keine Bewertungen
- Best Cardiologist in Pune - Cardiologist in Pune - DR Ajit MehtaDokument10 SeitenBest Cardiologist in Pune - Cardiologist in Pune - DR Ajit MehtaAjit MehtaNoch keine Bewertungen
- Cincinnati Veteran S Administration Medical CenterDokument13 SeitenCincinnati Veteran S Administration Medical CenterRicardo MontesNoch keine Bewertungen
- Reflex HammerDokument1 SeiteReflex HammerManuel Porras-BetancourtNoch keine Bewertungen
- CVSDokument58 SeitenCVSDoina SvetNoch keine Bewertungen
- Alveolar Distraction Osteogenesis ArchWise Appliance and TechniqueDokument132 SeitenAlveolar Distraction Osteogenesis ArchWise Appliance and TechniqueJaneth García ChávezNoch keine Bewertungen
- Peripheral Nerve InjuriesDokument29 SeitenPeripheral Nerve InjuriesbrillniksNoch keine Bewertungen
- Famous Discoveries by Medical StudentsansDokument8 SeitenFamous Discoveries by Medical StudentsansJoao FonsecaNoch keine Bewertungen
- Daftar PustakaDokument2 SeitenDaftar PustakaJalalludin AnNoch keine Bewertungen
- Snell Abdomen Questions AnswersDokument10 SeitenSnell Abdomen Questions AnswersBen67% (9)
- Preventive DentistryDokument14 SeitenPreventive DentistryatikramadhaniNoch keine Bewertungen
- Essential Newborn Care (Enc) & Delivery Room ProtocolsDokument95 SeitenEssential Newborn Care (Enc) & Delivery Room ProtocolsEyySiEffVeeNoch keine Bewertungen
- Spek Vent Vela ComphDokument4 SeitenSpek Vent Vela ComphRinawatiNoch keine Bewertungen
- Replacement Lamp Guide for Medical DevicesDokument16 SeitenReplacement Lamp Guide for Medical DevicesRene Gonzales VasquezNoch keine Bewertungen
- EANM Procedure Guideline For Brain Perfusion SPECT PDFDokument10 SeitenEANM Procedure Guideline For Brain Perfusion SPECT PDFAulia HudaNoch keine Bewertungen
- Treating Multiple Dental Injuries in a Teen Girl After a Car AccidentDokument7 SeitenTreating Multiple Dental Injuries in a Teen Girl After a Car AccidentDiego Andres Hincapie HerreraNoch keine Bewertungen
- Scientific Medical Rationale for Diagnostic Hardware Software Package Intera Vector-BIOPSI-DiaCorDokument10 SeitenScientific Medical Rationale for Diagnostic Hardware Software Package Intera Vector-BIOPSI-DiaCorElena IlioskaNoch keine Bewertungen
- Essentials of Plastic Surgery, 2nd EditionDokument1.351 SeitenEssentials of Plastic Surgery, 2nd EditionIcleanu Alexandru84% (19)
- Stoma CareDokument27 SeitenStoma CareRusida LiyaniNoch keine Bewertungen
- Japanese male medical doctors found to have average life span similar to general populationDokument5 SeitenJapanese male medical doctors found to have average life span similar to general populationfraushaiNoch keine Bewertungen
- The Facial Artery: Course and RelationsDokument9 SeitenThe Facial Artery: Course and Relationsvipul51190Noch keine Bewertungen