Das könnte Ihnen auch gefallen
- Acute Heart Failure and Cardiogenic Shock - 3a A Multidisciplinary Practical GuidanceDokument17 SeitenAcute Heart Failure and Cardiogenic Shock - 3a A Multidisciplinary Practical GuidanceAaron Nureña100% (1)
- Part 9 Acute Coronary SyndromesDokument19 SeitenPart 9 Acute Coronary SyndromesAbid Fuentes NevarezNoch keine Bewertungen
- 030 - EIJ D 23 00749 - GalassiDokument11 Seiten030 - EIJ D 23 00749 - GalassiBagus CarterNoch keine Bewertungen
- Complications of Percutaneous Coronary Intervention: The Survival HandbookVon EverandComplications of Percutaneous Coronary Intervention: The Survival HandbookAlistair LindsayNoch keine Bewertungen
- Acute Ischaemic StrokeDokument40 SeitenAcute Ischaemic StrokeDana Crusoveanu100% (1)
- 2012STEMI治療指引 3Dokument27 Seiten2012STEMI治療指引 3吳任爵Noch keine Bewertungen
- Referat Dysfunction Diastolic and Implication in AnathesiaDokument32 SeitenReferat Dysfunction Diastolic and Implication in AnathesiaRia Raissa FalaNoch keine Bewertungen
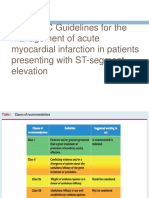
- 2017 ESC Guidelines For The Management of Acute Myocardial Infarction in Patients Presenting With ST-segment ElevationDokument62 Seiten2017 ESC Guidelines For The Management of Acute Myocardial Infarction in Patients Presenting With ST-segment ElevationNurcahyaKuswardhanaNoch keine Bewertungen
- Essential Messages - 2023 ACSDokument16 SeitenEssential Messages - 2023 ACSimran karimNoch keine Bewertungen
- RRC Art-2Dokument16 SeitenRRC Art-2TanyaDonciuNoch keine Bewertungen
- Biomarker-Based Preoperative Risk Stratification For Patients Undergoing Non-Cardiac Surgery - Yurttas Et Al 2020Dokument10 SeitenBiomarker-Based Preoperative Risk Stratification For Patients Undergoing Non-Cardiac Surgery - Yurttas Et Al 2020santosfer1102Noch keine Bewertungen
- Consensus Antithrombotic Therapy in AF in Patients With Acute Coronary Syndrome and Undergoing Percutaneous Coronary or Valve InterventionsDokument25 SeitenConsensus Antithrombotic Therapy in AF in Patients With Acute Coronary Syndrome and Undergoing Percutaneous Coronary or Valve InterventionsChalikias GeorgeNoch keine Bewertungen
- EHJ-triple-therapy DAPTDokument25 SeitenEHJ-triple-therapy DAPTmlinaballerinaNoch keine Bewertungen
- Positionpaper wg27 82kb-1 PDFDokument8 SeitenPositionpaper wg27 82kb-1 PDFYan BaseriNoch keine Bewertungen
- Guidelines For The Diagnosis, Treatment and Prevention of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2009)Dokument24 SeitenGuidelines For The Diagnosis, Treatment and Prevention of Pulmonary Embolism and Deep Vein Thrombosis (JSC 2009)Carlos JohnsonNoch keine Bewertungen
- Resusitasi AnastesiDokument15 SeitenResusitasi AnastesiFannia ReynathaNoch keine Bewertungen
- Recommendation On ICU DesignDokument7 SeitenRecommendation On ICU DesignIhab Sadek FaekNoch keine Bewertungen
- Adult Advanced Life Support GuidelinesDokument11 SeitenAdult Advanced Life Support GuidelinesRuvan AmarasingheNoch keine Bewertungen
- Adult Advanced Life Support GuidelinesDokument11 SeitenAdult Advanced Life Support Guidelinesrutba.ahmkhanNoch keine Bewertungen
- Buku CHFDokument59 SeitenBuku CHFSylvia PertiwiNoch keine Bewertungen
- Case Series - Acute Coronary SyndromeDokument18 SeitenCase Series - Acute Coronary SyndromenikNoch keine Bewertungen
- Adult Advanced Life Support GuidelinesDokument11 SeitenAdult Advanced Life Support GuidelinesDellaneira SetjiadiNoch keine Bewertungen
- Accepted Manuscript: Current Problems in CardiologyDokument17 SeitenAccepted Manuscript: Current Problems in CardiologyAldo González SalinasNoch keine Bewertungen
- Adult Cardiac Surgery - Nursing Care and ManagementDokument225 SeitenAdult Cardiac Surgery - Nursing Care and ManagementOsama Elsayed AhmedNoch keine Bewertungen
- Abel Wakai Diagnosis and Management of Patients WithDokument2 SeitenAbel Wakai Diagnosis and Management of Patients WithJuliaNoch keine Bewertungen
- TX Iskemik StrokeDokument17 SeitenTX Iskemik StrokeNailis Sa'adahNoch keine Bewertungen
- NZRC - All Adult Advanced Life Support Guidelines3Dokument79 SeitenNZRC - All Adult Advanced Life Support Guidelines3stanwalksNoch keine Bewertungen
- S0300 9572 (15) 00329 9 - MainDokument54 SeitenS0300 9572 (15) 00329 9 - MaintugurlanNoch keine Bewertungen
- Review Articles: Medical ProgressDokument10 SeitenReview Articles: Medical ProgressMiko AkmarozaNoch keine Bewertungen
- Antonio Landi Antithrombotic Therapy in Patients WithDokument8 SeitenAntonio Landi Antithrombotic Therapy in Patients WithAdriLuz AlphaNoch keine Bewertungen
- Cardiac Arrest in The Operating Room (2012)Dokument6 SeitenCardiac Arrest in The Operating Room (2012)patricia.untoroNoch keine Bewertungen
- Acute Myocardial Infarction: Primary Angioplasty: Coronary DiseaseDokument5 SeitenAcute Myocardial Infarction: Primary Angioplasty: Coronary DiseaseGuțu SergheiNoch keine Bewertungen
- Chest Pain Units (Issue of Cardiology Clinics Journal) - M. Crawford, Ed., (Elsevier, 2005) WWDokument215 SeitenChest Pain Units (Issue of Cardiology Clinics Journal) - M. Crawford, Ed., (Elsevier, 2005) WWRomeo-Remus RaffaiNoch keine Bewertungen
- NON CARDIAC SURGERY. ESC POCKET GLS.2022. Larger FontDokument63 SeitenNON CARDIAC SURGERY. ESC POCKET GLS.2022. Larger FontGeoNoch keine Bewertungen
- ESC GUIDELINES SUMMARY on heart failure, atrial fibrillation, dyslipidaemia and cardiovascular preventionDokument11 SeitenESC GUIDELINES SUMMARY on heart failure, atrial fibrillation, dyslipidaemia and cardiovascular preventionNick StamatiadisNoch keine Bewertungen
- Cardiology GuidelineDokument8 SeitenCardiology GuidelineIboy ZulhamNoch keine Bewertungen
- 2022 Non-Cardiac SurgeryDokument105 Seiten2022 Non-Cardiac Surgeryhosameldin ahmedNoch keine Bewertungen
- CPG Unstable AnginaDokument58 SeitenCPG Unstable AnginaAmir HassenNoch keine Bewertungen
- Vascular Surgery: Current QuestionsVon EverandVascular Surgery: Current QuestionsAires A. B. Barros D'SaBewertung: 5 von 5 Sternen5/5 (1)
- Peri-Arrest Arrhythmias: AuthorsDokument11 SeitenPeri-Arrest Arrhythmias: AuthorsMohammadAbdurRahmanNoch keine Bewertungen
- Los 10 Mandamientos Del Síndrome Coronario Agudo SEC 2023Dokument3 SeitenLos 10 Mandamientos Del Síndrome Coronario Agudo SEC 2023Yaneth FernandezNoch keine Bewertungen
- Effect of Implementing Clinical Pathway Guidelines On Patients' Clinical Outcomes With Acute Coronary SyndromeDokument17 SeitenEffect of Implementing Clinical Pathway Guidelines On Patients' Clinical Outcomes With Acute Coronary SyndromenurulfahmiNoch keine Bewertungen
- Arc Guideline 11 1 Introduction To and Principles of in Hospital Resuscitation Feb 2019Dokument22 SeitenArc Guideline 11 1 Introduction To and Principles of in Hospital Resuscitation Feb 2019hernandez2812Noch keine Bewertungen
- Essential Messages - 2023 CMDokument14 SeitenEssential Messages - 2023 CMimran karimNoch keine Bewertungen
- QR Management of Ischaemic Stroke 3rd Edition 2020 v20210228Dokument25 SeitenQR Management of Ischaemic Stroke 3rd Edition 2020 v20210228Jye yiNoch keine Bewertungen
- Emergency Neurological Life Support: Resuscitation Following Cardiac ArrestDokument27 SeitenEmergency Neurological Life Support: Resuscitation Following Cardiac ArrestElisabeth Permatasari SidabutarNoch keine Bewertungen
- Diagnosis and Risk Stratification of Chest Pain Patients in The Emergency Department: Focus On Acute Coronary Syndromes. A Position Paper of The Acute Cardiovascular Care AssociationDokument14 SeitenDiagnosis and Risk Stratification of Chest Pain Patients in The Emergency Department: Focus On Acute Coronary Syndromes. A Position Paper of The Acute Cardiovascular Care AssociationAngela OrozcoNoch keine Bewertungen
- Anesthesiology Centric ACLSDokument45 SeitenAnesthesiology Centric ACLSAlex ApsokardosNoch keine Bewertungen
- (26770164 - Imaging) Echocardiography in The Intensive Care Unit: An Essential Tool For Diagnosis, Monitoring and Guiding Clinical Decision-MakingDokument15 Seiten(26770164 - Imaging) Echocardiography in The Intensive Care Unit: An Essential Tool For Diagnosis, Monitoring and Guiding Clinical Decision-MakingCamilo GomezNoch keine Bewertungen
- Warfarin Och PCI-guidelinesDokument10 SeitenWarfarin Och PCI-guidelinesdoctormussieaberraNoch keine Bewertungen
- Pharmacotherapy of Non ST-elevation ACS (Adel Khalil Assignment)Dokument30 SeitenPharmacotherapy of Non ST-elevation ACS (Adel Khalil Assignment)عادل خليلNoch keine Bewertungen
- Manual of STEMI InterventionsVon EverandManual of STEMI InterventionsSameer MehtaNoch keine Bewertungen
- What Is Extracorporeal Cardiopulmonary Resuscitation?: Federico Pappalardo, Andrea MontisciDokument5 SeitenWhat Is Extracorporeal Cardiopulmonary Resuscitation?: Federico Pappalardo, Andrea MontisciPrajogo KusumaNoch keine Bewertungen
- Safety and Health Status Following Early Discharge in Patients With Acute Myocardial Infarction Treated With Primary PCI: A Randomized TrialDokument8 SeitenSafety and Health Status Following Early Discharge in Patients With Acute Myocardial Infarction Treated With Primary PCI: A Randomized TrialsarahNoch keine Bewertungen
- Syncope Update 2013: Diagnosis and Treatment: Piotr KułakowskiDokument9 SeitenSyncope Update 2013: Diagnosis and Treatment: Piotr KułakowskichandanNoch keine Bewertungen
- MINOCA Agewall 2017Dokument11 SeitenMINOCA Agewall 2017mate ellaNoch keine Bewertungen
- From Acute Heart Failure To Cardiogenic Shock Patients Requiring Admission, 2023Dokument2 SeitenFrom Acute Heart Failure To Cardiogenic Shock Patients Requiring Admission, 2023Jonathan Fierro MedinaNoch keine Bewertungen
- Guidelines for thrombolysis in STEMIDokument25 SeitenGuidelines for thrombolysis in STEMIrranindyaprabasaryNoch keine Bewertungen
- Morning Report SummaryDokument27 SeitenMorning Report SummaryFerdinando BaehaNoch keine Bewertungen
- Morning Report SummaryDokument27 SeitenMorning Report SummaryFerdinando BaehaNoch keine Bewertungen
- Timeline Lomba Dekan Cup 2019 NewDokument5 SeitenTimeline Lomba Dekan Cup 2019 NewFerdinando BaehaNoch keine Bewertungen
- Hypocalcemia, Hypoparathyroid WahyuDokument4 SeitenHypocalcemia, Hypoparathyroid WahyuFerdinando BaehaNoch keine Bewertungen
- RHDDokument130 SeitenRHDDeepu RajendranNoch keine Bewertungen
- Very Important!! Share 133Dokument20 SeitenVery Important!! Share 133Ferdinando BaehaNoch keine Bewertungen
- Hiperbilrubin AapDokument17 SeitenHiperbilrubin AapMochammad Ridwan CsrNoch keine Bewertungen
- Very Important!! Share 133Dokument20 SeitenVery Important!! Share 133Ferdinando BaehaNoch keine Bewertungen
- Chart Pertumbuhan AnakDokument1 SeiteChart Pertumbuhan AnakWahyudi Pratama HarliNoch keine Bewertungen
- Therapeutic Applications of Citicoline and Piracetam As Fixed Dose CombinationDokument6 SeitenTherapeutic Applications of Citicoline and Piracetam As Fixed Dose CombinationFerdinando BaehaNoch keine Bewertungen
- WHO Growth Chart Boys (Weight For Age) 0-5 YearsDokument1 SeiteWHO Growth Chart Boys (Weight For Age) 0-5 YearsHendry HuangNoch keine Bewertungen
- Algoritma BradycardiaDokument1 SeiteAlgoritma BradycardiaFiya SahrulNoch keine Bewertungen
- Ocular Shape and Myopia: Review ArticleDokument9 SeitenOcular Shape and Myopia: Review ArticleFerdinando BaehaNoch keine Bewertungen
- Yanoff DukerDokument8 SeitenYanoff DukerFerdinando BaehaNoch keine Bewertungen
- 2 PDFDokument3 Seiten2 PDFFerdinando BaehaNoch keine Bewertungen
- Degenerative MyopiaDokument49 SeitenDegenerative MyopiaSekar CiptaningrumNoch keine Bewertungen
- Manifestasi Klinis dan Etiologi Sindrom Koroner AkutDokument4 SeitenManifestasi Klinis dan Etiologi Sindrom Koroner AkutFerdinando BaehaNoch keine Bewertungen
- Myopic Degeneration - Myopic CrescentsDokument3 SeitenMyopic Degeneration - Myopic CrescentsFerdinando BaehaNoch keine Bewertungen
- CLM 12118Dokument8 SeitenCLM 12118Ferdinando BaehaNoch keine Bewertungen
- CLM 12118Dokument8 SeitenCLM 12118Ferdinando BaehaNoch keine Bewertungen
- Coo Endophthalmitis Post-Op v9 Sept11Dokument2 SeitenCoo Endophthalmitis Post-Op v9 Sept11Ferdinando BaehaNoch keine Bewertungen
- Article 6Dokument8 SeitenArticle 6Ferdinando BaehaNoch keine Bewertungen
- Measles in HIV Infection Children FIXDokument51 SeitenMeasles in HIV Infection Children FIXFerdinando BaehaNoch keine Bewertungen
- Yanoff DukerDokument8 SeitenYanoff DukerFerdinando BaehaNoch keine Bewertungen
- 2 PDFDokument3 Seiten2 PDFFerdinando BaehaNoch keine Bewertungen
- Clinical Features of Medical PneumomediastinumDokument4 SeitenClinical Features of Medical PneumomediastinumFerdinando BaehaNoch keine Bewertungen
- K-33 Endocrine System, FK Usu, RevDokument39 SeitenK-33 Endocrine System, FK Usu, RevFerdinando BaehaNoch keine Bewertungen
- Pathology revision with MCQs and case studiesDokument4 SeitenPathology revision with MCQs and case studiesRiyaduNoch keine Bewertungen
- What Is Coronavirus? The Different Types of CoronavirusesDokument9 SeitenWhat Is Coronavirus? The Different Types of Coronavirusesashley bendanaNoch keine Bewertungen
- #04 WN Ms Sheila Cartwright Case Notes Unstable Diabetes MellitusDokument2 Seiten#04 WN Ms Sheila Cartwright Case Notes Unstable Diabetes MellitusNurse OetNoch keine Bewertungen
- Antibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHDokument5 SeitenAntibiotic Susceptibility Patterns of Methicillin Resistant Staphyl - PDF NIHzia ul RahmanNoch keine Bewertungen
- Early Diagnosis of NeoplasisDokument25 SeitenEarly Diagnosis of NeoplasisDanielaNoch keine Bewertungen
- Babesia MicrotiDokument9 SeitenBabesia MicrotiFrancene Ac-DaNoch keine Bewertungen
- Body Art Consent and Health Disclosure Form For Tattooing and PiercingDokument1 SeiteBody Art Consent and Health Disclosure Form For Tattooing and PiercingDanielNoch keine Bewertungen
- Par QPlus 2022Dokument7 SeitenPar QPlus 2022MARIKA BALONDONoch keine Bewertungen
- Presented by Amir Sadaula BVSC & Ah, 8 Sem Rampur Campus Roll No: 01Dokument19 SeitenPresented by Amir Sadaula BVSC & Ah, 8 Sem Rampur Campus Roll No: 01naturalamirNoch keine Bewertungen
- CDC 1st Quar. REPORT 2015Dokument67 SeitenCDC 1st Quar. REPORT 2015abdi qanoNoch keine Bewertungen
- Nursing Care Plan - Acute Pain Related To Surgical IncisionDokument2 SeitenNursing Care Plan - Acute Pain Related To Surgical IncisionCamilogs80% (10)
- Nursing Care Plan For Pressure UlcerDokument4 SeitenNursing Care Plan For Pressure UlcerJobelle Acena50% (2)
- Jama Woo 2021 Oi 210106 1635192380.82276Dokument8 SeitenJama Woo 2021 Oi 210106 1635192380.82276Melissa GuerreroNoch keine Bewertungen
- Case Study Htm400Dokument6 SeitenCase Study Htm400maizatul rosniNoch keine Bewertungen
- NMC LICENSURE - Care PlanDokument2 SeitenNMC LICENSURE - Care PlanAlukuba AwalNoch keine Bewertungen
- Periodontal Disease and Its Impact On Health FromDokument9 SeitenPeriodontal Disease and Its Impact On Health FromLisbethNoch keine Bewertungen
- TorchesDokument23 SeitenTorchesErrold Joseph LahaganNoch keine Bewertungen
- Biology Cbse Class 12th Investigatory ProjectDokument33 SeitenBiology Cbse Class 12th Investigatory ProjectRajesh BiswalNoch keine Bewertungen
- Case Study BlepharitisDokument12 SeitenCase Study BlepharitisNorshahidah IedaNoch keine Bewertungen
- COURSE TITLE - NCM 113Dokument40 SeitenCOURSE TITLE - NCM 113Geevee Naganag VentulaNoch keine Bewertungen
- Amicus of ADHSDokument35 SeitenAmicus of ADHScronkitenewsNoch keine Bewertungen
- FOUL!! Swine Flu: It's Not What You ThinkDokument85 SeitenFOUL!! Swine Flu: It's Not What You ThinkDonna100% (2)
- Speci C Protein Analysis System: DiagnosticsDokument2 SeitenSpeci C Protein Analysis System: DiagnosticsAniket dubeyNoch keine Bewertungen
- Register Kunjungan Pasien BPJSDokument7 SeitenRegister Kunjungan Pasien BPJSLuLu Ika RizkikaNoch keine Bewertungen
- Daftar PustakaDokument2 SeitenDaftar PustakatiarNoch keine Bewertungen
- Unconscious: By: Simranpreet KaurDokument12 SeitenUnconscious: By: Simranpreet Kaurpreet kaurNoch keine Bewertungen
- A Case Report On Delusional ParasitosisDokument3 SeitenA Case Report On Delusional ParasitosisIJAR JOURNALNoch keine Bewertungen
- Series of 2021: Interim NITAG For COVID-19 Vaccine 1 Resolution No. 2 S. 2021Dokument7 SeitenSeries of 2021: Interim NITAG For COVID-19 Vaccine 1 Resolution No. 2 S. 2021Marky OlorvidaNoch keine Bewertungen
- Live Experiences of OFW Seafarers Covid Survivors This PandemicDokument5 SeitenLive Experiences of OFW Seafarers Covid Survivors This PandemicParong, AallyjahNoch keine Bewertungen
- Chapoco - Course Task - NCPDokument1 SeiteChapoco - Course Task - NCPsofia yapNoch keine Bewertungen