Das könnte Ihnen auch gefallen
- Red Cell Morphology in Peripheral Smear and Automated Counter 2019 PDFDokument6 SeitenRed Cell Morphology in Peripheral Smear and Automated Counter 2019 PDFtufis02Noch keine Bewertungen
- Abnormal WBC Scattergram A Clue To The Diagnosis of MalariaDokument6 SeitenAbnormal WBC Scattergram A Clue To The Diagnosis of Malariatufis02Noch keine Bewertungen
- Utility - of - Scatterplot - Patterns - of - Automated - Hematology Analysers 2020Dokument6 SeitenUtility - of - Scatterplot - Patterns - of - Automated - Hematology Analysers 2020tufis02Noch keine Bewertungen
- Interpretation-Of-Histograms PresentationDokument46 SeitenInterpretation-Of-Histograms Presentationtufis02Noch keine Bewertungen
- A Specific Abnormal Scattergram of Peripheral Blood Leukocytes That May Suggest Hairy Cell LeukemiaDokument4 SeitenA Specific Abnormal Scattergram of Peripheral Blood Leukocytes That May Suggest Hairy Cell Leukemiatufis02Noch keine Bewertungen
- XN Training ManualDokument135 SeitenXN Training Manualtufis02100% (2)
- Hematology Discussion 2011 KPBDokument10 SeitenHematology Discussion 2011 KPBtufis02Noch keine Bewertungen
- Reticulated Platelets - Clinical Application and FDokument13 SeitenReticulated Platelets - Clinical Application and Ftufis02Noch keine Bewertungen
- Serous Effusions 2018Dokument303 SeitenSerous Effusions 2018tufis02Noch keine Bewertungen
- Hiperfibrinogenoliza Path-Upmc-Edu-Cases-Case264-Dx-HtmlDokument1 SeiteHiperfibrinogenoliza Path-Upmc-Edu-Cases-Case264-Dx-Htmltufis02Noch keine Bewertungen
- Dan Matei Abandoned Forts and Their Civi PDFDokument19 SeitenDan Matei Abandoned Forts and Their Civi PDFtufis02Noch keine Bewertungen
- Open or Close BOOKMARKS - : Ken Grauer, MD-KG/EKG Press (Gainesville, FL 600 Pages - 2014)Dokument15 SeitenOpen or Close BOOKMARKS - : Ken Grauer, MD-KG/EKG Press (Gainesville, FL 600 Pages - 2014)tufis02Noch keine Bewertungen
- Peripheral Smear Examination PDFDokument91 SeitenPeripheral Smear Examination PDFtufis02Noch keine Bewertungen
- Learning The Nodal Stations in The AbdomenDokument9 SeitenLearning The Nodal Stations in The Abdomentufis02Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 10 General Anatomy of The Cardiovascular SystemDokument140 Seiten10 General Anatomy of The Cardiovascular SystemSuzana VoiculescuNoch keine Bewertungen
- Betarie Anum Almira - RMIK (A) - Praktik KSPK 11Dokument1 SeiteBetarie Anum Almira - RMIK (A) - Praktik KSPK 11Betarie Anum AlmiraNoch keine Bewertungen
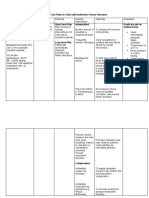
- NCP Preeclampsia and EclampsiaDokument16 SeitenNCP Preeclampsia and EclampsiaBiway Regala100% (1)
- JURNAL Diseksi AortaDokument3 SeitenJURNAL Diseksi AortaNurhidayantiAyaMSNoch keine Bewertungen
- Cardiomyopathy KonoDokument150 SeitenCardiomyopathy KonoValerian BîcosNoch keine Bewertungen
- Acute Myocardial Infarction Pa Tho Physiology Amp Schematic DiagramDokument6 SeitenAcute Myocardial Infarction Pa Tho Physiology Amp Schematic DiagramPeArl PeraltaNoch keine Bewertungen
- WBI11 01 Que 20220108Dokument28 SeitenWBI11 01 Que 20220108Hammodshan 7Noch keine Bewertungen
- Blood Supply of The Neck and HeadDokument56 SeitenBlood Supply of The Neck and HeadAdrianaNoch keine Bewertungen
- Cardiac Arrest: Signs and SymptomsDokument7 SeitenCardiac Arrest: Signs and SymptomsWebster The-TechGuy LunguNoch keine Bewertungen
- Data - Second Annual Data Science Bowl - KaggleDokument3 SeitenData - Second Annual Data Science Bowl - KaggleRVPNoch keine Bewertungen
- Umbilical Catheterization in ServiceDokument11 SeitenUmbilical Catheterization in ServiceLucian CaelumNoch keine Bewertungen
- Bloodpressure 2Dokument4 SeitenBloodpressure 2Yousuf Azhar AlamiaNoch keine Bewertungen
- Practical Checklist PD CVS OnlyDokument6 SeitenPractical Checklist PD CVS OnlyardiandawoodNoch keine Bewertungen
- Peran Perawat Pada Pemeriksaan Penunjang IVUS, OCT (Imaging)Dokument31 SeitenPeran Perawat Pada Pemeriksaan Penunjang IVUS, OCT (Imaging)Miftahul HudaNoch keine Bewertungen
- 2014-Brochure LeaderflexDokument2 Seiten2014-Brochure LeaderflexRaji VeeramalluNoch keine Bewertungen
- Blood Pressure ChartDokument5 SeitenBlood Pressure Chartmahajan1963100% (1)
- Ten Questions ICU Specialists Should Address When Managing Cardiogenic Acute Pulmonary OedemaDokument4 SeitenTen Questions ICU Specialists Should Address When Managing Cardiogenic Acute Pulmonary OedemaFarmacia Del Bosque100% (1)
- Circulatory SystemDokument49 SeitenCirculatory SystemBrent ValdespinaNoch keine Bewertungen
- Lymphatic System 2Dokument31 SeitenLymphatic System 2cardos cherryNoch keine Bewertungen
- Electrocardiogram: Dr. Yasser El-WazirDokument21 SeitenElectrocardiogram: Dr. Yasser El-WazirSalah Salah 201-901-341Noch keine Bewertungen
- Chest Pain Protocol in EDDokument3 SeitenChest Pain Protocol in EDshahidchaudharyNoch keine Bewertungen
- Pediatric Nursing Reviewer CardiovascularDokument4 SeitenPediatric Nursing Reviewer CardiovascularJemy Lorane TemporalNoch keine Bewertungen
- Heart Failure LCDokument14 SeitenHeart Failure LCgalih suharnoNoch keine Bewertungen
- Vitamin E Book For Ailing and Healthy Hearts - Wilfrid Shute PDF (Orthomolecular Medicine)Dokument212 SeitenVitamin E Book For Ailing and Healthy Hearts - Wilfrid Shute PDF (Orthomolecular Medicine)Anonymous gwFqQcnaX80% (5)
- Journal Coartation AortaDokument6 SeitenJournal Coartation AortaMangaismeNoch keine Bewertungen
- RBSE Class 8 Science Notes Chapter 7 Blood Circulation - RBSE GuideDokument3 SeitenRBSE Class 8 Science Notes Chapter 7 Blood Circulation - RBSE GuideAlpine AcademiaNoch keine Bewertungen
- Structured Oral Examination in Clinical Anaesthesia Practice Ex NDokument578 SeitenStructured Oral Examination in Clinical Anaesthesia Practice Ex Nkaran27091% (11)
- Nursing Care Plan For Client With Ineffective Tissue PerfusionDokument2 SeitenNursing Care Plan For Client With Ineffective Tissue PerfusionThe Right WayNoch keine Bewertungen
- Path-09 CARDIODokument18 SeitenPath-09 CARDIOCarlos Fernando Banegas FloresNoch keine Bewertungen
- Easy Rhythm Strip AnalysisDokument24 SeitenEasy Rhythm Strip Analysisheldai1100% (4)