Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Extended Techniques Resource PageDokument9 SeitenExtended Techniques Resource PageRubelleMicahCagampangSapongNoch keine Bewertungen
- Copy WriteDokument1 SeiteCopy WriteRubelleMicahCagampangSapongNoch keine Bewertungen
- Crowd SourcingDokument1 SeiteCrowd SourcingRubelleMicahCagampangSapongNoch keine Bewertungen
- Reaction PaperDokument3 SeitenReaction PaperRubelleMicahCagampangSapongNoch keine Bewertungen
- Lets Learn Japanese Basic 1 - Volume 1Dokument110 SeitenLets Learn Japanese Basic 1 - Volume 1Ismail Adha Kesuma94% (32)
- Intra CellularDokument1 SeiteIntra CellularRubelleMicahCagampangSapongNoch keine Bewertungen
- RodriguezDokument2 SeitenRodriguezRubelleMicahCagampangSapongNoch keine Bewertungen
- LarynxDokument17 SeitenLarynxRubelleMicahCagampangSapongNoch keine Bewertungen
- Dentry Travis13Dokument12 SeitenDentry Travis13RubelleMicahCagampangSapongNoch keine Bewertungen
- School Age: By: Rubelle Micah C. Sapong, RNDokument7 SeitenSchool Age: By: Rubelle Micah C. Sapong, RNRubelleMicahCagampangSapongNoch keine Bewertungen
- Illness BehaviorDokument11 SeitenIllness BehaviorRubelleMicahCagampangSapongNoch keine Bewertungen
- Greyling13 PDFDokument14 SeitenGreyling13 PDFRubelleMicahCagampangSapongNoch keine Bewertungen
- RodriguezDokument2 SeitenRodriguezRubelleMicahCagampangSapongNoch keine Bewertungen
- Pa ThoDokument1 SeitePa ThoRubelleMicahCagampangSapongNoch keine Bewertungen
- School Age: By: Rubelle Micah C. Sapong, RNDokument7 SeitenSchool Age: By: Rubelle Micah C. Sapong, RNRubelleMicahCagampangSapongNoch keine Bewertungen
- IntroductionDokument5 SeitenIntroductionRubelleMicahCagampangSapongNoch keine Bewertungen
- DisciplineDokument4 SeitenDisciplineRubelleMicahCagampangSapongNoch keine Bewertungen
- Final Term PaperDokument5 SeitenFinal Term PaperRubelleMicahCagampangSapongNoch keine Bewertungen
- Case AnalyisisDokument10 SeitenCase AnalyisisRubelleMicahCagampangSapongNoch keine Bewertungen
- General ObjectivesDokument1 SeiteGeneral ObjectivesRubelleMicahCagampangSapongNoch keine Bewertungen
- Pathophysiology PneumoniaDokument2 SeitenPathophysiology PneumoniaSheila Mae Escalante67% (3)
- Drug Study Amphotericin B, Meropenem, Furosemide, Ciprofloxacin, Pentoxifylline, Pip-Tazo, Midazolam, VecuroniumDokument12 SeitenDrug Study Amphotericin B, Meropenem, Furosemide, Ciprofloxacin, Pentoxifylline, Pip-Tazo, Midazolam, Vecuroniumpaupaulala100% (4)
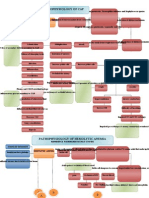
- Pa Tho Physiology Community Aquired Pneumonia and AnemiaDokument3 SeitenPa Tho Physiology Community Aquired Pneumonia and AnemiaRubelleMicahCagampangSapong100% (1)
- Pediatric Assesment Tool: Sakit Jud Siya, Mga 8 Siguro."Dokument5 SeitenPediatric Assesment Tool: Sakit Jud Siya, Mga 8 Siguro."RubelleMicahCagampangSapongNoch keine Bewertungen
- Assessment ToolDokument5 SeitenAssessment ToolRubelleMicahCagampangSapongNoch keine Bewertungen
- Pediatric Assesment Tool: Sakit Jud Siya, Mga 8 Siguro."Dokument5 SeitenPediatric Assesment Tool: Sakit Jud Siya, Mga 8 Siguro."RubelleMicahCagampangSapongNoch keine Bewertungen
- Diabetes MellitusDokument1 SeiteDiabetes MellitusRubelleMicahCagampangSapongNoch keine Bewertungen
- Assessment ToolDokument5 SeitenAssessment ToolRubelleMicahCagampangSapongNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 03 9609 12 MS Prov Rma 08022023111718Dokument18 Seiten03 9609 12 MS Prov Rma 08022023111718Kalsoom SoniNoch keine Bewertungen
- Sandy Ishikawa DiagramDokument24 SeitenSandy Ishikawa DiagramjammusandyNoch keine Bewertungen
- Lesson 2 Cultural Relativism - Part 1 (Reaction Paper)Dokument2 SeitenLesson 2 Cultural Relativism - Part 1 (Reaction Paper)Bai Zaida Abid100% (1)
- Project Report On Reliance TrendsDokument91 SeitenProject Report On Reliance TrendsSubash Tej T50% (4)
- Contract ManagementDokument26 SeitenContract ManagementGK TiwariNoch keine Bewertungen
- Streetcar - A Modern TradegyDokument4 SeitenStreetcar - A Modern Tradegyel spasser100% (2)
- Aarvee Denim & Export LTD.: CertificateDokument46 SeitenAarvee Denim & Export LTD.: CertificateVinita AgrawalNoch keine Bewertungen
- The Hollow ManDokument13 SeitenThe Hollow ManAya ArmandoNoch keine Bewertungen
- Power Semiconductor DevicesDokument11 SeitenPower Semiconductor DevicesBhavesh Kaushal100% (1)
- INTRODUCTION TO PROGRAMMING Exam QuestionsDokument30 SeitenINTRODUCTION TO PROGRAMMING Exam Questionshorrett100% (4)
- A Minor Project Report Submitted To Rajiv Gandhi Prodhyogik Vishwavidyalaya, Bhopal Towards Partial Fulfillment For The Award of The Degree ofDokument53 SeitenA Minor Project Report Submitted To Rajiv Gandhi Prodhyogik Vishwavidyalaya, Bhopal Towards Partial Fulfillment For The Award of The Degree ofwahidjaanNoch keine Bewertungen
- Nift B.ftech Gat PaperDokument7 SeitenNift B.ftech Gat PapergoelNoch keine Bewertungen
- Sampling TechniquesDokument96 SeitenSampling Techniquessixteen liquidoNoch keine Bewertungen
- Fossils (DK Smithsonian Handbook) by DKDokument320 SeitenFossils (DK Smithsonian Handbook) by DKAnthony Mello71% (7)
- Scientific Writing VerbsDokument3 SeitenScientific Writing VerbsNejdetEXn100% (1)
- Daily Hora ChartDokument2 SeitenDaily Hora ChartkalanemiNoch keine Bewertungen
- HeartCry Magazine Summer 2022 WebsiteDokument29 SeitenHeartCry Magazine Summer 2022 WebsiteefraNoch keine Bewertungen
- 6 Money SupplyDokument6 Seiten6 Money SupplySaroj LamichhaneNoch keine Bewertungen
- Tugas Pak Hendro PoemDokument24 SeitenTugas Pak Hendro PoemLaila LalaNoch keine Bewertungen
- Estimation of Barium From Barium Sulphate GravimetricallyDokument4 SeitenEstimation of Barium From Barium Sulphate GravimetricallyMg H67% (15)
- Meditation Club of RUET Asif EEE 17 PDFDokument2 SeitenMeditation Club of RUET Asif EEE 17 PDFShovonNoch keine Bewertungen
- Lemonade by Jeremy Passion: Song Lyrics and Poetry: Student ChoiceDokument2 SeitenLemonade by Jeremy Passion: Song Lyrics and Poetry: Student Choiceapi-330744576Noch keine Bewertungen
- Dark Enemies by Effie CampbellDokument250 SeitenDark Enemies by Effie Campbellsheenuyadav06080Noch keine Bewertungen
- PERENNIALISMDokument2 SeitenPERENNIALISMDaisy Rose TangonanNoch keine Bewertungen
- Krautkrämer Ultrasonic Transducers: For Flaw Detection and SizingDokument48 SeitenKrautkrämer Ultrasonic Transducers: For Flaw Detection and SizingBahadır Tekin100% (1)
- Professional Ethics in Human ValuesDokument25 SeitenProfessional Ethics in Human Valuesdips03275% (4)
- Estoryang BinisayaDokument27 SeitenEstoryang BinisayaAngel GellaNoch keine Bewertungen
- Energy Management Principles and PracticesDokument102 SeitenEnergy Management Principles and PracticesConnor ReedNoch keine Bewertungen
- Dwnload Full Social Psychology 4th Edition Gilovich Test Bank PDFDokument35 SeitenDwnload Full Social Psychology 4th Edition Gilovich Test Bank PDFalilonghidotardlyq71i7f100% (8)
- Fatwa of Zabiha MeatDokument7 SeitenFatwa of Zabiha MeatKrom JamilNoch keine Bewertungen