Das könnte Ihnen auch gefallen
- Soap Note Mary HailshamDokument1 SeiteSoap Note Mary HailshamAlexanderWarren0% (1)
- Applecare Clinical VerificationDokument1 SeiteApplecare Clinical VerificationAlexanderWarrenNoch keine Bewertungen
- Urgent Care Calendar and ObjectivesDokument3 SeitenUrgent Care Calendar and ObjectivesAlexanderWarrenNoch keine Bewertungen
- Clinical LogsDokument601 SeitenClinical LogsAlexanderWarrenNoch keine Bewertungen
- Primary Care Clinical Verification LogDokument2 SeitenPrimary Care Clinical Verification LogAlexanderWarrenNoch keine Bewertungen
- Conference CertificateDokument1 SeiteConference CertificateAlexanderWarrenNoch keine Bewertungen
- Urgent Care Calendar and ObjectivesDokument2 SeitenUrgent Care Calendar and ObjectivesAlexanderWarrenNoch keine Bewertungen
- Primary Care Calendar and ObjectivesDokument3 SeitenPrimary Care Calendar and ObjectivesAlexanderWarrenNoch keine Bewertungen
- Primary Care Clinical Verification LogDokument2 SeitenPrimary Care Clinical Verification LogAlexanderWarrenNoch keine Bewertungen
- Episodic 2Dokument5 SeitenEpisodic 2AlexanderWarrenNoch keine Bewertungen
- Urgent Care Calendar and ObjectivesDokument2 SeitenUrgent Care Calendar and ObjectivesAlexanderWarrenNoch keine Bewertungen
- Urgent Care Calendar and ObjectivesDokument3 SeitenUrgent Care Calendar and ObjectivesAlexanderWarrenNoch keine Bewertungen
- Georgia SignatureDokument13 SeitenGeorgia SignatureAlexanderWarrenNoch keine Bewertungen
- Episodic 1Dokument6 SeitenEpisodic 1AlexanderWarrenNoch keine Bewertungen
- Applecare Clinical Site EvalDokument2 SeitenApplecare Clinical Site EvalAlexanderWarrenNoch keine Bewertungen
- Conference SummaryDokument6 SeitenConference SummaryAlexanderWarrenNoch keine Bewertungen
- Practicum Episodic 3Dokument2 SeitenPracticum Episodic 3AlexanderWarren100% (1)
- Primary Care Issues Paper CorrectDokument7 SeitenPrimary Care Issues Paper CorrectAlexanderWarrenNoch keine Bewertungen
- Applecare Student EvalDokument2 SeitenApplecare Student EvalAlexanderWarrenNoch keine Bewertungen
- Applecare Objectives ChecklistDokument1 SeiteApplecare Objectives ChecklistAlexanderWarrenNoch keine Bewertungen
- NPI SignatureDokument3 SeitenNPI SignatureAlexanderWarrenNoch keine Bewertungen
- DEA SignatureDokument4 SeitenDEA SignatureAlexanderWarrenNoch keine Bewertungen
- ResponseDokument1 SeiteResponseAlexanderWarrenNoch keine Bewertungen
- Collaborative AgreementDokument3 SeitenCollaborative AgreementAlexanderWarrenNoch keine Bewertungen
- Employee ContractDokument5 SeitenEmployee ContractAlexanderWarrenNoch keine Bewertungen
- Initial DiscussionDokument1 SeiteInitial DiscussionAlexanderWarrenNoch keine Bewertungen
- Final Summary of Clinical Experience PDFDokument2 SeitenFinal Summary of Clinical Experience PDFAlexanderWarrenNoch keine Bewertungen
- Business PlanDokument5 SeitenBusiness PlanAlexanderWarrenNoch keine Bewertungen
- Final Summary of Clinical Experience PDFDokument2 SeitenFinal Summary of Clinical Experience PDFAlexanderWarrenNoch keine Bewertungen
- Midterm Clinical Site EvalDokument2 SeitenMidterm Clinical Site EvalAlexanderWarrenNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Case Study Herniated DiscDokument20 SeitenCase Study Herniated Disctinatin98960% (5)
- Hilde Peplau's Theory of Interpersonal RelationsDokument17 SeitenHilde Peplau's Theory of Interpersonal RelationsRosechelle Baggao Siupan-ElarcoNoch keine Bewertungen
- Acute Liver Failure in PediatricDokument28 SeitenAcute Liver Failure in PediatricLillada Giftie AnuntarumpornNoch keine Bewertungen
- Lucio Gullo - Iperenzimemia pancreatica benigna o sindrome di GulloDokument6 SeitenLucio Gullo - Iperenzimemia pancreatica benigna o sindrome di GullobogdanotiNoch keine Bewertungen
- Essay On Stem CellsDokument4 SeitenEssay On Stem CellsAdrien G. S. WaldNoch keine Bewertungen
- LIFE SKETCH OF DR James Tyler Kent PDFDokument3 SeitenLIFE SKETCH OF DR James Tyler Kent PDFkrsnaprakash8346Noch keine Bewertungen
- Drugs Causing Throm Drugs Causing Thrombocytopenia or Low Platelet CountDokument4 SeitenDrugs Causing Throm Drugs Causing Thrombocytopenia or Low Platelet CountDejan OgnjanovicNoch keine Bewertungen
- Icici Lombard Health Care Insurance Claim FormDokument5 SeitenIcici Lombard Health Care Insurance Claim FormsperoNoch keine Bewertungen
- 4.trigeminal Neuralgia OverviewDokument5 Seiten4.trigeminal Neuralgia OverviewVenkatesan VidhyaNoch keine Bewertungen
- Current Trents and Issues in EducationDokument15 SeitenCurrent Trents and Issues in EducationMohini MasseyNoch keine Bewertungen
- Neurologic Assessment: Chapter OutlineDokument22 SeitenNeurologic Assessment: Chapter Outlinekenthepa100% (1)
- الزمالة المصرية أمراض قلب أطفال كتاب الأنشطةDokument28 Seitenالزمالة المصرية أمراض قلب أطفال كتاب الأنشطةMernaAhmedGhoneimNoch keine Bewertungen
- Radiofrequncy Ablation in Chronic Pain ManagementDokument21 SeitenRadiofrequncy Ablation in Chronic Pain Managementtdiddy41Noch keine Bewertungen
- Concussion Management PlanDokument4 SeitenConcussion Management Planapi-310029510Noch keine Bewertungen
- Arrhythmia (Irregular Heartbeats) Symptoms, Types, and TreatmentDokument5 SeitenArrhythmia (Irregular Heartbeats) Symptoms, Types, and TreatmentCyberMeow100% (1)
- Nursing Case Analysis: Laparoscopic CholecystectomyDokument19 SeitenNursing Case Analysis: Laparoscopic CholecystectomyChristopher MaNoch keine Bewertungen
- Adazet 6fig LN TCMWTDokument13 SeitenAdazet 6fig LN TCMWTSwagath NNoch keine Bewertungen
- Gerontology in CroatiaDokument20 SeitenGerontology in Croatiasirup_girlNoch keine Bewertungen
- DigoxinDokument4 SeitenDigoxinJaessa FelicianoNoch keine Bewertungen
- Low Blood PressureDokument2 SeitenLow Blood PressurebambangNoch keine Bewertungen
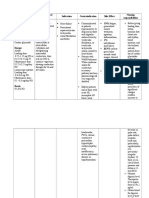
- Drug Study For Acute Renal FailureDokument22 SeitenDrug Study For Acute Renal FailureLhovely ConwiNoch keine Bewertungen
- Family Case AnalysisDokument27 SeitenFamily Case AnalysisEzekiel ArtetaNoch keine Bewertungen
- Schedule AboutDokument13 SeitenSchedule AboutOmkar Joshi100% (1)
- Format English Homework Chapter Four Cardiology Page 29-30Dokument3 SeitenFormat English Homework Chapter Four Cardiology Page 29-30Alvi Jalilul HakimNoch keine Bewertungen
- Steven JohnsonDokument3 SeitenSteven JohnsonJuwandi RahmanNoch keine Bewertungen
- Neonatal TPN: Dr. Fahad Al-AqlDokument10 SeitenNeonatal TPN: Dr. Fahad Al-AqlAnonymous 9dVZCnTXSNoch keine Bewertungen
- Downstate Biotechnology IncubatorDokument2 SeitenDownstate Biotechnology IncubatorJack LynchNoch keine Bewertungen
- Into The Magic Shop - IntroductionDokument4 SeitenInto The Magic Shop - IntroductionSara NemetNoch keine Bewertungen
- CNS DrugsDokument8 SeitenCNS DrugsSheral Aida100% (2)
- FMRI Obs Icu & HduDokument13 SeitenFMRI Obs Icu & HduApoorv JainNoch keine Bewertungen