Das könnte Ihnen auch gefallen
- Daily Vagus Nerve Exercises A Self-Help G - Sherman SanderDokument90 SeitenDaily Vagus Nerve Exercises A Self-Help G - Sherman Sanderscriberone100% (6)
- Stimulate Your Vagus Nerve To Relieve InflammationDokument3 SeitenStimulate Your Vagus Nerve To Relieve Inflammationdocbin100% (3)
- Applied Polyvagal Theory in Yoga - Arielle Schwartz - EbookDokument38 SeitenApplied Polyvagal Theory in Yoga - Arielle Schwartz - EbookSanja Ne Sanja100% (6)
- Marsha Linehan - A Biosocial Developmental Model of Borderline Personality: Elaborating and Extending Linehan's TheoryDokument16 SeitenMarsha Linehan - A Biosocial Developmental Model of Borderline Personality: Elaborating and Extending Linehan's TheoryIrving Pérez MéndezNoch keine Bewertungen
- Stephen Porges Interview Nicabm PDFDokument28 SeitenStephen Porges Interview Nicabm PDFana_vio_94100% (3)
- VBO Bonus Chapter Jodi Cohen 2021Dokument19 SeitenVBO Bonus Chapter Jodi Cohen 2021ioanaNoch keine Bewertungen
- The Heart of Flow PDFDokument72 SeitenThe Heart of Flow PDFBenjamin Rüffin100% (2)
- Porges-2003-The Polyvagal Theory-Phylogenetic Contributions To Social BehaviorDokument11 SeitenPorges-2003-The Polyvagal Theory-Phylogenetic Contributions To Social BehaviorJohn Bakalis100% (1)
- Jodi Cohen Parasympathetic Activation Strategies Updated 2021Dokument31 SeitenJodi Cohen Parasympathetic Activation Strategies Updated 2021Thiago Gueiros100% (1)
- Facilitating Emotional Self Regulation in Preschool ChildrenDokument36 SeitenFacilitating Emotional Self Regulation in Preschool ChildrenIndra Daria100% (2)
- Coronary Artery DiseaseDokument4 SeitenCoronary Artery DiseaseCharles MatabangNoch keine Bewertungen
- The Biology of Aging: The Current Research AgendaDokument10 SeitenThe Biology of Aging: The Current Research Agendagriffone1Noch keine Bewertungen
- Emotion Regulation in Children and AdolescentsDokument14 SeitenEmotion Regulation in Children and AdolescentsRoxana CGhNoch keine Bewertungen
- Yoga Healthy Heart GuideDokument100 SeitenYoga Healthy Heart GuidePralesh12Noch keine Bewertungen
- How To Treat: InsideDokument6 SeitenHow To Treat: InsideAnonymous 4txA8N8etNoch keine Bewertungen
- Sarah Peyton - Attachment NVC Academy 2020Dokument84 SeitenSarah Peyton - Attachment NVC Academy 2020Lucas Moraes100% (2)
- STEPHEN W. PORGES Polyvagal Theory - FullDokument5 SeitenSTEPHEN W. PORGES Polyvagal Theory - FullAugusta AlecsaNoch keine Bewertungen
- Reading Part A Hip FracturesDokument6 SeitenReading Part A Hip Fracturesfernanda1rondelliNoch keine Bewertungen
- Age-Related Anatomic & Physiological Changes: Cardiovascular SystemDokument4 SeitenAge-Related Anatomic & Physiological Changes: Cardiovascular SystemAnonymous AHJFTkI3S5Noch keine Bewertungen
- Trauma GeriatricoDokument13 SeitenTrauma GeriatricoAndreaManceraNoch keine Bewertungen
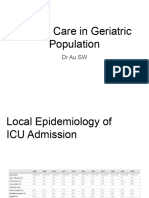
- GeriDokument61 SeitenGeriB AuNoch keine Bewertungen
- Anesthesiaintheelderly Patientundergoing Otolaryngologyheadand NecksurgeryDokument10 SeitenAnesthesiaintheelderly Patientundergoing Otolaryngologyheadand Necksurgeryfabian arassiNoch keine Bewertungen
- Management of Very Old Patient in ICUDokument17 SeitenManagement of Very Old Patient in ICUSuci RahmayenjNoch keine Bewertungen
- Ischemic Stroke in The ElderlyDokument10 SeitenIschemic Stroke in The ElderlysilviaemohNoch keine Bewertungen
- Hipertension en El AncianoDokument11 SeitenHipertension en El AncianoEdgar G RoblesNoch keine Bewertungen
- Corazon EnvejecidoDokument13 SeitenCorazon EnvejecidoAntonio AlonsoNoch keine Bewertungen
- Cardiovascular Risk Factors in The Elderly: Baskent University Cardiology Dept., Ankara, TurkeyDokument23 SeitenCardiovascular Risk Factors in The Elderly: Baskent University Cardiology Dept., Ankara, TurkeyMocanu Cristina-VioricaNoch keine Bewertungen
- AbuelitosDokument38 SeitenAbuelitosMariana VGNoch keine Bewertungen
- Normal Aging - UpToDateDokument57 SeitenNormal Aging - UpToDatejoaopaulocuginottiNoch keine Bewertungen
- Surgery Elderly 4Dokument5 SeitenSurgery Elderly 4mx.pramirezNoch keine Bewertungen
- Heart Failure in Older Adults PDFDokument23 SeitenHeart Failure in Older Adults PDFcuisilaisNoch keine Bewertungen
- Question No 2 PDFDokument7 SeitenQuestion No 2 PDFPalwasha KhanNoch keine Bewertungen
- Rhinitis Allergy and ElderlyDokument26 SeitenRhinitis Allergy and ElderlyPutri Rizky AmaliaNoch keine Bewertungen
- Management of The Critically Ill Geriatric Patient: Paul E. Marik, MD, FCCMDokument7 SeitenManagement of The Critically Ill Geriatric Patient: Paul E. Marik, MD, FCCManisa7689Noch keine Bewertungen
- Prognostic MortalityDokument7 SeitenPrognostic MortalityZamzami SapoetraNoch keine Bewertungen
- Jurnal 5Dokument6 SeitenJurnal 5Siti rahmi AbukhaerNoch keine Bewertungen
- Seminar: John J V Mcmurray, Marc A PfefferDokument13 SeitenSeminar: John J V Mcmurray, Marc A Pfefferjvasco_santos8178Noch keine Bewertungen
- Bod Cerebrovasculardiseasestroke PDFDokument67 SeitenBod Cerebrovasculardiseasestroke PDFMax Laban SeminarioNoch keine Bewertungen
- Polytrauma in The Elderly: Specific Considerations and Current Concepts of ManagementDokument10 SeitenPolytrauma in The Elderly: Specific Considerations and Current Concepts of ManagementUdien Jmc Tíga TìgaNoch keine Bewertungen
- Influence of AgingDokument16 SeitenInfluence of AgingSCIH HFCPNoch keine Bewertungen
- Pearls and Pitfalls in The Crashing Geriatric PatientDokument12 SeitenPearls and Pitfalls in The Crashing Geriatric PatientVikrantNoch keine Bewertungen
- StrokeDokument67 SeitenStrokeGagi MiloševićNoch keine Bewertungen
- European Guidelines On Perioperative Venous.8Dokument7 SeitenEuropean Guidelines On Perioperative Venous.8ionut.andruscaNoch keine Bewertungen
- Bod - Cerebrovascular Disease Stroke BurdenDokument67 SeitenBod - Cerebrovascular Disease Stroke BurdenderiNoch keine Bewertungen
- Bod CerebrovasculardiseasestrokeDokument67 SeitenBod CerebrovasculardiseasestrokeErlin IrawatiNoch keine Bewertungen
- Arterial Hypertension and Aortic Valve Stenosis: Shedding Light On A Common "Liaison"Dokument6 SeitenArterial Hypertension and Aortic Valve Stenosis: Shedding Light On A Common "Liaison"Adriana VasilicaNoch keine Bewertungen
- DiscorsoDokument9 SeitenDiscorsodughi95Noch keine Bewertungen
- Abstract Case PresDokument6 SeitenAbstract Case PresSMJ DRDNoch keine Bewertungen
- Hypertension in ElderlyDokument13 SeitenHypertension in ElderlybookwormMD100% (2)
- A Review of Stroke in Pregnancy Incidence Investigations and Management Khalid 2020 The Obstetrician Gynaecologist Wiley Online LibraryDokument39 SeitenA Review of Stroke in Pregnancy Incidence Investigations and Management Khalid 2020 The Obstetrician Gynaecologist Wiley Online LibraryJAMPTNoch keine Bewertungen
- Association Between Acute Myocardial Infarction, Lipid Profile and Smoking HabitDokument5 SeitenAssociation Between Acute Myocardial Infarction, Lipid Profile and Smoking HabitIOSRjournalNoch keine Bewertungen
- Pulmonary Embolism in Intensive Care Unit: Michael Baram,, Bharat Awsare,, Geno MerliDokument9 SeitenPulmonary Embolism in Intensive Care Unit: Michael Baram,, Bharat Awsare,, Geno MerliTamaraNoch keine Bewertungen
- Sick Individuals and Sick Population by Rose. GDokument7 SeitenSick Individuals and Sick Population by Rose. GTate SimbaNoch keine Bewertungen
- Medicina 58 01078 v2Dokument14 SeitenMedicina 58 01078 v2Arief KamilNoch keine Bewertungen
- NICE 2010 Guidelines On VTEDokument509 SeitenNICE 2010 Guidelines On VTEzaidharbNoch keine Bewertungen
- Congestive Heart Failure in The ElderlyDokument13 SeitenCongestive Heart Failure in The ElderlyKezia MarsilinaNoch keine Bewertungen
- Management of Ischaemic Stroke2000Dokument29 SeitenManagement of Ischaemic Stroke2000FEllis LEoNoch keine Bewertungen
- Oral Anticoagulation in The Elderly and Frail: Rupert M. Bauersachs Joerg HeroldDokument10 SeitenOral Anticoagulation in The Elderly and Frail: Rupert M. Bauersachs Joerg Herold90STRATOVARIUS90Noch keine Bewertungen
- Schlitzkus 2015Dokument25 SeitenSchlitzkus 2015rnvisNoch keine Bewertungen
- 6 Osteoporotic Fractures in Older Adults: Cathleen S. Colo N-EmericDokument12 Seiten6 Osteoporotic Fractures in Older Adults: Cathleen S. Colo N-EmericRafael CastellarNoch keine Bewertungen
- Article 0785Dokument5 SeitenArticle 0785RaraZNoch keine Bewertungen
- Acute Kidney Injury in Elderly IntensiveDokument11 SeitenAcute Kidney Injury in Elderly IntensivefahlevyNoch keine Bewertungen
- Age-Related Longitudinal Change in Cardiac Structure and Function in Adults at Increased Cardiovascular RiskDokument18 SeitenAge-Related Longitudinal Change in Cardiac Structure and Function in Adults at Increased Cardiovascular Riskabraham rumayaraNoch keine Bewertungen
- Cerebral Venous Thrombosis From UptodateDokument20 SeitenCerebral Venous Thrombosis From UptodatewbudyaNoch keine Bewertungen
- Ehac 515Dokument18 SeitenEhac 515Phuoc NguyenNoch keine Bewertungen
- Stroke Epidemiology: Advancing Our Understanding of Disease Mechanism and TherapyDokument12 SeitenStroke Epidemiology: Advancing Our Understanding of Disease Mechanism and TherapyDodik's NihNoch keine Bewertungen
- Chapter 7. Longitudinal Studies: Nama: Sofia Marcelina NPM: A1E017005 PRODI: Pendidikan FisikaDokument4 SeitenChapter 7. Longitudinal Studies: Nama: Sofia Marcelina NPM: A1E017005 PRODI: Pendidikan FisikaSofia MarcelinaNoch keine Bewertungen
- J Amjcard 2009 10 007Dokument7 SeitenJ Amjcard 2009 10 007terminallllNoch keine Bewertungen
- Correa 2018Dokument52 SeitenCorrea 2018Esteban Matus MuñozNoch keine Bewertungen
- Causes of Heart FailureDokument4 SeitenCauses of Heart Failurejana7-7Noch keine Bewertungen
- Literature Review On Obesity and HypertensionDokument8 SeitenLiterature Review On Obesity and Hypertensionafdtygyhk100% (1)
- Screening For Osteoporosis: Clinical PracticeDokument8 SeitenScreening For Osteoporosis: Clinical PracticeGayuh PrastyaNoch keine Bewertungen
- Secondary HypertensionVon EverandSecondary HypertensionAlberto MorgantiNoch keine Bewertungen
- Atherosclerosis: Clinical Perspectives Through ImagingVon EverandAtherosclerosis: Clinical Perspectives Through ImagingNoch keine Bewertungen
- Diretrizes Européias para DislipidemiaDokument50 SeitenDiretrizes Européias para DislipidemiaEno FilhoNoch keine Bewertungen
- Cycle 13 Quiz 3 (CEID)Dokument2 SeitenCycle 13 Quiz 3 (CEID)DanielAndresNoch keine Bewertungen
- L.A. Noire Official Strategy GuideDokument321 SeitenL.A. Noire Official Strategy GuideDanielAndresNoch keine Bewertungen
- Formulario 1010 v5Dokument4 SeitenFormulario 1010 v5JuanCarlosValenzuelaMedina100% (2)
- Diretrizes Européias para DislipidemiaDokument50 SeitenDiretrizes Européias para DislipidemiaEno FilhoNoch keine Bewertungen
- Diretrizes Européias para DislipidemiaDokument50 SeitenDiretrizes Européias para DislipidemiaEno FilhoNoch keine Bewertungen
- Diretrizes Européias para DislipidemiaDokument50 SeitenDiretrizes Européias para DislipidemiaEno FilhoNoch keine Bewertungen
- Nuevo DX ColonDokument1 SeiteNuevo DX ColonDanielAndresNoch keine Bewertungen
- Diretrizes Européias para DislipidemiaDokument50 SeitenDiretrizes Européias para DislipidemiaEno FilhoNoch keine Bewertungen
- Extracting Heart Rate and Respiration Rate Using A Cell Phone CameraDokument6 SeitenExtracting Heart Rate and Respiration Rate Using A Cell Phone CameraPreethamReddyNoch keine Bewertungen
- Chronic Fatigue Syndrome From Vagus Nerve InfectionDokument10 SeitenChronic Fatigue Syndrome From Vagus Nerve InfectionLevente BalázsNoch keine Bewertungen
- RH RV TutorialDokument97 SeitenRH RV TutorialTavpritesh SethiNoch keine Bewertungen
- Mutual Influences Between Child Emotion Regulation and Parentchild Reciprocity Support Development Across The First 10 Years of Life Implications For Developmental PsychopathologyDokument17 SeitenMutual Influences Between Child Emotion Regulation and Parentchild Reciprocity Support Development Across The First 10 Years of Life Implications For Developmental PsychopathologyRaluca TudorNoch keine Bewertungen
- 2 Book Clinical - Applications - and - Interaction - Between - HRV - and - Heart - RateDokument168 Seiten2 Book Clinical - Applications - and - Interaction - Between - HRV - and - Heart - RateJulio OliveiraNoch keine Bewertungen
- Respiratory Sinus ArrhythmiaDokument8 SeitenRespiratory Sinus ArrhythmiaTatiana RecinosNoch keine Bewertungen
- Morgan 2012Dokument5 SeitenMorgan 2012aixacamila3Noch keine Bewertungen
- 2015 - Effects of Deep Pressure Stimulation On Physiological Arousal VAYU VEST With STRESSOR MORON TESTDokument5 Seiten2015 - Effects of Deep Pressure Stimulation On Physiological Arousal VAYU VEST With STRESSOR MORON TESTM Izzur MaulaNoch keine Bewertungen
- Breath Practices For Survivor and Caregiver Stress Depression ADokument24 SeitenBreath Practices For Survivor and Caregiver Stress Depression ADodik M. Nurul YamanNoch keine Bewertungen
- Physiology of Autonomic Nervous System: J J M Medical College, Davangere. Dept of AnesthesiaDokument117 SeitenPhysiology of Autonomic Nervous System: J J M Medical College, Davangere. Dept of AnesthesiaKithminaNoch keine Bewertungen
- Dufey Et Al - Sintonizando Con Otro La Teoría Polivagal y El Proceso de PsicoterapiaDokument10 SeitenDufey Et Al - Sintonizando Con Otro La Teoría Polivagal y El Proceso de PsicoterapiaMax RibeiroNoch keine Bewertungen
- Wireless Monitoring of Physiological Data Using Nexus-10 & BiotraceDokument64 SeitenWireless Monitoring of Physiological Data Using Nexus-10 & BiotraceInternational Journal of Application or Innovation in Engineering & ManagementNoch keine Bewertungen
- Conscious Breathing and Vagal ToneDokument8 SeitenConscious Breathing and Vagal Tonecora4eva5699Noch keine Bewertungen
- Polyvagal Theory - A Science of SafetyDokument15 SeitenPolyvagal Theory - A Science of SafetyShanthieNoch keine Bewertungen
- Campugan Jay Patho AssignmentDokument27 SeitenCampugan Jay Patho AssignmentJAY M. CAMPUGANNoch keine Bewertungen
- Teoria PolivagalDokument13 SeitenTeoria PolivagalPedro FlorNoch keine Bewertungen