Das könnte Ihnen auch gefallen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- A Case of Pulmonary Metastasis of Recurrent Giant Cell Tumor of BoneDokument1 SeiteA Case of Pulmonary Metastasis of Recurrent Giant Cell Tumor of BoneBagas WidhiarsoNoch keine Bewertungen
- Bone Cement Implantation SyndromeDokument5 SeitenBone Cement Implantation SyndromeBagas WidhiarsoNoch keine Bewertungen
- JurnalDokument4 SeitenJurnalBagas WidhiarsoNoch keine Bewertungen
- Bone Cement Implantation SyndromeDokument5 SeitenBone Cement Implantation SyndromeBagas WidhiarsoNoch keine Bewertungen
- Log Book MST November 2016Dokument5 SeitenLog Book MST November 2016Bagas WidhiarsoNoch keine Bewertungen
- ReferencesDokument2 SeitenReferencesBagas WidhiarsoNoch keine Bewertungen
- Ankle Fracture Treatment OptionsDokument19 SeitenAnkle Fracture Treatment OptionsBagas WidhiarsoNoch keine Bewertungen
- Log Book Hand Peb 17Dokument6 SeitenLog Book Hand Peb 17Bagas WidhiarsoNoch keine Bewertungen
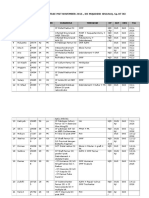
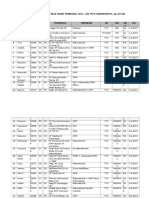
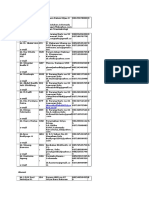
- LOG BOOK OPERASI STASE HAND JANUARI 2017 , DR TITO SUMARWOTO, Sp.OT (KDokument6 SeitenLOG BOOK OPERASI STASE HAND JANUARI 2017 , DR TITO SUMARWOTO, Sp.OT (KBagas WidhiarsoNoch keine Bewertungen
- DASH (Disabilities of The Arm, Shoulder and Hand)Dokument3 SeitenDASH (Disabilities of The Arm, Shoulder and Hand)Chriss ChristinaNoch keine Bewertungen
- Log Book Operasi Mei16Dokument2 SeitenLog Book Operasi Mei16Bagas WidhiarsoNoch keine Bewertungen
- Phalanx FractureDokument46 SeitenPhalanx FractureBagas WidhiarsoNoch keine Bewertungen
- Contact Person Draft RevisiDokument3 SeitenContact Person Draft RevisiBagas WidhiarsoNoch keine Bewertungen
- OTA Open Fracture ClassificationDokument1 SeiteOTA Open Fracture ClassificationPanda PavNoch keine Bewertungen
- 97042.15metatarsals S95 S98Dokument4 Seiten97042.15metatarsals S95 S98Bagas WidhiarsoNoch keine Bewertungen
- ACJointQx IMANAJKDokument11 SeitenACJointQx IMANAJKBagas WidhiarsoNoch keine Bewertungen
- Weaver Dunn ProcedureDokument3 SeitenWeaver Dunn ProcedureBagas WidhiarsoNoch keine Bewertungen
- Radial RadialisDokument1 SeiteRadial RadialisBagas WidhiarsoNoch keine Bewertungen
- 1043apdf SfjdasfhsdDokument8 Seiten1043apdf SfjdasfhsdBagas WidhiarsoNoch keine Bewertungen
- OTA Open Fracture ClassificationDokument1 SeiteOTA Open Fracture ClassificationPanda PavNoch keine Bewertungen
- Tibial HemimeliaDokument2 SeitenTibial HemimeliaBagas WidhiarsoNoch keine Bewertungen
- 97042.1TOC I IVDokument4 Seiten97042.1TOC I IVBagas WidhiarsoNoch keine Bewertungen
- PETA PASIEN BEDAH ANAK Jumat 26 September 2014 BGSL Bed Nama Umur CM Mrs Diagnosa OP STT S Plan Ket Lab StafDokument1 SeitePETA PASIEN BEDAH ANAK Jumat 26 September 2014 BGSL Bed Nama Umur CM Mrs Diagnosa OP STT S Plan Ket Lab StafBagas WidhiarsoNoch keine Bewertungen
- Peta Pasien Bedah Anak Sabtu 20 September 2014 BGSL Bed Nama Umur CM Mrs Diagnosa OP STT S Plan Ket Lab StafDokument1 SeitePeta Pasien Bedah Anak Sabtu 20 September 2014 BGSL Bed Nama Umur CM Mrs Diagnosa OP STT S Plan Ket Lab StafBagas WidhiarsoNoch keine Bewertungen
- PETA PASIEN BEDAH ANAK Rabu 24 September 2014 BGSL Bed Nama Umur CM Mrs Diagnosa OP STT S Plan Ket Lab StafDokument1 SeitePETA PASIEN BEDAH ANAK Rabu 24 September 2014 BGSL Bed Nama Umur CM Mrs Diagnosa OP STT S Plan Ket Lab StafBagas WidhiarsoNoch keine Bewertungen
- SELESAI The EndDokument1 SeiteSELESAI The EndBagas WidhiarsoNoch keine Bewertungen
- Mapping Bedah Anak 170914Dokument1 SeiteMapping Bedah Anak 170914Bagas WidhiarsoNoch keine Bewertungen
- Seminar & Workshop Total Hip Arthroplasty: Skill Lab Rso Prof DR R Soeharso Sabtu, 1 November 2014Dokument1 SeiteSeminar & Workshop Total Hip Arthroplasty: Skill Lab Rso Prof DR R Soeharso Sabtu, 1 November 2014Bagas WidhiarsoNoch keine Bewertungen
- SELESAI The EndDokument1 SeiteSELESAI The EndBagas WidhiarsoNoch keine Bewertungen
- Optician ChartDokument5 SeitenOptician ChartBagas WidhiarsoNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Twin-Field Quantum Key Distribution Without Optical Frequency DisseminationDokument8 SeitenTwin-Field Quantum Key Distribution Without Optical Frequency DisseminationHareesh PanakkalNoch keine Bewertungen
- Di OutlineDokument81 SeitenDi OutlineRobert E. BrannNoch keine Bewertungen
- UNDERSTANDING-WPS OfficeDokument51 SeitenUNDERSTANDING-WPS OfficeCristina Lance100% (1)
- Web Search - One People's Public Trust 1776 UCCDokument28 SeitenWeb Search - One People's Public Trust 1776 UCCVincent J. CataldiNoch keine Bewertungen
- Primer To Using Stampplot® Pro Standard User LicensedDokument21 SeitenPrimer To Using Stampplot® Pro Standard User LicensedSandy Rachman AdrianNoch keine Bewertungen
- The Human Element is Critical in Personal SellingDokument18 SeitenThe Human Element is Critical in Personal SellingArsalan AhmedNoch keine Bewertungen
- WORKSHOP ON ACCOUNTING OF IJARAHDokument12 SeitenWORKSHOP ON ACCOUNTING OF IJARAHAkif ShaikhNoch keine Bewertungen
- Sustainability of A Beach Resort A Case Study-1Dokument6 SeitenSustainability of A Beach Resort A Case Study-1abhinavsathishkumarNoch keine Bewertungen
- Phantom Susan KayDokument379 SeitenPhantom Susan Kaytheeyeofthemoon100% (9)
- People vs. Abad SantosDokument2 SeitenPeople vs. Abad SantosTrixie PeraltaNoch keine Bewertungen
- Javier Couso, Alexandra Huneeus, Rachel Sieder Cultures of Legality Judicialization and Political Activism in Latin America Cambridge Studies in Law and SocietyDokument290 SeitenJavier Couso, Alexandra Huneeus, Rachel Sieder Cultures of Legality Judicialization and Political Activism in Latin America Cambridge Studies in Law and SocietyLívia de SouzaNoch keine Bewertungen
- Grade 10 To 12 English Amplified PamphletDokument59 SeitenGrade 10 To 12 English Amplified PamphletChikuta ShingaliliNoch keine Bewertungen
- Neandertal Birth Canal Shape and The Evo PDFDokument6 SeitenNeandertal Birth Canal Shape and The Evo PDFashkenadaharsaNoch keine Bewertungen
- S The Big Five Personality TestDokument4 SeitenS The Big Five Personality TestXiaomi MIX 3Noch keine Bewertungen
- 2200SRM0724 (04 2005) Us en PDFDokument98 Seiten2200SRM0724 (04 2005) Us en PDFMayerson AlmaoNoch keine Bewertungen
- Philhis Handouts Week 1Dokument5 SeitenPhilhis Handouts Week 1Jeen JeenNoch keine Bewertungen
- Leading a Community Through Integrity and CourageDokument2 SeitenLeading a Community Through Integrity and CourageGretchen VenturaNoch keine Bewertungen
- Adjustment DisordersDokument2 SeitenAdjustment DisordersIsabel CastilloNoch keine Bewertungen
- Henderson - Historical Documents of The Middle AgesDokument536 SeitenHenderson - Historical Documents of The Middle AgesVlad VieriuNoch keine Bewertungen
- P7 Summary of ISADokument76 SeitenP7 Summary of ISAAlina Tariq100% (1)
- Longman - New Total English Elementary Video BankDokument26 SeitenLongman - New Total English Elementary Video Bankyuli100% (1)
- H-1 Nationalism in Europe NotesDokument5 SeitenH-1 Nationalism in Europe Noteskanishk kumarNoch keine Bewertungen
- Fractional GradingDokument7 SeitenFractional Gradingapi-355619062Noch keine Bewertungen
- Ororbia Maze LearningDokument10 SeitenOrorbia Maze LearningTom WestNoch keine Bewertungen
- 50 Cool Stories 3000 Hot Words (Master Vocabulary in 50 Days) For GRE Mba Sat Banking SSC DefDokument263 Seiten50 Cool Stories 3000 Hot Words (Master Vocabulary in 50 Days) For GRE Mba Sat Banking SSC DefaravindNoch keine Bewertungen
- Christian Appraisal of Feminist Ideologies Among Nigerian Women 2020Dokument78 SeitenChristian Appraisal of Feminist Ideologies Among Nigerian Women 2020Nwaozuru JOHNMAJOR ChinecheremNoch keine Bewertungen
- Psychology - A Separate PeaceDokument2 SeitenPsychology - A Separate PeacevasudhaaaaaNoch keine Bewertungen
- Endocrine Hypothyroidism HyperthyroidismDokument16 SeitenEndocrine Hypothyroidism HyperthyroidismJeel MohtaNoch keine Bewertungen
- Technical Specifications For The: LAMBDA 950 UV/Vis/NIR and LAMBDA 850 UV/Vis SpectrophotometersDokument4 SeitenTechnical Specifications For The: LAMBDA 950 UV/Vis/NIR and LAMBDA 850 UV/Vis SpectrophotometersDiogo GálicoNoch keine Bewertungen