Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Pearson - Age-Associated Changes in Blood Pressure in A Longitudinal Study of Healthy Men & WomenDokument7 SeitenPearson - Age-Associated Changes in Blood Pressure in A Longitudinal Study of Healthy Men & WomenxtraqrkyNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Leung (2008) - Familial Melanonychia StriataDokument4 SeitenLeung (2008) - Familial Melanonychia StriataxtraqrkyNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Baran & Kechijian (1996) - Hutchinson's Sign - A ReappraisalDokument4 SeitenBaran & Kechijian (1996) - Hutchinson's Sign - A ReappraisalxtraqrkyNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Braun Et Al. (2007) - Diagnosis and Management of Nail PigmentationsDokument13 SeitenBraun Et Al. (2007) - Diagnosis and Management of Nail PigmentationsxtraqrkyNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Selim (2008) - Melanonychia A Question of DensityDokument2 SeitenSelim (2008) - Melanonychia A Question of DensityxtraqrkyNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Harris Et Al. (2004) - Diagnosis and Treatment of Pediatric FlatfootDokument33 SeitenHarris Et Al. (2004) - Diagnosis and Treatment of Pediatric FlatfootxtraqrkyNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Morrison & Ferrari (2009) - Inter-Rater Reliability of The Foot Posture Index (FPI-6) in The Assessment of The Paediatric FootDokument6 SeitenMorrison & Ferrari (2009) - Inter-Rater Reliability of The Foot Posture Index (FPI-6) in The Assessment of The Paediatric FootxtraqrkyNoch keine Bewertungen
- Fitzpatricks Color Atlas and Synopsis of Clinical Dermatology - Exfoliative Erythroderma SyndromeDokument17 SeitenFitzpatricks Color Atlas and Synopsis of Clinical Dermatology - Exfoliative Erythroderma SyndromextraqrkyNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Sehgal Et Al. (2004) - Erythroderma :exfoliative Dermatitis - A SynopsisDokument9 SeitenSehgal Et Al. (2004) - Erythroderma :exfoliative Dermatitis - A SynopsisxtraqrkyNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- RH IncompatibilityDokument10 SeitenRH IncompatibilityVernie Dinglasa GeligNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Bioethics in The 21st CenturyDokument164 SeitenBioethics in The 21st CenturyAndika SiswantaNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Food Safety and Sanitation ManagementDokument71 SeitenFood Safety and Sanitation Managementshielad_4100% (1)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Drugstudy - Delivery RoomDokument12 SeitenDrugstudy - Delivery RoomAUBREY MARIE . GUERRERONoch keine Bewertungen
- NephritisDokument16 SeitenNephritisyikesNoch keine Bewertungen
- Labor Case Digest FR Azucena BookDokument11 SeitenLabor Case Digest FR Azucena BookAnonymous rVdy7u5Noch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
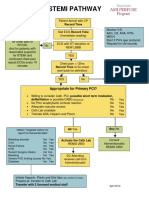
- Stemi Pathway: Record TimeDokument2 SeitenStemi Pathway: Record TimeOlga Jadha CasmiraNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Developing A ParagraphDokument12 SeitenDeveloping A ParagraphKhairul AnuarNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Pathophysiology MCQ With Answers PDFDokument4 SeitenPathophysiology MCQ With Answers PDF02 Babar Saurabh NavnathNoch keine Bewertungen
- Case Study FormatDokument11 SeitenCase Study FormatDemecillo, NoelleNoch keine Bewertungen
- PancreatitisDokument23 SeitenPancreatitissalmanhabeebekNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Test Bank For Medical Genetics 4th Edition Lynn B JordeDokument8 SeitenTest Bank For Medical Genetics 4th Edition Lynn B JorderoytuyenbauNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- OHS - U-3 - Socio-Economic and Gender Aspects of M&EDokument57 SeitenOHS - U-3 - Socio-Economic and Gender Aspects of M&Esidda lingeshaNoch keine Bewertungen
- Abaya Vs ECCDokument4 SeitenAbaya Vs ECCJudith LaguitaoNoch keine Bewertungen
- Benzo ZdrugDokument12 SeitenBenzo Zdruglnair_43Noch keine Bewertungen
- NCP DM 1Dokument6 SeitenNCP DM 1Shin AblangNoch keine Bewertungen
- Getting Crap Out of A CatDokument5 SeitenGetting Crap Out of A CatLarasati FadhlenNoch keine Bewertungen
- Health Guide Lines For Ramadan FastingDokument4 SeitenHealth Guide Lines For Ramadan Fastingmaidul.islamNoch keine Bewertungen
- Doctor Shift PatternDokument4 SeitenDoctor Shift PatternHalilGutajNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Sheehan's Syndrome.Dokument4 SeitenSheehan's Syndrome.MosesNoch keine Bewertungen
- Tut Essay - CompleteDokument3 SeitenTut Essay - Completeapi-208141723Noch keine Bewertungen
- Microbiology: Presented by Alyazeed Hussein, BSCDokument64 SeitenMicrobiology: Presented by Alyazeed Hussein, BSCT N100% (1)
- DynamedDokument41 SeitenDynamedkaren AlvaradoNoch keine Bewertungen
- Mitral Stenosis (MS) X Mitral Regurgitasi (MR)Dokument25 SeitenMitral Stenosis (MS) X Mitral Regurgitasi (MR)Nur Faydotus SalsabilaNoch keine Bewertungen
- Acute Isolated MyocarditisDokument20 SeitenAcute Isolated Myocarditismerin sunilNoch keine Bewertungen
- AnophthalmaDokument17 SeitenAnophthalmaMarvellous OkonobohNoch keine Bewertungen
- 9 - Keeping The Digestive System Healthy PDFDokument11 Seiten9 - Keeping The Digestive System Healthy PDFAnthony GonzalesNoch keine Bewertungen
- EH Talk 9 Miasms - FLowchart PDFDokument6 SeitenEH Talk 9 Miasms - FLowchart PDFcausmicdanceNoch keine Bewertungen
- Narrative Report in School Clinic Sy 2018 - 2019Dokument8 SeitenNarrative Report in School Clinic Sy 2018 - 2019Daiseree Salvador100% (7)
- Practice Mmi Questions Station 1: Placebo (Ethical Decision Making)Dokument2 SeitenPractice Mmi Questions Station 1: Placebo (Ethical Decision Making)Nicolas CortezNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)