Das könnte Ihnen auch gefallen
- Daftar Pustaka TuberkulomaDokument1 SeiteDaftar Pustaka TuberkulomagowindamijayaNoch keine Bewertungen
- BR J Ophthalmol 1979 Akkermans 129 31Dokument4 SeitenBR J Ophthalmol 1979 Akkermans 129 31gowindamijayaNoch keine Bewertungen
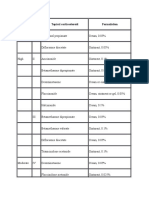
- Potency Class Topical Corticosteroid FormulationDokument5 SeitenPotency Class Topical Corticosteroid FormulationgowindamijayaNoch keine Bewertungen
- BronkiektasisDokument25 SeitenBronkiektasisgowindamijayaNoch keine Bewertungen
- JMedLife 04 330Dokument16 SeitenJMedLife 04 330gowindamijayaNoch keine Bewertungen
- 73Dokument2 Seiten73gowindamijayaNoch keine Bewertungen
- DAFTARDokument1 SeiteDAFTARgowindamijayaNoch keine Bewertungen
- EUCAST Detection of Resistance Mechanisms v1.0 20131211Dokument40 SeitenEUCAST Detection of Resistance Mechanisms v1.0 20131211gowindamijayaNoch keine Bewertungen
- MPA vs PAN: Two Vasculitis ConditionsDokument1 SeiteMPA vs PAN: Two Vasculitis ConditionsgowindamijayaNoch keine Bewertungen
- Hasil To SBMPTNDokument17 SeitenHasil To SBMPTNYid BajangNoch keine Bewertungen
- EUCAST Detection of Resistance Mechanisms v1.0 20131211Dokument40 SeitenEUCAST Detection of Resistance Mechanisms v1.0 20131211gowindamijayaNoch keine Bewertungen
- Istc 2009Dokument84 SeitenIstc 2009Nur FaiZah HaRunNoch keine Bewertungen
- MPA vs PAN: Two Vasculitis ConditionsDokument1 SeiteMPA vs PAN: Two Vasculitis ConditionsgowindamijayaNoch keine Bewertungen
- Galazka AMDokument1 SeiteGalazka AMgowindamijayaNoch keine Bewertungen
- Daftar Pustaka EssaiDokument1 SeiteDaftar Pustaka EssaigowindamijayaNoch keine Bewertungen
- Trypanosomiasis AfricanDokument5 SeitenTrypanosomiasis AfricangowindamijayaNoch keine Bewertungen
- Trypanosomiasis AmericanDokument8 SeitenTrypanosomiasis AmericanJosé Isaac Lamas GarcíaNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Bibliography Clothing TextilesDokument138 SeitenBibliography Clothing Textilesjagan19790% (1)
- Flaws and All: I Been OnDokument6 SeitenFlaws and All: I Been OnJéssica FreitasNoch keine Bewertungen
- Neutrophil Function From Mechanism To DiseaseDokument33 SeitenNeutrophil Function From Mechanism To DiseaseMajoo HernándezNoch keine Bewertungen
- Respiratory SystemDokument36 SeitenRespiratory Systemسارة عبد الكاظم مكطوفNoch keine Bewertungen
- Word Analogy and Number Puzzles SEODokument44 SeitenWord Analogy and Number Puzzles SEOAjith abdulNoch keine Bewertungen
- Test Bank For Operations Management 14th Edition William J StevensonDokument36 SeitenTest Bank For Operations Management 14th Edition William J Stevensonmasqueedenized8a43l100% (44)
- Examen InglésDokument10 SeitenExamen InglésAntonio CórdovaNoch keine Bewertungen
- Berriozabal-Islas Et Al. 2017Dokument11 SeitenBerriozabal-Islas Et Al. 2017Anonymous 0zpUv8cmqbNoch keine Bewertungen
- Ferdinand SequencingDokument2 SeitenFerdinand SequencingEFL Classroom 2.0Noch keine Bewertungen
- Beyond The VeilDokument589 SeitenBeyond The VeilJRNoch keine Bewertungen
- NAT Reviewer ScienceDokument3 SeitenNAT Reviewer ScienceRandy100% (1)
- Hannah ReevesDokument2 SeitenHannah Reevesapi-242939734Noch keine Bewertungen
- Characteristics of Life Long TestDokument5 SeitenCharacteristics of Life Long TestMichelle Ramirez Co-GonzalesNoch keine Bewertungen
- Verb classes and types in English and UkrainianDokument16 SeitenVerb classes and types in English and UkrainianАнастасия ДобровольскаяNoch keine Bewertungen
- Wambui ImciDokument1 SeiteWambui ImciHERRERA, ANGELANoch keine Bewertungen
- The Jungle Book - The Cobra 39 S Egg Watts Michael 2013Dokument36 SeitenThe Jungle Book - The Cobra 39 S Egg Watts Michael 2013mamermNoch keine Bewertungen
- Physical Examination Form: Return by July 17ThDokument1 SeitePhysical Examination Form: Return by July 17ThFlorian Ananias ByarugabaNoch keine Bewertungen
- Identifying Venomous and Nonvenomous Snakes in TexasDokument10 SeitenIdentifying Venomous and Nonvenomous Snakes in TexasAttila KissNoch keine Bewertungen
- Quarter 3, Week 1 English Inkay - PeraltaDokument47 SeitenQuarter 3, Week 1 English Inkay - PeraltaPatrick EdrosoloNoch keine Bewertungen
- EquestrianCatalogue - 2014 As at 26th NovemberDokument29 SeitenEquestrianCatalogue - 2014 As at 26th NovemberAnne HjorthNoch keine Bewertungen
- Biology ProjectDokument19 SeitenBiology ProjectJaya mohanNoch keine Bewertungen
- CH 42 Circulatory Systems: AP BiologyDokument27 SeitenCH 42 Circulatory Systems: AP BiologyNelson TingalingNoch keine Bewertungen
- VB2 Grammar Lesson2 ExtraDokument20 SeitenVB2 Grammar Lesson2 ExtraOanh Nguyễn100% (1)
- Charcuteria Libro PDFDokument313 SeitenCharcuteria Libro PDFFederico GómezNoch keine Bewertungen
- Skinwalker - Monsters - Homebrew - D&D BeyondDokument1 SeiteSkinwalker - Monsters - Homebrew - D&D BeyondCallum MacgregorNoch keine Bewertungen
- Atlas Games2Dokument2 SeitenAtlas Games2Beki LokaNoch keine Bewertungen
- Undefined The Penguin Dictionary of PDFDokument304 SeitenUndefined The Penguin Dictionary of PDFMaliha Cheema100% (2)
- Charlotte (Gaint Faerie Hamster)Dokument3 SeitenCharlotte (Gaint Faerie Hamster)DebraLievenNoch keine Bewertungen
- PressedDokument8 SeitenPressedJohnGioloneNoch keine Bewertungen
- The Blonde and The Lawyer GameDokument15 SeitenThe Blonde and The Lawyer GameChristevanNoch keine Bewertungen