Das könnte Ihnen auch gefallen
- Request For Project/Programme Funding From The Adaptation FundDokument166 SeitenRequest For Project/Programme Funding From The Adaptation FundNhialNoch keine Bewertungen
- Digital Marketing: Nanodegree Program SyllabusDokument22 SeitenDigital Marketing: Nanodegree Program SyllabusjhgfNoch keine Bewertungen
- Daisys Philosophy of Education Spring 2022 1Dokument25 SeitenDaisys Philosophy of Education Spring 2022 1api-603772650Noch keine Bewertungen
- The Role of Student Affairs in Student Learning AssessmentDokument18 SeitenThe Role of Student Affairs in Student Learning AssessmentRyan Michael Oducado100% (1)
- 12 CSS Q4 M3 StampedDokument17 Seiten12 CSS Q4 M3 StampedJunebel YosoresNoch keine Bewertungen
- Weboc 1Dokument30 SeitenWeboc 1Altaf Ur RehmanNoch keine Bewertungen
- A M 06 Ironmongery July 09Dokument13 SeitenA M 06 Ironmongery July 09suneethmohanNoch keine Bewertungen
- Trash BallDokument7 SeitenTrash BallRizzah MagnoNoch keine Bewertungen
- Surat Resmi Dan Tak ResmiDokument7 SeitenSurat Resmi Dan Tak ResmideviansdoniNoch keine Bewertungen
- MOW ConcreteDokument76 SeitenMOW ConcretesuneethmohanNoch keine Bewertungen
- Rakata PDFDokument3 SeitenRakata PDFMuhammad IlhamNoch keine Bewertungen
- How To Create A Winning Social Media ReportDokument21 SeitenHow To Create A Winning Social Media Reportdmh1976Noch keine Bewertungen
- Test Report Motor - 4578450AAENGDokument4 SeitenTest Report Motor - 4578450AAENGjacklyn ade putraNoch keine Bewertungen
- A M 16 Electrical Installation July 09Dokument61 SeitenA M 16 Electrical Installation July 09suneethmohanNoch keine Bewertungen
- Electrom Instruments: iTIG II Series Winding AnalyzersDokument87 SeitenElectrom Instruments: iTIG II Series Winding AnalyzersJose Raul LeonNoch keine Bewertungen
- PA00K8FDokument33 SeitenPA00K8FomarnoamanNoch keine Bewertungen
- PT 1 CSS8 2018Dokument9 SeitenPT 1 CSS8 2018Gerean Abeleda-VillasNoch keine Bewertungen
- Community Rights and Welfare (CRAW) Proposal: Mary Philline DescalzoDokument5 SeitenCommunity Rights and Welfare (CRAW) Proposal: Mary Philline DescalzoUSCUPDNoch keine Bewertungen
- SHIROVASTIDokument3 SeitenSHIROVASTINatseenNoch keine Bewertungen
- Glass & GlazingDokument20 SeitenGlass & GlazingsuneethmohanNoch keine Bewertungen
- Invitation Michaelhollender PDFDokument27 SeitenInvitation Michaelhollender PDFPrakash SantraNoch keine Bewertungen
- German NGO AppDokument12 SeitenGerman NGO AppsimbiroNoch keine Bewertungen
- Hijab Representation in FashionDokument8 SeitenHijab Representation in Fashionapi-533571781100% (1)
- UNDEF Projects DatabaseDokument62 SeitenUNDEF Projects DatabasefagchNoch keine Bewertungen
- Emarketer - Retail Trends 2023Dokument6 SeitenEmarketer - Retail Trends 2023jhoni ambaritaNoch keine Bewertungen
- 9 CSS Q4 M4 StampedDokument15 Seiten9 CSS Q4 M4 StampedJunebel YosoresNoch keine Bewertungen
- English AfanOromoGlossaryDokument81 SeitenEnglish AfanOromoGlossaryMillimoh Asfaw100% (1)
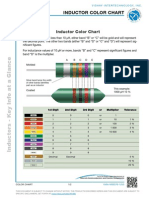
- Inductor ChartDokument2 SeitenInductor Chartshaswat_23Noch keine Bewertungen
- KWLDokument1 SeiteKWLChernobog100% (1)
- Nov. 7 G10Dokument56 SeitenNov. 7 G10Honey Diana MejiaNoch keine Bewertungen
- Libraries New EssayDokument1 SeiteLibraries New EssayMohammad Kashif Saeed KunwarNoch keine Bewertungen
- Peace Corps Cambodia Welcome Book - 2012Dokument75 SeitenPeace Corps Cambodia Welcome Book - 2012Accessible Journal Media: Peace Corps DocumentsNoch keine Bewertungen
- Keraliya Panchakarma Therapy: Ayurveda Is A Science of Life. The Chief Object of This Science AreDokument12 SeitenKeraliya Panchakarma Therapy: Ayurveda Is A Science of Life. The Chief Object of This Science Arerocky006600Noch keine Bewertungen
- Edt 180 Reflection PaperDokument3 SeitenEdt 180 Reflection Paperapi-500170226Noch keine Bewertungen
- CRAW Committee ProposalDokument12 SeitenCRAW Committee ProposalheartdinoNoch keine Bewertungen
- MOW General Spec.Dokument20 SeitenMOW General Spec.suneethmohanNoch keine Bewertungen
- GenderCommProposal ReynoDokument5 SeitenGenderCommProposal ReynoUSCUPDNoch keine Bewertungen
- 1277-Article Text-4013-1-10-20211021Dokument9 Seiten1277-Article Text-4013-1-10-20211021Ummu AthiyyahNoch keine Bewertungen
- Community Rights and Welfare Committee C/o Councilor Mico PangalanganDokument7 SeitenCommunity Rights and Welfare Committee C/o Councilor Mico PangalanganArjay MercadoNoch keine Bewertungen
- USAID DAI ContractDokument41 SeitenUSAID DAI ContractJDStusterNoch keine Bewertungen
- Bluetooth Indoor PositioningDokument56 SeitenBluetooth Indoor PositioningGabriela MateiNoch keine Bewertungen
- PVCHR: Tactics and StrategyDokument29 SeitenPVCHR: Tactics and StrategyPeoples' Vigilance Committee on Human rights100% (1)
- Annual Progress ReportDokument26 SeitenAnnual Progress Reportactivist knowledge center100% (1)
- Manipur Torture Report 2015Dokument69 SeitenManipur Torture Report 2015MansinghNepramNoch keine Bewertungen
- OppSpeaker 2motion 1Dokument2 SeitenOppSpeaker 2motion 1priyagaur27Noch keine Bewertungen
- Dr. Bhim Rao Ambedkar College Department of Social WorkDokument3 SeitenDr. Bhim Rao Ambedkar College Department of Social WorkYadav NitinNoch keine Bewertungen
- Despair To HopeDokument85 SeitenDespair To HopePeoples' Vigilance Committee on Human rightsNoch keine Bewertungen
- Dr. Bhim Rao Ambedkar College Department of Social WorkDokument3 SeitenDr. Bhim Rao Ambedkar College Department of Social WorkYadav NitinNoch keine Bewertungen
- Medical Examination of Rape VictimsDokument14 SeitenMedical Examination of Rape VictimsTirtharaj ChoudhuryNoch keine Bewertungen
- Targetted Intervention Program For Sex Work ProfessionalsDokument14 SeitenTargetted Intervention Program For Sex Work ProfessionalsJuree HojaiNoch keine Bewertungen
- Victims' Perspectives About The Human Rights Violations HearingsDokument21 SeitenVictims' Perspectives About The Human Rights Violations HearingsPaula OrtizNoch keine Bewertungen
- Gujarat Earthquake Indian Peoples Tribunal ReportDokument80 SeitenGujarat Earthquake Indian Peoples Tribunal ReportRiaNoch keine Bewertungen
- Guide To Judge With A Gender Perspective 2022Dokument107 SeitenGuide To Judge With A Gender Perspective 2022noeliaNoch keine Bewertungen
- Gujarat Earthquake - Indian Peoples' Tribunal Report.Dokument80 SeitenGujarat Earthquake - Indian Peoples' Tribunal Report.willyindiaNoch keine Bewertungen
- First Pilot Project of PVCHR-RCT For Testimonial TherapyDokument49 SeitenFirst Pilot Project of PVCHR-RCT For Testimonial TherapyPeoples' Vigilance Committee on Human rightsNoch keine Bewertungen
- Vats Family 1Dokument20 SeitenVats Family 1Krishna AhujaNoch keine Bewertungen
- UNESCO CMW AsiePac1Dokument68 SeitenUNESCO CMW AsiePac1faye wongNoch keine Bewertungen
- Sem7 CRPC TanuDokument18 SeitenSem7 CRPC TanuTaruna ShandilyaNoch keine Bewertungen
- ARM SOP English VersionDokument70 SeitenARM SOP English Versioniaderae6784Noch keine Bewertungen
- Article On Child Rights PDFDokument8 SeitenArticle On Child Rights PDFactivist knowledge centerNoch keine Bewertungen
- HRDA - UA - North - Uttar Pradesh - Mr. Lenin RaghuvanshiDokument3 SeitenHRDA - UA - North - Uttar Pradesh - Mr. Lenin Raghuvanshiactivist knowledge centerNoch keine Bewertungen
- Resilience Baseed On Hope Honour and DignityDokument15 SeitenResilience Baseed On Hope Honour and Dignityactivist knowledge centerNoch keine Bewertungen
- Strategic Plan of PVCHR/JMN For Year 2015-2018Dokument28 SeitenStrategic Plan of PVCHR/JMN For Year 2015-2018activist knowledge centerNoch keine Bewertungen
- Despair To HopeDokument85 SeitenDespair To HopePeoples' Vigilance Committee on Human rightsNoch keine Bewertungen
- PVCHR Submission About Access To Water and Sanitation To Marginalized CommunitiesDokument3 SeitenPVCHR Submission About Access To Water and Sanitation To Marginalized Communitiesactivist knowledge centerNoch keine Bewertungen
- Annual Progress ReportDokument26 SeitenAnnual Progress Reportactivist knowledge center100% (1)
- Media List of PVCHR On Bonded Labour From 1996 - 2013Dokument21 SeitenMedia List of PVCHR On Bonded Labour From 1996 - 2013activist knowledge centerNoch keine Bewertungen
- List of The Bonded Labour and Child Labour Who Rescued and Received Release Certificate and Rehabilitation Package - Data of PVCHR From 1996 - 2003 (Part - 2)Dokument11 SeitenList of The Bonded Labour and Child Labour Who Rescued and Received Release Certificate and Rehabilitation Package - Data of PVCHR From 1996 - 2003 (Part - 2)activist knowledge centerNoch keine Bewertungen
- Compilation of Different Political Parties Election ManifestoDokument21 SeitenCompilation of Different Political Parties Election Manifestoactivist knowledge centerNoch keine Bewertungen
- List of Prison Inmates in Varanasi Central PrisonDokument26 SeitenList of Prison Inmates in Varanasi Central Prisonactivist knowledge centerNoch keine Bewertungen
- Voice of Voicesless: Vol 4 No. 2Dokument58 SeitenVoice of Voicesless: Vol 4 No. 2activist knowledge centerNoch keine Bewertungen
- List of The Bonded Labour Rescued and Received Release Certificate and Rehabilitation Certificate - Data of PVCHR From 1996 - 2003Dokument49 SeitenList of The Bonded Labour Rescued and Received Release Certificate and Rehabilitation Certificate - Data of PVCHR From 1996 - 2003activist knowledge centerNoch keine Bewertungen
- A Guiding Manual For Bonded Labour in HindiDokument2 SeitenA Guiding Manual For Bonded Labour in Hindiactivist knowledge centerNoch keine Bewertungen
- Election of Governing Board and Social Audit of Jan Mitra Nyas/PVCHRDokument2 SeitenElection of Governing Board and Social Audit of Jan Mitra Nyas/PVCHRactivist knowledge centerNoch keine Bewertungen
- Shiksha Ka AdhikarDokument3 SeitenShiksha Ka Adhikaractivist knowledge centerNoch keine Bewertungen
- Torture of Underprivileged Class by Authorise SafeguardersDokument9 SeitenTorture of Underprivileged Class by Authorise Safeguardersactivist knowledge centerNoch keine Bewertungen
- PIL On The Subject of Right of Education of The Children Who Are Living in Different Prisons of Uttar Pradesh Alongwith Their Mothers.Dokument29 SeitenPIL On The Subject of Right of Education of The Children Who Are Living in Different Prisons of Uttar Pradesh Alongwith Their Mothers.activist knowledge centerNoch keine Bewertungen
- Judgement On The PILDokument1 SeiteJudgement On The PILactivist knowledge centerNoch keine Bewertungen
- PIL On The Subject of Right of Education of The Children Who Are Living in Different Prisons of Uttar Pradesh Alongwith Their Mothers.Dokument29 SeitenPIL On The Subject of Right of Education of The Children Who Are Living in Different Prisons of Uttar Pradesh Alongwith Their Mothers.activist knowledge centerNoch keine Bewertungen
- Verdict in The Case of Sexual Assault by The Police ConstableDokument12 SeitenVerdict in The Case of Sexual Assault by The Police Constableactivist knowledge centerNoch keine Bewertungen
- Akkhan Mushar IIDokument12 SeitenAkkhan Mushar IIactivist knowledge centerNoch keine Bewertungen
- Akkhar MuhsarDokument14 SeitenAkkhar Muhsaractivist knowledge centerNoch keine Bewertungen
- News Published in Various NewspaperDokument15 SeitenNews Published in Various Newspaperactivist knowledge centerNoch keine Bewertungen
- Judgement On The PILDokument1 SeiteJudgement On The PILactivist knowledge centerNoch keine Bewertungen
- Comprehensive Program For Survivors of Torture and Organized ViolenceDokument36 SeitenComprehensive Program For Survivors of Torture and Organized Violenceactivist knowledge centerNoch keine Bewertungen
- Attack On Dr. Lenin PDFDokument2 SeitenAttack On Dr. Lenin PDFactivist knowledge centerNoch keine Bewertungen
- Neo Dalit Celebration in KodermaDokument1 SeiteNeo Dalit Celebration in Kodermaactivist knowledge centerNoch keine Bewertungen
- Comprehensive Program For Survivors of Torture and Organized ViolenceDokument36 SeitenComprehensive Program For Survivors of Torture and Organized Violenceactivist knowledge centerNoch keine Bewertungen
- Awareness BuildingDokument2 SeitenAwareness Buildingactivist knowledge centerNoch keine Bewertungen
- Ali Et Al., 2017 How Durable Is The Effect of Low Intensity CBT For Depression and AnxietyDokument8 SeitenAli Et Al., 2017 How Durable Is The Effect of Low Intensity CBT For Depression and AnxietyZehraNoch keine Bewertungen
- COUNSELINGDokument13 SeitenCOUNSELINGfrederick macaleNoch keine Bewertungen
- CBT For PsychosisDokument45 SeitenCBT For PsychosisNadia Boxer100% (1)
- Beh - Thorndike - Student - S - Copy - PPT Filename - UTF-8''Beh - Thorndike - Student - S CDokument24 SeitenBeh - Thorndike - Student - S - Copy - PPT Filename - UTF-8''Beh - Thorndike - Student - S CRevira EstorelNoch keine Bewertungen
- Multidimensional Family Therapy PDFDokument21 SeitenMultidimensional Family Therapy PDFBakos BenceNoch keine Bewertungen
- CBT For ADHD in Adults: Cognitive Behavioral Therapy For ADD SymptomsDokument6 SeitenCBT For ADHD in Adults: Cognitive Behavioral Therapy For ADD Symptomsrico rubenNoch keine Bewertungen
- Psychology Frontiers and ApplicationsDokument881 SeitenPsychology Frontiers and ApplicationsRoman Bal100% (2)
- Dark Night of The Soul (Kumpulan Tulisan Singkat)Dokument15 SeitenDark Night of The Soul (Kumpulan Tulisan Singkat)Alvin HadiwonoNoch keine Bewertungen
- PTSD Type 1, OSCILLOPSIA, EMDR and A PTSD Type 2Dokument29 SeitenPTSD Type 1, OSCILLOPSIA, EMDR and A PTSD Type 2do leeNoch keine Bewertungen
- Just Therapy PublicationsDokument48 SeitenJust Therapy PublicationsCésar Hernández LaraNoch keine Bewertungen
- Code of Ethics DVDokument5 SeitenCode of Ethics DVapi-231342001Noch keine Bewertungen
- WHO - Maternal Mental Health and Child Health and Development in Low and Middle Income Countries PDFDokument39 SeitenWHO - Maternal Mental Health and Child Health and Development in Low and Middle Income Countries PDFCamila PyongaNoch keine Bewertungen
- Films in PsychologyDokument288 SeitenFilms in PsychologyDharaa GuptaNoch keine Bewertungen
- Internship Application FormDokument1 SeiteInternship Application FormCedric Joseph MandapNoch keine Bewertungen
- History and Roots of Gestalt Therapy TheDokument10 SeitenHistory and Roots of Gestalt Therapy TheobchodxNoch keine Bewertungen
- Pre Observation ConferenceDokument4 SeitenPre Observation ConferenceJonas Miranda CabusbusanNoch keine Bewertungen
- Attention in Personality DevelopmentDokument15 SeitenAttention in Personality DevelopmentZubair LatifNoch keine Bewertungen
- BasingDokument7 SeitenBasingDyang Wulan AprilianiNoch keine Bewertungen
- Guidelines SupervisionDokument46 SeitenGuidelines SupervisionDianaSantiago100% (1)
- Standards Goals ObjectivesDokument2 SeitenStandards Goals ObjectivesChristine OrenseNoch keine Bewertungen
- Introduction To Psychology.2Dokument15 SeitenIntroduction To Psychology.2khawar abbasi100% (1)
- PCN 12481 PDFDokument2 SeitenPCN 12481 PDFFernandoNoch keine Bewertungen
- Brown BearDokument6 SeitenBrown Bearapi-296126471Noch keine Bewertungen
- Case Conceptualiz Ation: Course Instructor Tabinda AfzalDokument18 SeitenCase Conceptualiz Ation: Course Instructor Tabinda AfzalJERRY ZARANoch keine Bewertungen
- 【课件】自然游戏治疗01场Dokument67 Seiten【课件】自然游戏治疗01场xjawyh0208Noch keine Bewertungen
- Brock, Batten, Walser, Robb (2015) Recognizing Common Clinical Mistakes in ACT PDFDokument5 SeitenBrock, Batten, Walser, Robb (2015) Recognizing Common Clinical Mistakes in ACT PDFAlexNoch keine Bewertungen
- Lesson Plan1 Letter WDokument3 SeitenLesson Plan1 Letter Wapi-307983330Noch keine Bewertungen
- Reflection Paper On Psychoanalytic TheoryDokument4 SeitenReflection Paper On Psychoanalytic Theoryisabela100% (1)
- 000524425Dokument12 Seiten000524425Lluís Martínez SalvadorNoch keine Bewertungen
- Maternal Child Nursing Care 2nd Edition Ward Test BankDokument26 SeitenMaternal Child Nursing Care 2nd Edition Ward Test Bankkevincharlesfztodrpwck100% (14)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (24)
- Do Dead People Watch You Shower?: And Other Questions You've Been All but Dying to Ask a MediumVon EverandDo Dead People Watch You Shower?: And Other Questions You've Been All but Dying to Ask a MediumBewertung: 3.5 von 5 Sternen3.5/5 (20)
- Dogland: Passion, Glory, and Lots of Slobber at the Westminster Dog ShowVon EverandDogland: Passion, Glory, and Lots of Slobber at the Westminster Dog ShowNoch keine Bewertungen
- Cynical Theories: How Activist Scholarship Made Everything about Race, Gender, and Identity―and Why This Harms EverybodyVon EverandCynical Theories: How Activist Scholarship Made Everything about Race, Gender, and Identity―and Why This Harms EverybodyBewertung: 4.5 von 5 Sternen4.5/5 (221)
- Welcome to the United States of Anxiety: Observations from a Reforming NeuroticVon EverandWelcome to the United States of Anxiety: Observations from a Reforming NeuroticBewertung: 3.5 von 5 Sternen3.5/5 (10)
- The Season: Inside Palm Beach and America's Richest SocietyVon EverandThe Season: Inside Palm Beach and America's Richest SocietyBewertung: 4.5 von 5 Sternen4.5/5 (5)
- Lost in a Good Game: Why we play video games and what they can do for usVon EverandLost in a Good Game: Why we play video games and what they can do for usBewertung: 4.5 von 5 Sternen4.5/5 (31)
- The Canceling of the American Mind: Cancel Culture Undermines Trust, Destroys Institutions, and Threatens Us All—But There Is a SolutionVon EverandThe Canceling of the American Mind: Cancel Culture Undermines Trust, Destroys Institutions, and Threatens Us All—But There Is a SolutionBewertung: 4 von 5 Sternen4/5 (16)
- You Never Give Me Your Money: The Beatles After the BreakupVon EverandYou Never Give Me Your Money: The Beatles After the BreakupNoch keine Bewertungen
- Rage Becomes Her: The Power of Women's AngerVon EverandRage Becomes Her: The Power of Women's AngerBewertung: 4.5 von 5 Sternen4.5/5 (184)
- 1963: The Year of the Revolution: How Youth Changed the World with Music, Fashion, and ArtVon Everand1963: The Year of the Revolution: How Youth Changed the World with Music, Fashion, and ArtBewertung: 4 von 5 Sternen4/5 (5)
- Alright, Alright, Alright: The Oral History of Richard Linklater's Dazed and ConfusedVon EverandAlright, Alright, Alright: The Oral History of Richard Linklater's Dazed and ConfusedBewertung: 4 von 5 Sternen4/5 (23)
- As You Wish: Inconceivable Tales from the Making of The Princess BrideVon EverandAs You Wish: Inconceivable Tales from the Making of The Princess BrideBewertung: 4.5 von 5 Sternen4.5/5 (1182)
- Greek Mythology: The Gods, Goddesses, and Heroes Handbook: From Aphrodite to Zeus, a Profile of Who's Who in Greek MythologyVon EverandGreek Mythology: The Gods, Goddesses, and Heroes Handbook: From Aphrodite to Zeus, a Profile of Who's Who in Greek MythologyBewertung: 4.5 von 5 Sternen4.5/5 (72)
- Silver Screen Fiend: Learning About Life from an Addiction to FilmVon EverandSilver Screen Fiend: Learning About Life from an Addiction to FilmBewertung: 4 von 5 Sternen4/5 (182)
- Attack from Within: How Disinformation Is Sabotaging AmericaVon EverandAttack from Within: How Disinformation Is Sabotaging AmericaBewertung: 4 von 5 Sternen4/5 (5)
- Good Booty: Love and Sex, Black & White, Body and Soul in American MusicVon EverandGood Booty: Love and Sex, Black & White, Body and Soul in American MusicBewertung: 3.5 von 5 Sternen3.5/5 (7)
- Made-Up: A True Story of Beauty Culture under Late CapitalismVon EverandMade-Up: A True Story of Beauty Culture under Late CapitalismBewertung: 3.5 von 5 Sternen3.5/5 (3)
- In the Form of a Question: The Joys and Rewards of a Curious LifeVon EverandIn the Form of a Question: The Joys and Rewards of a Curious LifeBewertung: 4.5 von 5 Sternen4.5/5 (8)
- Last Night at the Viper Room: River Phoenix and the Hollywood He Left BehindVon EverandLast Night at the Viper Room: River Phoenix and the Hollywood He Left BehindBewertung: 3.5 von 5 Sternen3.5/5 (48)
- Don't Panic: Douglas Adams and the Hitchhiker's Guide to the GalaxyVon EverandDon't Panic: Douglas Adams and the Hitchhiker's Guide to the GalaxyBewertung: 4 von 5 Sternen4/5 (488)
- How to Slowly Kill Yourself and Others in America: EssaysVon EverandHow to Slowly Kill Yourself and Others in America: EssaysBewertung: 5 von 5 Sternen5/5 (12)
- Sex and the City and Us: How Four Single Women Changed the Way We Think, Live, and LoveVon EverandSex and the City and Us: How Four Single Women Changed the Way We Think, Live, and LoveBewertung: 4.5 von 5 Sternen4.5/5 (22)