Das könnte Ihnen auch gefallen
- The Complete Photo Guide To Great SexDokument175 SeitenThe Complete Photo Guide To Great Sexstillaire40% (5)
- Goddess Kali: The Black MagickianDokument59 SeitenGoddess Kali: The Black MagickianJane PauNoch keine Bewertungen
- TipologiiiiiDokument88 SeitenTipologiiiiiminodoraNoch keine Bewertungen
- Unstoppable ConfidenceDokument48 SeitenUnstoppable ConfidenceShriyani Datta100% (1)
- Charles Tart - Sex, Drugs and Altered States of ConsciousnessDokument11 SeitenCharles Tart - Sex, Drugs and Altered States of ConsciousnessElianKithaNoch keine Bewertungen
- Summer SolsticeDokument5 SeitenSummer SolsticeJc QuismundoNoch keine Bewertungen
- Long-Term Consequences of Childhood Sexual Abuse by Gender of VictimDokument9 SeitenLong-Term Consequences of Childhood Sexual Abuse by Gender of VictimMalyasree BasuNoch keine Bewertungen
- The Reproductive SystemDokument5 SeitenThe Reproductive SystemPak LypNoch keine Bewertungen
- People V AlegadoDokument3 SeitenPeople V AlegadoMiguel CastricionesNoch keine Bewertungen
- Attitudes Toward Sex and Relationships. The Second Australian Study of Health and RelationshipsDokument9 SeitenAttitudes Toward Sex and Relationships. The Second Australian Study of Health and Relationshipsfelipegonzalezfg1Noch keine Bewertungen
- RA 7610 PowerpointDokument112 SeitenRA 7610 PowerpointRomeo Belmonte Hugo93% (15)
- The University of Chicago Press American Historical AssociationDokument3 SeitenThe University of Chicago Press American Historical AssociationFernando SuarezNoch keine Bewertungen
- My Mother Liked To Fuck Joan Nestle: Mother Was Shameless, A Word Our Shame-Ridden Culture Still Uses As ADokument3 SeitenMy Mother Liked To Fuck Joan Nestle: Mother Was Shameless, A Word Our Shame-Ridden Culture Still Uses As AJane LiuNoch keine Bewertungen
- Future DirectionsDokument5 SeitenFuture DirectionsMark ElbenNoch keine Bewertungen
- Nurse Practitioners' Knowledge, Attitudes, and Self-Efficacy For Working With Transgender PatientsDokument8 SeitenNurse Practitioners' Knowledge, Attitudes, and Self-Efficacy For Working With Transgender PatientsJeresse Jeah RecaforteNoch keine Bewertungen
- Jurnal KesproDokument44 SeitenJurnal KesproFani PranidasariNoch keine Bewertungen
- A Survey of Nursing Students' Knowledge of and Attitudes Toward LGBT Health Care ConcernsDokument3 SeitenA Survey of Nursing Students' Knowledge of and Attitudes Toward LGBT Health Care ConcernsJeresse Jeah RecaforteNoch keine Bewertungen
- Concept Paper: The Effect of Discrimination On The LGBT CommunityDokument3 SeitenConcept Paper: The Effect of Discrimination On The LGBT CommunityjhadeacuinbrazaNoch keine Bewertungen
- Physicians' Use of Inclusive Language During Teen VisitsDokument9 SeitenPhysicians' Use of Inclusive Language During Teen VisitsTherese Berina-MallenNoch keine Bewertungen
- CHAP 2 DRAFTDokument3 SeitenCHAP 2 DRAFTJess JessNoch keine Bewertungen
- Nursing Students' Attitudes Toward Lesbian, Gay, Bisexual, and Transgender Persons An Integrative ReviewDokument9 SeitenNursing Students' Attitudes Toward Lesbian, Gay, Bisexual, and Transgender Persons An Integrative ReviewJeresse Jeah RecaforteNoch keine Bewertungen
- PSYC6213 Final Paper NotesDokument14 SeitenPSYC6213 Final Paper NotesMiryam MNoch keine Bewertungen
- Change in Attitudes of Indian Population About HomosexualityDokument36 SeitenChange in Attitudes of Indian Population About HomosexualityHarshi KumarNoch keine Bewertungen
- I Am Yet To Encounter Any Survey That Actually Reflects My Life A Qualitative Study of Inclusivity in Sexual Health ResearchDokument10 SeitenI Am Yet To Encounter Any Survey That Actually Reflects My Life A Qualitative Study of Inclusivity in Sexual Health Researchcallisto69Noch keine Bewertungen
- Lesbian, Gay, Bisexual, and Transgender Older Adults ' Experiences With Elder Abuse and NeglectDokument8 SeitenLesbian, Gay, Bisexual, and Transgender Older Adults ' Experiences With Elder Abuse and NeglectKimberlyn CustodioNoch keine Bewertungen
- N32_revDokument8 SeitenN32_revCristianCorreaNoch keine Bewertungen
- Sexuality in People With Intellectual DisabilityDokument18 SeitenSexuality in People With Intellectual DisabilityAlbaNoch keine Bewertungen
- Youth Violence Research PaperDokument4 SeitenYouth Violence Research Paperafmcgebln100% (1)
- 2 Imrad ResearchDokument15 Seiten2 Imrad Researchninyawenceslao4Noch keine Bewertungen
- Perspect Sex Reprod Health 23 55 49Dokument13 SeitenPerspect Sex Reprod Health 23 55 49natalia barriosNoch keine Bewertungen
- Life Satisfaction and Mental Health Among Transgender Students in NorwayDokument11 SeitenLife Satisfaction and Mental Health Among Transgender Students in NorwayMuhammad Usman KhanNoch keine Bewertungen
- Sexual Violence Victimization of Youth andDokument10 SeitenSexual Violence Victimization of Youth andhussi.musajiNoch keine Bewertungen
- It's Cool To Care About Sexual Violence''Dokument19 SeitenIt's Cool To Care About Sexual Violence''Raul LimaNoch keine Bewertungen
- Article Critique 1 - Christina Marquez 007394927Dokument6 SeitenArticle Critique 1 - Christina Marquez 007394927api-643006925Noch keine Bewertungen
- 2020 Article 323Dokument13 Seiten2020 Article 323Sarra TekayaNoch keine Bewertungen
- Autism and Adult Sex Education: A Literature Review Using The Information-Motivation-Behavioral Skills FrameworkDokument13 SeitenAutism and Adult Sex Education: A Literature Review Using The Information-Motivation-Behavioral Skills FrameworkMaria Julia Lopes NigroNoch keine Bewertungen
- 12889_2021_Article_10386Dokument9 Seiten12889_2021_Article_10386Afifah Az-ZahraNoch keine Bewertungen
- Body Image Impacts Risky Behavior in Youth with HIVDokument6 SeitenBody Image Impacts Risky Behavior in Youth with HIVMorrison Omokiniovo Jessa SnrNoch keine Bewertungen
- Kidd - Severe Mental Illness in LGBT PopulationsDokument5 SeitenKidd - Severe Mental Illness in LGBT PopulationsEmildre CampinsNoch keine Bewertungen
- Argument AnalysisDokument6 SeitenArgument AnalysisEvangelist Stephen NziokaNoch keine Bewertungen
- CheeeeDokument9 SeitenCheeeeNet Chee AlampayNoch keine Bewertungen
- What I Have LearnedDokument14 SeitenWhat I Have LearnedALLAN JUNTILLNoch keine Bewertungen
- A Rights-Based Sexuality Education Curriculum For Adolescents 1-Year Outcomes From A Cluster-Randomized TrialDokument8 SeitenA Rights-Based Sexuality Education Curriculum For Adolescents 1-Year Outcomes From A Cluster-Randomized TrialBETINA PAULEE CIPRIANONoch keine Bewertungen
- Gender IdentityDokument14 SeitenGender IdentityHemang ANoch keine Bewertungen
- Limitation of The StudyDokument13 SeitenLimitation of The StudyMuwaga Musa MNoch keine Bewertungen
- A Systematic Review of Associations Among Religiosity Spirituality and Adolescent Health Attitudes and BehaviorsDokument10 SeitenA Systematic Review of Associations Among Religiosity Spirituality and Adolescent Health Attitudes and BehaviorsFrancesco MarquinaNoch keine Bewertungen
- Perspectivas de Estudiantes de Medicina Sobre Interacción Con Industria FarmacéuticaDokument5 SeitenPerspectivas de Estudiantes de Medicina Sobre Interacción Con Industria FarmacéuticapsychforallNoch keine Bewertungen
- Literature Review On Juvenile RecidivismDokument8 SeitenLiterature Review On Juvenile Recidivismelfgxwwgf100% (1)
- Perceptions of Sex Education Among Secondary Teachers in BelizeDokument12 SeitenPerceptions of Sex Education Among Secondary Teachers in BelizeINP PAINNoch keine Bewertungen
- 2019 Addressing Sexuality Among People Living With Chronic Di 2020 Archives of PHDokument12 Seiten2019 Addressing Sexuality Among People Living With Chronic Di 2020 Archives of PHAngie OvandoNoch keine Bewertungen
- Ageism, Healthy Life Expectancy and Population Ageing: How Are They Related?Dokument11 SeitenAgeism, Healthy Life Expectancy and Population Ageing: How Are They Related?Betsabé CastroNoch keine Bewertungen
- Journal of Dental Education - 2017 - Feng - Dental Students Knowledge of Resources For LGBT Persons Findings From ThreeDokument7 SeitenJournal of Dental Education - 2017 - Feng - Dental Students Knowledge of Resources For LGBT Persons Findings From ThreeRodrigo Otávio MorettiNoch keine Bewertungen
- Transgender Research PaperDokument4 SeitenTransgender Research Papervehysad1s1w3100% (1)
- Chapter 1Dokument11 SeitenChapter 1James Lao TapiaNoch keine Bewertungen
- Relationships, Love and Sexuality: What The Filipino Teens Think and FeelDokument13 SeitenRelationships, Love and Sexuality: What The Filipino Teens Think and FeelVitas VitalyNoch keine Bewertungen
- Student DevelopmentDokument5 SeitenStudent DevelopmentTejash PanchalNoch keine Bewertungen
- Abordagem Do Paciente Psiquiatrico Pelo ClínicoDokument24 SeitenAbordagem Do Paciente Psiquiatrico Pelo ClínicoCintia AndradeNoch keine Bewertungen
- Research Paper Final DraftDokument10 SeitenResearch Paper Final Draftapi-464020532Noch keine Bewertungen
- 10.1007@s10803 020 04399 2Dokument7 Seiten10.1007@s10803 020 04399 2Krol AmafoNoch keine Bewertungen
- Problems Faced by Children in School and Counselors RoleDokument10 SeitenProblems Faced by Children in School and Counselors RoleJoyson DsouzaNoch keine Bewertungen
- 2015-3 Abioda (Knowledge About, Attitude Towards Reproductive Health and Health Seeking Behavior of Adolescents in Iloilo City)Dokument13 Seiten2015-3 Abioda (Knowledge About, Attitude Towards Reproductive Health and Health Seeking Behavior of Adolescents in Iloilo City)gausinremeaNoch keine Bewertungen
- LGBTQ Anti-Bullying AdvocacyDokument11 SeitenLGBTQ Anti-Bullying AdvocacyJosephCerniglia100% (2)
- Not All Patiens Want To ParticipateDokument5 SeitenNot All Patiens Want To ParticipateAmelia ArnisNoch keine Bewertungen
- Research Paper Chapter 1Dokument9 SeitenResearch Paper Chapter 1Sherene UmpiaNoch keine Bewertungen
- Research Paper Chapter 1-2Dokument16 SeitenResearch Paper Chapter 1-2Sherene UmpiaNoch keine Bewertungen
- Interpersonal Violence and Mental Health: New Findings and Paradigms For Enduring ProblemsDokument4 SeitenInterpersonal Violence and Mental Health: New Findings and Paradigms For Enduring ProblemsDewi NofiantiNoch keine Bewertungen
- Sexual Behaviors, Relationships, and Perceived Health Among Adult Men in The United States: Results From A National Probability SampleDokument14 SeitenSexual Behaviors, Relationships, and Perceived Health Among Adult Men in The United States: Results From A National Probability Samplescribd_com3286Noch keine Bewertungen
- Chapter 2 RDokument23 SeitenChapter 2 RJasper R. CastroverdeNoch keine Bewertungen
- Brief TherapyDokument11 SeitenBrief TherapyThomas kyengeNoch keine Bewertungen
- DEMOCRATS versus REPUBLICANS: Research on the Behaviors of High School StudentsVon EverandDEMOCRATS versus REPUBLICANS: Research on the Behaviors of High School StudentsNoch keine Bewertungen
- About HomosexualityDokument25 SeitenAbout HomosexualityVlad DenisaaNoch keine Bewertungen
- Tutor-Assessed Task 1: Slices of Homemade Bread With Pats of Fresh Butter, and Pieces of Pumpkin Pie For DessertDokument7 SeitenTutor-Assessed Task 1: Slices of Homemade Bread With Pats of Fresh Butter, and Pieces of Pumpkin Pie For DessertVlad DenisaaNoch keine Bewertungen
- DissertationDokument101 SeitenDissertationVlad Denisaa100% (1)
- Lista Colaboratori - RecomandariDokument4 SeitenLista Colaboratori - RecomandariVlad DenisaaNoch keine Bewertungen
- Lista Colaboratori - RecomandariDokument4 SeitenLista Colaboratori - RecomandariVlad DenisaaNoch keine Bewertungen
- Chapter 1 Powerpoint For Invitation To The Lifespan by BergerDokument62 SeitenChapter 1 Powerpoint For Invitation To The Lifespan by Bergermusic20102011100% (1)
- Knight, Angela - The VampdomDokument8 SeitenKnight, Angela - The VampdomLaviniaNoch keine Bewertungen
- People Vs PanchoDokument17 SeitenPeople Vs PanchoAngel AmarNoch keine Bewertungen
- Subjective Reactions To First Coitus in Relation To Participant Sex, - Bruce RindDokument19 SeitenSubjective Reactions To First Coitus in Relation To Participant Sex, - Bruce RindLaurent BronsNoch keine Bewertungen
- Doctoring - Horacio QuirogaDokument10 SeitenDoctoring - Horacio QuirogaRaquel Solano RuízNoch keine Bewertungen
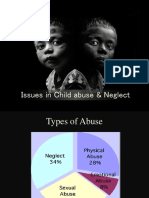
- Issues in Child Abuse & NeglectDokument28 SeitenIssues in Child Abuse & NeglectAmrutha KrishnanNoch keine Bewertungen
- Puberty: Arshiya Sultana Lecturer, Dept. of Obstetrics & Gynaecology NIUM, Bangalore, KarnatakaDokument63 SeitenPuberty: Arshiya Sultana Lecturer, Dept. of Obstetrics & Gynaecology NIUM, Bangalore, KarnatakamickageliNoch keine Bewertungen
- Sixfold Vedha Diksha InitiationsDokument2 SeitenSixfold Vedha Diksha InitiationsVenkateswaran KrishnamurthyNoch keine Bewertungen
- Population Composition and Sex Ratios ExplainedDokument20 SeitenPopulation Composition and Sex Ratios ExplainedAlga BijuNoch keine Bewertungen
- SordariaDokument31 SeitenSordariaapi-251288828Noch keine Bewertungen
- The Education of Alice WellsDokument755 SeitenThe Education of Alice WellsGeorgiana Dorojan67% (3)
- Larval development and biometry of fairy shrimp cystsDokument10 SeitenLarval development and biometry of fairy shrimp cystsBeatriz López SánchezNoch keine Bewertungen
- PP vs. PoculanDokument16 SeitenPP vs. PoculanchellychavezNoch keine Bewertungen
- Care To Be Aware: " A Single Pleasure Is Not Worth Your Future." A Campaign Awareness For Pre-Marital Sex and Early PregnanciesDokument3 SeitenCare To Be Aware: " A Single Pleasure Is Not Worth Your Future." A Campaign Awareness For Pre-Marital Sex and Early PregnanciesMariella Rose BenitoNoch keine Bewertungen
- Top 10 Most Communicable DiseasesDokument6 SeitenTop 10 Most Communicable DiseasesRaymund ArcosNoch keine Bewertungen
- General Biology 2 NotesDokument17 SeitenGeneral Biology 2 NotesAlyssa Mae BinoNoch keine Bewertungen
- Examining The Relationship Between Connection Rituals and Marital PDFDokument92 SeitenExamining The Relationship Between Connection Rituals and Marital PDFMa. Gemma Roxas-RojalesNoch keine Bewertungen
- The Role of Masturbation in HealthyDokument12 SeitenThe Role of Masturbation in HealthyprabhaNoch keine Bewertungen
- Syllabus FSEM11Dokument7 SeitenSyllabus FSEM11kinoglazNoch keine Bewertungen
- ProstitutionDokument13 SeitenProstitutionAnonymous gABfkMUGS100% (1)