Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Investigations (Gout) : 1 Tests To OrderDokument2 SeitenInvestigations (Gout) : 1 Tests To OrderRajDarvelGillNoch keine Bewertungen
- Pigmentation Disorders: Medicine, Elsevier, China, Pp. 1295-1296Dokument1 SeitePigmentation Disorders: Medicine, Elsevier, China, Pp. 1295-1296RajDarvelGillNoch keine Bewertungen
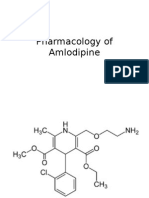
- Pharmacology of AmlodipineDokument6 SeitenPharmacology of AmlodipineRajDarvelGillNoch keine Bewertungen
- Anatomy of Pituitary GlandDokument8 SeitenAnatomy of Pituitary GlandRajDarvelGillNoch keine Bewertungen
- Panel Discussion Maternal and Child Health Improved in Urban SettingDokument4 SeitenPanel Discussion Maternal and Child Health Improved in Urban SettingRajDarvelGillNoch keine Bewertungen
- Treatment & Management: Antithyroid DrugsDokument3 SeitenTreatment & Management: Antithyroid DrugsRajDarvelGillNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- An Examination of The Effect of Product Performance On Brand Reputation, Satisfaction and LoyaltyDokument17 SeitenAn Examination of The Effect of Product Performance On Brand Reputation, Satisfaction and Loyaltyjoannakam0% (1)
- 5 D Earthsoft Personality Development Practical File 4Dokument111 Seiten5 D Earthsoft Personality Development Practical File 4Rajendra Rakhecha100% (1)
- Attitudes of Audience Towards Repeat Advertisements A Case of Pepsi AdsDokument4 SeitenAttitudes of Audience Towards Repeat Advertisements A Case of Pepsi AdsDev RishabhNoch keine Bewertungen
- Cognitive DissonanceDokument11 SeitenCognitive DissonanceAnand PrasadNoch keine Bewertungen
- Integrated Advertising Promotion and Marketing Communications 7th Edition Clow Solutions Manual DownloadDokument30 SeitenIntegrated Advertising Promotion and Marketing Communications 7th Edition Clow Solutions Manual DownloadArnita Walden100% (25)
- Review 3 - KeyDokument4 SeitenReview 3 - KeyPhạm MơNoch keine Bewertungen
- DownloadDokument22 SeitenDownloadMIKAELA THERESE OBACHNoch keine Bewertungen
- Work Values and Teaching Performance of Physical Education Teachers in Secondary Schools of Central Area Districts, Division of Northern SamarDokument14 SeitenWork Values and Teaching Performance of Physical Education Teachers in Secondary Schools of Central Area Districts, Division of Northern SamarJournal of Interdisciplinary PerspectivesNoch keine Bewertungen
- Career PlateauDokument7 SeitenCareer PlateauSyaidatina Aishah0% (1)
- Attitude and MindsetDokument22 SeitenAttitude and MindsetAbdur RofiqNoch keine Bewertungen
- PornDokument38 SeitenPorncarrier lopezNoch keine Bewertungen
- Managing Individual Differences and BehaviorDokument40 SeitenManaging Individual Differences and BehaviorDyg Norjuliani100% (1)
- The Learning Process: NCM 102-HEALTH EDUCATION AY:2020-2021Dokument74 SeitenThe Learning Process: NCM 102-HEALTH EDUCATION AY:2020-2021CLARENCE REMUDARONoch keine Bewertungen
- Tugas SP Bahasa Inggris Natasya (1511080268)Dokument30 SeitenTugas SP Bahasa Inggris Natasya (1511080268)natasya979Noch keine Bewertungen
- Conflict & NegotiationDokument28 SeitenConflict & Negotiationaadis191Noch keine Bewertungen
- A Research Proposal Submitted in Partial Fulfilment of The Requirements For The Degree of Marketing ManagementDokument40 SeitenA Research Proposal Submitted in Partial Fulfilment of The Requirements For The Degree of Marketing ManagementJossi AbuleNoch keine Bewertungen
- Week 9 - Identity Contact and Intergroup Encounters. FinalDokument55 SeitenWeek 9 - Identity Contact and Intergroup Encounters. FinalTuân NguyễnNoch keine Bewertungen
- Agarwal 2009Dokument12 SeitenAgarwal 2009marufNoch keine Bewertungen
- SympathyDokument19 SeitenSympathyblazsekNoch keine Bewertungen
- Attitudes and Behaviour For TEX3701 2020Dokument13 SeitenAttitudes and Behaviour For TEX3701 2020SleepingPhantomsNoch keine Bewertungen
- Raimo Tuomela - Social Ontology - Collective Intentionality and Group Agents-Oxford University Press (2013)Dokument327 SeitenRaimo Tuomela - Social Ontology - Collective Intentionality and Group Agents-Oxford University Press (2013)Marco Fedro ImberganoNoch keine Bewertungen
- Needs Assessment in Mathematics Competencies of Grade 6 Completers PDFDokument8 SeitenNeeds Assessment in Mathematics Competencies of Grade 6 Completers PDFAldrin MatiraNoch keine Bewertungen
- L & M in Nursing - ConflictDokument26 SeitenL & M in Nursing - ConflictMichael SamaniegoNoch keine Bewertungen
- Ex The Theory of Reasoned Action-2016 Munson PDFDokument4 SeitenEx The Theory of Reasoned Action-2016 Munson PDFAlexa0% (1)
- Improving Children's Reading AttitudesDokument25 SeitenImproving Children's Reading Attitudesajitar2003Noch keine Bewertungen
- Self AwarenessDokument30 SeitenSelf AwarenessMuneeba AminNoch keine Bewertungen
- Advertising: Meaning, Definition and FunctionsDokument137 SeitenAdvertising: Meaning, Definition and FunctionsDhruv DuaNoch keine Bewertungen
- Chapter 1 MoellerDokument18 SeitenChapter 1 MoellerLuis Rosique MartinezNoch keine Bewertungen
- Employee Attitudes and Job SatisfactionDokument14 SeitenEmployee Attitudes and Job SatisfactionBobby DNoch keine Bewertungen
- Priya 2Dokument36 SeitenPriya 2gudiyaprajapati825Noch keine Bewertungen