Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Pleural EffusionsDokument41 SeitenPleural Effusionssanjivdas100% (1)
- 2013 Fluconazole Resistant Candida Albicans.22Dokument8 Seiten2013 Fluconazole Resistant Candida Albicans.22Kala SuvarnaNoch keine Bewertungen
- Surgery CssDokument13 SeitenSurgery CssNaren ShanNoch keine Bewertungen
- ACOG Abnormal Uterine Bleeding DiagnosisDokument11 SeitenACOG Abnormal Uterine Bleeding DiagnosisJimmy Crack CornsNoch keine Bewertungen
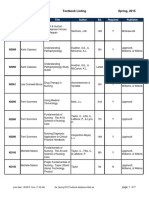
- BFLSON Course Textbook ListingDokument7 SeitenBFLSON Course Textbook ListingWina ViqaNoch keine Bewertungen
- Narayana Hrudayalaya Cardiac Hospital Case Study LessonsDokument11 SeitenNarayana Hrudayalaya Cardiac Hospital Case Study LessonsSuhaib KhanNoch keine Bewertungen
- Presentation Syntax Score TCT 2008 PDFDokument33 SeitenPresentation Syntax Score TCT 2008 PDFElla MihNoch keine Bewertungen
- 10 1097@aog 0000000000001708Dokument20 Seiten10 1097@aog 0000000000001708oodarkfireooNoch keine Bewertungen
- Thesis T3003 PDFDokument99 SeitenThesis T3003 PDFNor HidayahNoch keine Bewertungen
- MCQDokument6 SeitenMCQalirbidiNoch keine Bewertungen
- Nle Exam SamplesDokument6 SeitenNle Exam SamplesAldrich ArquizaNoch keine Bewertungen
- Pediatric Fluid and Electrolyte AlterationsDokument51 SeitenPediatric Fluid and Electrolyte AlterationsMatthew Ryan100% (1)
- LaryngoceleDokument7 SeitenLaryngoceleM Grecu CeptureanuNoch keine Bewertungen
- NCP Epidural HemDokument32 SeitenNCP Epidural HemKatrina PonceNoch keine Bewertungen
- GlossectomyDokument68 SeitenGlossectomyRohan GroverNoch keine Bewertungen
- 11 Exercises For MyopiaDokument4 Seiten11 Exercises For MyopiaarifiqNoch keine Bewertungen
- Ventilator Wave Form and InterpretationDokument59 SeitenVentilator Wave Form and InterpretationArnab SitNoch keine Bewertungen
- Medical-Surgical Questions With Rationale 70 QuestionsDokument59 SeitenMedical-Surgical Questions With Rationale 70 QuestionsJam Torres100% (7)
- Dental and Craniomaxillofacial Implant SurgeryDokument35 SeitenDental and Craniomaxillofacial Implant SurgeryJean Carlos Barbosa FerreiraNoch keine Bewertungen
- Cauda Equina Syndrome Review: Diagnosis and TreatmentDokument9 SeitenCauda Equina Syndrome Review: Diagnosis and Treatmentabelinda100% (1)
- International Journal of Health Sciences and ResearchDokument8 SeitenInternational Journal of Health Sciences and Researchrizk86Noch keine Bewertungen
- Children of Mothers With Borderline Personality Disorder (BPD)Dokument6 SeitenChildren of Mothers With Borderline Personality Disorder (BPD)curiositykillcatNoch keine Bewertungen
- Super Arrow Flex Sheath - Brochure - EN PDFDokument3 SeitenSuper Arrow Flex Sheath - Brochure - EN PDFbiomedical_com_brNoch keine Bewertungen
- 38 The Use of Meta-Analysis in Pharmacoepidemiology: Jesse A. BerlinDokument27 Seiten38 The Use of Meta-Analysis in Pharmacoepidemiology: Jesse A. BerlinFranklin garryNoch keine Bewertungen
- Reading All That Jazz - Body ClockDokument4 SeitenReading All That Jazz - Body ClockMehran EltNoch keine Bewertungen
- Case Study Acute PancreatitisDokument62 SeitenCase Study Acute PancreatitisAilyne A. CleofeNoch keine Bewertungen
- Anamnesis & PemfisDokument81 SeitenAnamnesis & PemfisFikriYTNoch keine Bewertungen
- Case Presentatio Insomnia 1Dokument49 SeitenCase Presentatio Insomnia 1kiran mahal100% (1)
- The Role of Imaging in Primary Health CareDokument28 SeitenThe Role of Imaging in Primary Health CareishkoldNoch keine Bewertungen