Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- INCB Yellow ListDokument23 SeitenINCB Yellow Listsunil_vaman_joshiNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
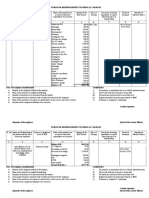
- Medical BillDokument8 SeitenMedical Billsarveshfdk48Noch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Quia Timet InjunctionDokument7 SeitenQuia Timet InjunctiondivyashekarNoch keine Bewertungen
- Czerny - Selected Pianoforte Studies - Book I - Part I & II - Edition GermerDokument106 SeitenCzerny - Selected Pianoforte Studies - Book I - Part I & II - Edition Germeryu86% (7)
- OtotoxicityDokument233 SeitenOtotoxicityGianluca Gandini100% (1)
- Mpp-Verification of Prescription OrdersDokument6 SeitenMpp-Verification of Prescription OrdersMelai Rodriguez IbardalozaNoch keine Bewertungen
- Snore Score Text 2006 Formatted PDFDokument1 SeiteSnore Score Text 2006 Formatted PDFGianluca GandiniNoch keine Bewertungen
- Snoreplasty Procedure Info PDFDokument29 SeitenSnoreplasty Procedure Info PDFGianluca GandiniNoch keine Bewertungen
- Hur Sling Snoreplasty PDFDokument1 SeiteHur Sling Snoreplasty PDFGianluca GandiniNoch keine Bewertungen
- Gradingsystembachar PDFDokument6 SeitenGradingsystembachar PDFGianluca GandiniNoch keine Bewertungen
- Gradingkoo PDFDokument5 SeitenGradingkoo PDFGianluca GandiniNoch keine Bewertungen
- Fotona Er Yag Laser Treatment of Sleep Disordered Breathing PDFDokument4 SeitenFotona Er Yag Laser Treatment of Sleep Disordered Breathing PDFGianluca GandiniNoch keine Bewertungen
- Ibuprofen - WikipediaDokument73 SeitenIbuprofen - WikipediaKishore KishoreNoch keine Bewertungen
- Fact and Comparison NGTDokument13 SeitenFact and Comparison NGTCecep Dicki HeriyandiNoch keine Bewertungen
- Prescription ModelDokument7 SeitenPrescription ModelAbhijeet PatilNoch keine Bewertungen
- Drug StudyDokument3 SeitenDrug StudyMarychen Cabunas100% (1)
- Sample Calculation Problems With AnswerDokument7 SeitenSample Calculation Problems With AnswerStephen Gabriel BongolNoch keine Bewertungen
- Patar Elementary School Fourth Periodic Test in Mapeh 6Dokument8 SeitenPatar Elementary School Fourth Periodic Test in Mapeh 6Mark Angel MorenoNoch keine Bewertungen
- AugmentinDokument7 SeitenAugmentinHeba_Al_Khozae0% (1)
- Clonazepam Drug CardDokument1 SeiteClonazepam Drug CardSheri490Noch keine Bewertungen
- WS 4 - Risani Andalasia Putri, M.Farm., Apt - PAIN MANAGEMENTDokument66 SeitenWS 4 - Risani Andalasia Putri, M.Farm., Apt - PAIN MANAGEMENTMuhammad HabibieNoch keine Bewertungen
- Wikijournalclub:List of Landmark Papers/Cardiology: HypertensionDokument5 SeitenWikijournalclub:List of Landmark Papers/Cardiology: Hypertensionrvar839Noch keine Bewertungen
- Barrier Isolator WikiDokument2 SeitenBarrier Isolator Wikiana_mondekarNoch keine Bewertungen
- Opioid Replacement Therapy Pharmacy Business Model PDFDokument76 SeitenOpioid Replacement Therapy Pharmacy Business Model PDFAbdul B. Gharaibeh0% (1)
- Question 1Dokument8 SeitenQuestion 1Camille Calcaben LongaraNoch keine Bewertungen
- Package Insert - 048437-01 - en - 422243Dokument22 SeitenPackage Insert - 048437-01 - en - 422243HadiNoch keine Bewertungen
- Dry SocketDokument10 SeitenDry SocketTomson ThomasNoch keine Bewertungen
- Shape - November 2015Dokument174 SeitenShape - November 2015alejandroneal100% (1)
- 1Dokument20 Seiten1Mervin John MercadoNoch keine Bewertungen
- Riyan Fauzan: 12100116239 Preceptor: Diana Wijayanti, DR - SP.KKDokument22 SeitenRiyan Fauzan: 12100116239 Preceptor: Diana Wijayanti, DR - SP.KKJohn BlackNoch keine Bewertungen
- End-Stage Heart DiseaseDokument44 SeitenEnd-Stage Heart DiseaseCyrille AgnesNoch keine Bewertungen
- Drug StudyDokument7 SeitenDrug StudyCandace DarleneNoch keine Bewertungen
- Metabical Pricing Case DNA Syndicate-AnswerDokument9 SeitenMetabical Pricing Case DNA Syndicate-AnswerArdha BustamiNoch keine Bewertungen
- Pediatric DentistryDokument15 SeitenPediatric DentistryPeyman Dhg100% (2)
- Skeletal Muscle Relaxants and AssociatedDokument10 SeitenSkeletal Muscle Relaxants and AssociatedMiguelNoch keine Bewertungen
- Management of Asthma: Dr. Md. Khairul Hassan JessyDokument42 SeitenManagement of Asthma: Dr. Md. Khairul Hassan JessyDr. NasrumminallahNoch keine Bewertungen
- Daftar Obat Klinik Azra: 1. Antibiotik No Nama Product KomposisiDokument11 SeitenDaftar Obat Klinik Azra: 1. Antibiotik No Nama Product KomposisiTia AgustianiNoch keine Bewertungen
- List Ubat CommonDokument4 SeitenList Ubat Commonpitjo_angin100% (1)