Das könnte Ihnen auch gefallen
- Pressure Ulcer CareDokument39 SeitenPressure Ulcer CareRosalyn YuNoch keine Bewertungen
- ABCs of Wound DebridementDokument3 SeitenABCs of Wound DebridementSheril MarekNoch keine Bewertungen
- How To Choose The Appropriate DressingDokument4 SeitenHow To Choose The Appropriate DressingDyan TD100% (1)
- DermatomyositisDokument26 SeitenDermatomyositiszaki100% (1)
- Pace Partnership Wound Care ProtocolDokument5 SeitenPace Partnership Wound Care ProtocolAmmar AlnajjarNoch keine Bewertungen
- Wound Care Giudeline NHS Bolton HospitalDokument44 SeitenWound Care Giudeline NHS Bolton HospitalJumatun Mona WarahNoch keine Bewertungen
- Wound CareDokument36 SeitenWound CareZulfadli SallehNoch keine Bewertungen
- Acute and Chronic WoundDokument18 SeitenAcute and Chronic WoundNawal FarooqNoch keine Bewertungen
- Applied Wound ManagementDokument21 SeitenApplied Wound ManagementBrian Harris100% (3)
- Burns: Major and Minor BurnsDokument25 SeitenBurns: Major and Minor BurnsTrisha TannerNoch keine Bewertungen
- Pressuread Ulcer Prevention Master ClassDokument52 SeitenPressuread Ulcer Prevention Master ClassMuhd FaiziNoch keine Bewertungen
- WoundsDokument6 SeitenWoundsTeddy MuaNoch keine Bewertungen
- Clinical Practice Guidelines 2012Dokument50 SeitenClinical Practice Guidelines 2012Immanuel Van Donn Batubara100% (1)
- Iyengar 2019Dokument13 SeitenIyengar 2019Prima BhadraNoch keine Bewertungen
- Introduction To Dermatology Assessment of A Dermatologic PatientDokument86 SeitenIntroduction To Dermatology Assessment of A Dermatologic PatientAtifNoch keine Bewertungen
- Created By:: Prof. Dr. Dr. David S. Perdanakusumah SPBPDokument1 SeiteCreated By:: Prof. Dr. Dr. David S. Perdanakusumah SPBPFivendraNoch keine Bewertungen
- McGoldrick - Infection Control Ritual To Science - Based PracticeDokument8 SeitenMcGoldrick - Infection Control Ritual To Science - Based PracticeUswaPutriemelelaNoch keine Bewertungen
- Presentation SSIDokument41 SeitenPresentation SSIJawad Mustafa100% (1)
- EndopthalmitisDokument106 SeitenEndopthalmitisGiselle EclarinoNoch keine Bewertungen
- Primary Skin LesionDokument7 SeitenPrimary Skin Lesion_carido_Noch keine Bewertungen
- Introduction To Trauma: LSU Medical Student Clerkship, New Orleans, LADokument31 SeitenIntroduction To Trauma: LSU Medical Student Clerkship, New Orleans, LAnandangNoch keine Bewertungen
- Wound Healing )Dokument14 SeitenWound Healing )miftahuldursinaNoch keine Bewertungen
- Meatotomy and Wound CareDokument13 SeitenMeatotomy and Wound CareAgung IndraNoch keine Bewertungen
- Approach To Patient With Allergic Diseases: Jovilia M. Abong, M.D. FPCP, Fpsaai, MSCDokument65 SeitenApproach To Patient With Allergic Diseases: Jovilia M. Abong, M.D. FPCP, Fpsaai, MSCCristinaConcepcionNoch keine Bewertungen
- Srinadh Neonatal Skin Conditions FinalDokument110 SeitenSrinadh Neonatal Skin Conditions FinalSrinadh Pragada100% (1)
- Burn Injury and Its ManagementsDokument86 SeitenBurn Injury and Its ManagementsBaraka Sayore0% (1)
- Dermatitis DR Citra 260907Dokument56 SeitenDermatitis DR Citra 260907Adam AriwibawaNoch keine Bewertungen
- Diabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSDokument20 SeitenDiabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSPrashant LokhandeNoch keine Bewertungen
- 1 Principles of First Aid and Its PracticeDokument118 Seiten1 Principles of First Aid and Its PracticeMohamed SamyNoch keine Bewertungen
- AWMA 2011 Standards For Wound Management v2Dokument36 SeitenAWMA 2011 Standards For Wound Management v2Agung Ginanjar100% (1)
- 2008 Classification and Management of Acute WoundsDokument5 Seiten2008 Classification and Management of Acute WoundsMiguel Angel Carrasco MedinaNoch keine Bewertungen
- NPIAP Staging PosterDokument2 SeitenNPIAP Staging PosterDr. Hüseyin ŞAHİNNoch keine Bewertungen
- Wound CareDokument11 SeitenWound Carenichole9981Noch keine Bewertungen
- Adult Bradycardia Algorithm: Identify and Treat Underlying CauseDokument1 SeiteAdult Bradycardia Algorithm: Identify and Treat Underlying CausenebrasNoch keine Bewertungen
- Cutaneous Leishmaniasis: A Case StudyDokument7 SeitenCutaneous Leishmaniasis: A Case StudyIJAR JOURNALNoch keine Bewertungen
- Api Q0315Dokument68 SeitenApi Q0315Abidi HichemNoch keine Bewertungen
- Bacterial Skin Infections - Course VIIIDokument37 SeitenBacterial Skin Infections - Course VIIIAngelie PedregosaNoch keine Bewertungen
- Burn NotesDokument5 SeitenBurn NotespaulineorrNoch keine Bewertungen
- Burns: James Taclin C. Banez M.D., FPSGS, FPCSDokument48 SeitenBurns: James Taclin C. Banez M.D., FPSGS, FPCSCodillia CheongNoch keine Bewertungen
- Copy1-Wounds and Wound HealingDokument44 SeitenCopy1-Wounds and Wound Healingfodayskamara67Noch keine Bewertungen
- DermatitisDokument6 SeitenDermatitisNader SmadiNoch keine Bewertungen
- Phototherapy For Dermatologic ConditionsDokument18 SeitenPhototherapy For Dermatologic ConditionsSeth MosebyNoch keine Bewertungen
- PsoriasisDokument27 SeitenPsoriasisMishaNoch keine Bewertungen
- The Role of Skin Care As An Integral Component in The Management of Acne VulgarisDokument9 SeitenThe Role of Skin Care As An Integral Component in The Management of Acne VulgarisluthfiNoch keine Bewertungen
- Common Skin Dis WPS OfficeDokument17 SeitenCommon Skin Dis WPS OfficeJoan JumawanNoch keine Bewertungen
- Burn WoundDokument68 SeitenBurn WoundjrefkyNoch keine Bewertungen
- Chronic Wound Managment HMIDokument37 SeitenChronic Wound Managment HMIannisa edwarNoch keine Bewertungen
- Snake Bite: DR - Vemuri ChaitanyaDokument54 SeitenSnake Bite: DR - Vemuri ChaitanyaMutiara YuliantikaNoch keine Bewertungen
- Symptom Management Guidelines: Care of Malignant WoundsDokument7 SeitenSymptom Management Guidelines: Care of Malignant WoundsPatrico Rillah Setiawan100% (1)
- Presentation of Wound DressingDokument17 SeitenPresentation of Wound DressingGafur TarniNoch keine Bewertungen
- WOUND Assessment 1Dokument30 SeitenWOUND Assessment 1Yunita BudiasmitasariNoch keine Bewertungen
- WoundsDokument79 SeitenWoundsrahmanNoch keine Bewertungen
- Skin Manifestations of HIV DiseaseDokument31 SeitenSkin Manifestations of HIV Diseaselovelots1234Noch keine Bewertungen
- BURNSDokument16 SeitenBURNSRegina KadenyiNoch keine Bewertungen
- Atopic Eczema 11Dokument71 SeitenAtopic Eczema 11khola aijazNoch keine Bewertungen
- Pulmonary EmbolismDokument19 SeitenPulmonary EmbolismIbrahimNoch keine Bewertungen
- Management of Analgesia and Sedation in the Polytraumatized patientVon EverandManagement of Analgesia and Sedation in the Polytraumatized patientNoch keine Bewertungen
- Fast Facts: Dermatological Nursing: A practical guide on career pathwaysVon EverandFast Facts: Dermatological Nursing: A practical guide on career pathwaysNoch keine Bewertungen
- Dengue National Guidelines 2014Dokument55 SeitenDengue National Guidelines 2014nrhmhealthNoch keine Bewertungen
- C. Dengue Management HypotensiveShockDokument1 SeiteC. Dengue Management HypotensiveShocknrhmhealthNoch keine Bewertungen
- Revised 5x5 Matrix National Health MissionDokument2 SeitenRevised 5x5 Matrix National Health MissionnrhmhealthNoch keine Bewertungen
- D. Dengue Management CompensatedShockDokument1 SeiteD. Dengue Management CompensatedShocknrhmhealthNoch keine Bewertungen
- A. Management Dengue PatientsDokument1 SeiteA. Management Dengue PatientsnrhmhealthNoch keine Bewertungen
- Yonex Badminton Catalog 2023 ENDokument116 SeitenYonex Badminton Catalog 2023 ENnrhmhealth100% (1)
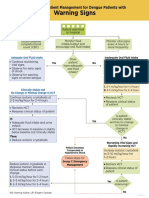
- B. Dengue Management Warning Signs InpatientDokument1 SeiteB. Dengue Management Warning Signs InpatientnrhmhealthNoch keine Bewertungen
- Standard For Female Male SterilizationDokument104 SeitenStandard For Female Male Sterilizationiman_kundu2007756Noch keine Bewertungen
- Clinical Guidance On Diabetes Management at COVID-19 Patient Management FacilityDokument14 SeitenClinical Guidance On Diabetes Management at COVID-19 Patient Management FacilitynrhmhealthNoch keine Bewertungen
- Guidelines On Clinical Management of Covid - 19Dokument15 SeitenGuidelines On Clinical Management of Covid - 19shah007zaadNoch keine Bewertungen
- Noac GuidelinesDokument40 SeitenNoac GuidelinesCocosul Cocosului CocosaruluiNoch keine Bewertungen
- Clinical Guidance On Diabetes Management at COVID-19 Patient Management FacilityDokument14 SeitenClinical Guidance On Diabetes Management at COVID-19 Patient Management FacilitynrhmhealthNoch keine Bewertungen
- Frequently Asked Questions On COVID-19 Vaccine: Target Group: General Public S. No. Potential ResponseDokument8 SeitenFrequently Asked Questions On COVID-19 Vaccine: Target Group: General Public S. No. Potential ResponseCNBCTV18 DigitalNoch keine Bewertungen
- Standard Treatment Guidelines General Surgery: Ministry of Health & Family Welfare Govt. of IndiaDokument73 SeitenStandard Treatment Guidelines General Surgery: Ministry of Health & Family Welfare Govt. of IndiaiuytrerNoch keine Bewertungen
- PPIUCD Reference Manual-Feb 2011Dokument81 SeitenPPIUCD Reference Manual-Feb 2011nrhmhealthNoch keine Bewertungen
- Blunt Chest TraumaDokument23 SeitenBlunt Chest TraumanrhmhealthNoch keine Bewertungen
- WHO - Essential Drugs PDFDokument376 SeitenWHO - Essential Drugs PDFnrhmhealthNoch keine Bewertungen
- WHO - Clinical Guidelines PDFDokument334 SeitenWHO - Clinical Guidelines PDFnrhmhealthNoch keine Bewertungen
- Pocket Book of Hospital Care For ChildrenDokument438 SeitenPocket Book of Hospital Care For ChildrenTawangNoch keine Bewertungen
- STG - Obg PDFDokument101 SeitenSTG - Obg PDFnrhmhealthNoch keine Bewertungen
- Care of The Newborn AIP Chap21Dokument30 SeitenCare of The Newborn AIP Chap21nrhmhealthNoch keine Bewertungen
- RMNCH+A 5x5 MatrixDokument1 SeiteRMNCH+A 5x5 Matrixnrhmhealth100% (2)
- 2015 Who Model List of Essential MedicinesDokument53 Seiten2015 Who Model List of Essential MedicinessallyNoch keine Bewertungen
- PCPNC BemoncDokument180 SeitenPCPNC BemoncBeryl de la CruzNoch keine Bewertungen
- Making Pregnancy Safer Safer Pregnancy in Tamil NaduDokument100 SeitenMaking Pregnancy Safer Safer Pregnancy in Tamil NaduUthayakumar KasthuriNoch keine Bewertungen
- IMCI 2011 Chart BookletDokument14 SeitenIMCI 2011 Chart BookletYam Theresa Remo100% (1)
- District Planning Tool For Maternal and Newborn Health Strategy ImplementationDokument67 SeitenDistrict Planning Tool For Maternal and Newborn Health Strategy ImplementationnrhmhealthNoch keine Bewertungen
- Who Guidelines For Safe SurgeryDokument173 SeitenWho Guidelines For Safe SurgeryAhmed M Frieg100% (1)
- Guia Reanimacion Neonatal OMSDokument61 SeitenGuia Reanimacion Neonatal OMSMarco RiveraNoch keine Bewertungen
- Vitamin K2 and Cardiovascular HealthDokument3 SeitenVitamin K2 and Cardiovascular HealthIroner'z Puroner'zNoch keine Bewertungen
- REQUEST FOR ASSESSMENT EIM NC II - Dec 19, 2020 NEW PDFDokument39 SeitenREQUEST FOR ASSESSMENT EIM NC II - Dec 19, 2020 NEW PDFChe MoralesNoch keine Bewertungen
- Dan BuettnerDokument18 SeitenDan BuettnerDaria CarutaNoch keine Bewertungen
- Hearing PresentationDokument27 SeitenHearing PresentationTaremwa PeterNoch keine Bewertungen
- Cancer Rehabilitation ENDokument298 SeitenCancer Rehabilitation ENMirjana MandićNoch keine Bewertungen
- GONORRHEADokument15 SeitenGONORRHEAVer Garcera TalosigNoch keine Bewertungen
- Pharmacy Formulary - Booklet - 2016Dokument178 SeitenPharmacy Formulary - Booklet - 2016pcartercNoch keine Bewertungen
- VA Complete RegsDokument47 SeitenVA Complete RegsTJSNoch keine Bewertungen
- Lycopodium Clavatum 30 Uses, Benefits - Lycopodium Clavatum 1m DosageDokument8 SeitenLycopodium Clavatum 30 Uses, Benefits - Lycopodium Clavatum 1m Dosagesubrat100% (1)
- Awakenings Viewing GuideDokument7 SeitenAwakenings Viewing GuidenatalieNoch keine Bewertungen
- Acute Effect of High Intensity Interval Training On Luecocytes BoutsDokument5 SeitenAcute Effect of High Intensity Interval Training On Luecocytes BoutsAhmad AlfanNoch keine Bewertungen
- Cilostazol (Pletal)Dokument4 SeitenCilostazol (Pletal)Maria Leonie Dela CruzNoch keine Bewertungen
- Parasite120019 PDFDokument8 SeitenParasite120019 PDFEka RinantoNoch keine Bewertungen
- Short Learning Topics On Biomedical Equipments by Heer Thoshani 22998Dokument55 SeitenShort Learning Topics On Biomedical Equipments by Heer Thoshani 22998Salim AloneNoch keine Bewertungen
- Healing Crystals Michael GiengerDokument99 SeitenHealing Crystals Michael Giengerjorgeblotta348995% (21)
- 1 s2.0 S2405844021020491 MainDokument10 Seiten1 s2.0 S2405844021020491 Mainambi bidullahNoch keine Bewertungen
- Chapter 10 Human DevelopmentDokument35 SeitenChapter 10 Human DevelopmentChehekNoch keine Bewertungen
- CRS and HIPEC in Patients With PC - Yang Et Al. Jgo-2019 PDFDokument15 SeitenCRS and HIPEC in Patients With PC - Yang Et Al. Jgo-2019 PDFDiego EskinaziNoch keine Bewertungen
- Maxillary Sinus Chemotherapy Extractions PDF PDFDokument4 SeitenMaxillary Sinus Chemotherapy Extractions PDF PDFAlleste OrenNoch keine Bewertungen
- 30eoct DSSSB Je-CroppedDokument46 Seiten30eoct DSSSB Je-CroppedRaj BakhtaniNoch keine Bewertungen
- Spinal StabilizationDokument32 SeitenSpinal StabilizationLakshita PrajapatiNoch keine Bewertungen
- Technological Forecasting & Social ChangeDokument19 SeitenTechnological Forecasting & Social ChangeKhoa TranNoch keine Bewertungen
- Hypoglycemia in Baby Pig-1Dokument9 SeitenHypoglycemia in Baby Pig-1sasmita100% (1)
- Ovarian CystDokument1 SeiteOvarian CystLoriene LopezNoch keine Bewertungen
- RDPL Royal Diagnostics Pvt. Ltd.Dokument6 SeitenRDPL Royal Diagnostics Pvt. Ltd.Royal Diagnostic Centre in Vaishali Nagar JaipurNoch keine Bewertungen
- RCVMHS FinalReport Vol1 AccessibleDokument704 SeitenRCVMHS FinalReport Vol1 AccessibleJulius NguyenNoch keine Bewertungen
- Evaluating The Impact of Field Epidemiology Training ProgramsDokument21 SeitenEvaluating The Impact of Field Epidemiology Training ProgramsNishtha BhawalpuriaNoch keine Bewertungen
- Maersk VN - Benefit Summary - Staff - 2020 (En)Dokument36 SeitenMaersk VN - Benefit Summary - Staff - 2020 (En)Thanh TraNoch keine Bewertungen
- Plant Derived Nootropics and Human Cognition A Systematic ReviewDokument26 SeitenPlant Derived Nootropics and Human Cognition A Systematic ReviewSubbaraju GvNoch keine Bewertungen
- Understanding Carpal Tunnel Syndrome.4Dokument8 SeitenUnderstanding Carpal Tunnel Syndrome.4ayu permata dewiNoch keine Bewertungen