Das könnte Ihnen auch gefallen
- Articles Fernand Montreuil1949 Cyst of The Nasal VestibuleDokument8 SeitenArticles Fernand Montreuil1949 Cyst of The Nasal Vestibuledieynaba baNoch keine Bewertungen
- EmpyemaDokument52 SeitenEmpyemaDivara Syauta100% (3)
- Respiratory Step 2 CK NoteDokument41 SeitenRespiratory Step 2 CK NoteXboyx MahdiNoch keine Bewertungen
- Postmedj00740 0024Dokument6 SeitenPostmedj00740 0024Danao, Aira A.Noch keine Bewertungen
- Localized EmphysemaDokument8 SeitenLocalized EmphysemaSuhartiniNoch keine Bewertungen
- Childhood Adult: Bronchiectasis in PulmonaryDokument9 SeitenChildhood Adult: Bronchiectasis in PulmonaryphobicmdNoch keine Bewertungen
- Causes of BronchopneumoniaDokument6 SeitenCauses of BronchopneumoniaSuhas Ingale100% (1)
- Case Ih Tractor Axial Flow 7230 8230 9230 Service Manual 47548079Dokument22 SeitenCase Ih Tractor Axial Flow 7230 8230 9230 Service Manual 47548079luisjimenez080687edr100% (128)
- Medical Mnemonic Sketches : Pulmonary DiseasesVon EverandMedical Mnemonic Sketches : Pulmonary DiseasesNoch keine Bewertungen
- Edinbmedj74325 0089Dokument5 SeitenEdinbmedj74325 0089anandadigdoyo44Noch keine Bewertungen
- Bronchiectasis Clinical Case SurgeryDokument9 SeitenBronchiectasis Clinical Case SurgeryChibueze AfugbuomNoch keine Bewertungen
- Prof. Koch's Method to Cure Tuberculosis Popularly TreatedVon EverandProf. Koch's Method to Cure Tuberculosis Popularly TreatedNoch keine Bewertungen
- Brmedj08338 0063Dokument6 SeitenBrmedj08338 0063api-246003035Noch keine Bewertungen
- Introduction of Tracheal Tubes by The Mouth Instead of Performing Tracheotomy or Laryngotomy.Dokument3 SeitenIntroduction of Tracheal Tubes by The Mouth Instead of Performing Tracheotomy or Laryngotomy.Pablo PradoNoch keine Bewertungen
- Pharyngeal Abscesses, Tonsillar and Adenoid InfectionsDokument36 SeitenPharyngeal Abscesses, Tonsillar and Adenoid InfectionsRon Christian Neil RodriguezNoch keine Bewertungen
- SGL6 - CoughDokument63 SeitenSGL6 - CoughDarawan MirzaNoch keine Bewertungen
- Parapneumonic Pleural Effusions and Empyema Thoracis - Background, Pathophysiology, EpidemiologyDokument4 SeitenParapneumonic Pleural Effusions and Empyema Thoracis - Background, Pathophysiology, EpidemiologyLorentina Den PanjaitanNoch keine Bewertungen
- The Lung Pathology Lab Encoded PDFDokument85 SeitenThe Lung Pathology Lab Encoded PDFJustinNoch keine Bewertungen
- On Bronchography in Cases of Purulent Lung AffectionsDokument22 SeitenOn Bronchography in Cases of Purulent Lung AffectionsAmany IbrahimNoch keine Bewertungen
- A Bronchographic Sign of Chronic: Bronchitis'Dokument4 SeitenA Bronchographic Sign of Chronic: Bronchitis'Ziyan NafisahNoch keine Bewertungen
- Allergic BronchitisDokument18 SeitenAllergic BronchitisTeresa EvansNoch keine Bewertungen
- Canmedaj00472 0105Dokument3 SeitenCanmedaj00472 0105Andre Eka Putra PrakosaNoch keine Bewertungen
- Symptoms of Respiratory DiseaseDokument70 SeitenSymptoms of Respiratory DiseaseDr-i BarreNoch keine Bewertungen
- 2.2 Pulmonary Radiology 2Dokument41 Seiten2.2 Pulmonary Radiology 2Casey Rae YanoNoch keine Bewertungen
- Uneventful, Complete,: 1933. Post-Graduate Medical JournalDokument2 SeitenUneventful, Complete,: 1933. Post-Graduate Medical JournaljabeedNoch keine Bewertungen
- Claas Mowers Disco 3600 F Disco 3500 FRC Assembly Instruction FR de en RuDokument23 SeitenClaas Mowers Disco 3600 F Disco 3500 FRC Assembly Instruction FR de en Rumarkrush140898asj100% (87)
- Manitou Access Platform 165 Atj Repair Manual 547343Dokument22 SeitenManitou Access Platform 165 Atj Repair Manual 547343kekysib100% (46)
- Test Bank For Negotiation and Dispute Resolution Beverly Demarr Suzanne de JanaszDokument24 SeitenTest Bank For Negotiation and Dispute Resolution Beverly Demarr Suzanne de JanaszMrsNicoleWarrenbkgn100% (43)
- Topic 5 Resp Syst 2016Dokument31 SeitenTopic 5 Resp Syst 2016Daniel Ashoori100% (1)
- Dr. Sana Bashir DPT, MS-CPPTDokument46 SeitenDr. Sana Bashir DPT, MS-CPPTbkdfiesefll100% (1)
- Symptoms and Signs of Respiratory Disease Lecture 2: DyspnoeaDokument9 SeitenSymptoms and Signs of Respiratory Disease Lecture 2: DyspnoeaShannon RamsumairNoch keine Bewertungen
- Textbook of Special Pathological Anatomy of Domestic AnimalsVon EverandTextbook of Special Pathological Anatomy of Domestic AnimalsNoch keine Bewertungen
- 3 Restrictive DisordersDokument26 Seiten3 Restrictive DisordersLulu MushiNoch keine Bewertungen
- Brmedj08820 0015bDokument1 SeiteBrmedj08820 0015btoreniyNoch keine Bewertungen
- (Referensi) LowelDokument8 Seiten(Referensi) LowelA. Arviani Desianti NurNoch keine Bewertungen
- California State of Medicine III, No. THE Surgical Treatment Chro-NIC Tonsillitis.Dokument2 SeitenCalifornia State of Medicine III, No. THE Surgical Treatment Chro-NIC Tonsillitis.Hendra SquidsartNoch keine Bewertungen
- Bronchiectasis OkDokument60 SeitenBronchiectasis OkImmanuelNoch keine Bewertungen
- Respiratory Exam (RCT)Dokument8 SeitenRespiratory Exam (RCT)kenners100% (31)
- Recurrent Parotitis in ChildrenDokument5 SeitenRecurrent Parotitis in ChildrenMira SharaswatiNoch keine Bewertungen
- 2 The Diagnosis of Focal Sepsis of The Nose Throat and EarDokument8 Seiten2 The Diagnosis of Focal Sepsis of The Nose Throat and EarLina WatilubisNoch keine Bewertungen
- Jnma00736 0021Dokument3 SeitenJnma00736 0021talenticaxo1Noch keine Bewertungen
- Mechanical IntubationDokument5 SeitenMechanical IntubationBAILEN AYNNA PEARLNoch keine Bewertungen
- Case Study BPNDokument9 SeitenCase Study BPNRozecarl JhoyNoch keine Bewertungen
- Lower Respiratory Disorders Part 1Dokument70 SeitenLower Respiratory Disorders Part 1Joseph Krafft100% (1)
- PneumoniaDokument66 SeitenPneumoniasamakayigrace808Noch keine Bewertungen
- Ulcer of The Stomach 9Dokument3 SeitenUlcer of The Stomach 9Ashucool65Noch keine Bewertungen
- Physician, Thoracic Unit (E.M.S.), HarefieldDokument3 SeitenPhysician, Thoracic Unit (E.M.S.), HarefieldkurniafniatiNoch keine Bewertungen
- Chest X Ray - 4Dokument64 SeitenChest X Ray - 4melindamentariNoch keine Bewertungen
- Respiration CH 43.Dr SarahDokument59 SeitenRespiration CH 43.Dr Sarahaiman siddiquiNoch keine Bewertungen
- Sistem Respirasi Sesak Napas: Problem Based LearningDokument61 SeitenSistem Respirasi Sesak Napas: Problem Based LearningAkbar IskandarNoch keine Bewertungen
- Bacterial Destruction of The LungsDokument46 SeitenBacterial Destruction of The LungsAhmad Abu KushNoch keine Bewertungen
- The Atlantic Monthly, Volume 11, No. 68, June, 1863 A Magazine of Literature, Art, and PoliticsVon EverandThe Atlantic Monthly, Volume 11, No. 68, June, 1863 A Magazine of Literature, Art, and PoliticsNoch keine Bewertungen
- CracklesDokument6 SeitenCracklesFernando Sánchez DíezNoch keine Bewertungen
- The Diseases of the Dog and Their Treatment - Containing Information on Fevers, Inflammation, Mange and Other Ailments of the DogVon EverandThe Diseases of the Dog and Their Treatment - Containing Information on Fevers, Inflammation, Mange and Other Ailments of the DogNoch keine Bewertungen
- Case Report Ruptur TrakheaDokument6 SeitenCase Report Ruptur TrakheaNurul NingrumNoch keine Bewertungen
- Lung Abscess: Presented byDokument36 SeitenLung Abscess: Presented byPalanki Gopal100% (1)
- Professor Youry Vladimirovitch PlotnicovDokument109 SeitenProfessor Youry Vladimirovitch PlotnicovOxana TulbeaNoch keine Bewertungen
- Seizstroke in ChildDokument6 SeitenSeizstroke in ChildDian Isti AngrainiNoch keine Bewertungen
- Poststroke EpilepsyDokument5 SeitenPoststroke EpilepsyDian Isti AngrainiNoch keine Bewertungen
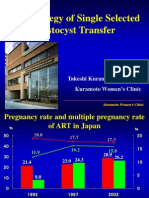
- The Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDokument43 SeitenThe Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDian Isti AngrainiNoch keine Bewertungen
- Sleeping Dif Culties in Relation To Depression and Anxiety in Elderly AdultsDokument6 SeitenSleeping Dif Culties in Relation To Depression and Anxiety in Elderly AdultsDian Isti AngrainiNoch keine Bewertungen
- Jurnal PDFDokument10 SeitenJurnal PDFNayda FitrinaNoch keine Bewertungen
- Theories of EmotionDokument11 SeitenTheories of EmotionNoman ANoch keine Bewertungen
- Understanding The School Curriculum Close Encounter With The School Curriculum SPARK Your InterestDokument12 SeitenUnderstanding The School Curriculum Close Encounter With The School Curriculum SPARK Your InterestJoshua Lander Soquita CadayonaNoch keine Bewertungen
- Sleeping GarmentsDokument1 SeiteSleeping GarmentsRosalie LazaroNoch keine Bewertungen
- Online Gaming and Social BehaviorDokument13 SeitenOnline Gaming and Social BehaviorPave Llido100% (1)
- Pearson Edexcel A Level Economics A Fifth Edition Peter Smith Full Chapter PDF ScribdDokument67 SeitenPearson Edexcel A Level Economics A Fifth Edition Peter Smith Full Chapter PDF Scribdrobert.eligio703100% (5)
- DAR Provincial Office: On-the-Job Training (OJT) Training PlanDokument3 SeitenDAR Provincial Office: On-the-Job Training (OJT) Training PlanCherry Jean MaanoNoch keine Bewertungen
- Short Question: Computer Science For 9 Class (Unit # 3)Dokument5 SeitenShort Question: Computer Science For 9 Class (Unit # 3)Yasir MehmoodNoch keine Bewertungen
- Knowledge About Visha - Upavisha & Metalic Preparations - Knowledge of Formulations Containing Visha - Upavisha & Rasa AushadhisDokument154 SeitenKnowledge About Visha - Upavisha & Metalic Preparations - Knowledge of Formulations Containing Visha - Upavisha & Rasa AushadhisPRASHNT SINGHNoch keine Bewertungen
- Eva Braun Life With Hitler PDFDokument2 SeitenEva Braun Life With Hitler PDFPamela0% (1)
- Begc133em20 21Dokument14 SeitenBegc133em20 21nkNoch keine Bewertungen
- Trabajos de InglésDokument6 SeitenTrabajos de Inglésliztmmm35Noch keine Bewertungen
- Region 2Dokument75 SeitenRegion 2yoyiyyiiyiyNoch keine Bewertungen
- Amma Vun - Bala AshtagamDokument4 SeitenAmma Vun - Bala AshtagamSHIV RAMNoch keine Bewertungen
- The Perception of Veggie Nilupak To Selected Grade 11 Students of Fort Bonifacio High SchoolDokument4 SeitenThe Perception of Veggie Nilupak To Selected Grade 11 Students of Fort Bonifacio High SchoolSabrina EleNoch keine Bewertungen
- Lesson 20 PerdevDokument7 SeitenLesson 20 PerdevIvan Joshua RemosNoch keine Bewertungen
- Essay 1 John WatsonDokument4 SeitenEssay 1 John Watsonapi-259502356Noch keine Bewertungen
- Family Advent Devotions 1Dokument3 SeitenFamily Advent Devotions 1collingdalenazNoch keine Bewertungen
- Control Work.: ..... Is A Typical ..... DishDokument4 SeitenControl Work.: ..... Is A Typical ..... DishАндрій ХомишакNoch keine Bewertungen
- Dela Cruz vs. Atty. DimaanoDokument8 SeitenDela Cruz vs. Atty. DimaanoMarga CastilloNoch keine Bewertungen
- Drishti IasDokument36 SeitenDrishti Ias23010126269Noch keine Bewertungen
- Joget Mini Case Studies TelecommunicationDokument3 SeitenJoget Mini Case Studies TelecommunicationavifirmanNoch keine Bewertungen
- MNDCS-2024 New3 - 231101 - 003728Dokument3 SeitenMNDCS-2024 New3 - 231101 - 003728Dr. Farida Ashraf AliNoch keine Bewertungen
- Derivative Pakistan PerspectiveDokument99 SeitenDerivative Pakistan PerspectiveUrooj KhanNoch keine Bewertungen
- Alb Ani A BrochureDokument18 SeitenAlb Ani A BrochurejskardaNoch keine Bewertungen
- 12 Biology CBSE Sample Papers 2018Dokument5 Seiten12 Biology CBSE Sample Papers 2018Sakshi GodaraNoch keine Bewertungen
- All This Comand Use To Type in NotepadDokument9 SeitenAll This Comand Use To Type in NotepadBiloul ShirazNoch keine Bewertungen
- Islamic Architecture PDFDokument59 SeitenIslamic Architecture PDFHarshi Garg100% (3)
- IEEE 802.1adDokument7 SeitenIEEE 802.1adLe Viet HaNoch keine Bewertungen
- Kinematic Tool-Path Smoothing For 6-Axis Industrial Machining RobotsDokument10 SeitenKinematic Tool-Path Smoothing For 6-Axis Industrial Machining RobotsToniolo LucaNoch keine Bewertungen
- Vocab Money HeistDokument62 SeitenVocab Money HeistCivil EngineeringNoch keine Bewertungen