IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 2 Ver. III (Feb. 2015), PP 44-46
www.iosrjournals.org
Giant Porokeratosis of Mibelli with Squamous Cell Carcinomas
Vani. T, Ramamohan. Ch, Nageswaramma. S, Swarnakumari. G, V
Sivaramakrishna. T , Rajunaidu. D.S, Swapna K, Ramadas N
Department of Dermatology Venereology Leprology, Department of Radiotherapy
Guntur medical college, Guntur.
Abstract: Porokeratosis is a specific disorder of keratinization that has five major clinical types and shows a
characteristic cornoid lamella on histopathology. Giant porokeratosis is considered to be a morphological
variant of porokeratosis of mibelli. Malignant degeneration has been described in all forms of porokeratosis but
highest risk is associated with linear and giant porokeratosis . We report a case of giant porokeratosis with
squamous cell carcinomas in 55yr old female patient. To the best of our knowledge this is the largest giant
porokeratosis ever reported measuring 6248cm with two large squamous cell carcinomas.
Keywords: Cornoid lamellae, Giant porokeratosis of Mibelli, Malignant degeneration, Squamous cell
carcinoma, Ultraviolet Radiation.
I.
Introduction
Porokeratosis is a rare clonal disorder of keratinization, characterized clinically by atrophic patches
with a distinct ridge like border. The border has a histologic hall mark in the form of cornoid lamella - a
parakeratotic column. Various morphologic forms of porokeratosis have been described. Five major variants
among them are Porokeratosis of Mibelli(PM), Disseminated superficial actinic porokeratois(DSAP), Linear
porokeratosis(LP), Porokeratosis Palmaris et plantaris disseminate(PPPD), & Punctate porokeratosis(PP). There
are other variants like giant porokeratosis, hyperkeratotic, verrucous, nodular, punched out & reticulate type. 10
Malignant transformation into squamous, bowenoid or basal cell carcinoma has been described in all forms of
porokeratosis with the highest risk for the linear form followed by giant porokeratosis. Giant porokeratosis is
considered to be a morphological variant of porokeratosis of Mibelli with a diameter of upto 20cm.
II.
Case Report
A 55 year old female from a remote village of Andhra Pradesh, India presented with hypo and
hyperpigmented plaque on left side of the trunk (chest and back) and shoulder of 30 years duration. She is an
agriculture worker. The lesion started as a papule on upper back which was asymptomatic. The lesion gradually
increased in size and extended on to the left shoulder and chest. There is no history of taking any treatment.
She developed two ulcerated growths (cauliflower like as described by patient), one on the back of two
years duration and the other on the chest of one year duration on previously existing lesion. Patient developed
mild irritation and pain for which she took some symptomatic treatment. There is no similar complaint in the
family. Cutaneous examination revealed a plaque of size 6248 cms on the back extending up to the lower
end of the rib cage on left side crossing the midline, in front extending on to the breast and left arm up to the
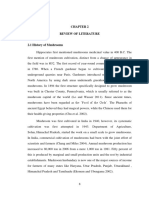
elbow with central atrophy and well demarcated hyperkeratotic border with a groove in centre. Two ulcerated
masses are present of size 126 cms on left side of chest and 1410 cms in upper back . [Fig. 1,2]
Fig 1 : annular plaque with keratotic border and atrophic centre with sqaumous cell carcinoma on chest and
upper arm
DOI: 10.9790/0853-14234446
www.iosrjournals.org
44 | Page
Giant Porokeratosis Of Mibelli With Squamous Cell Carcinomas
Fig 2: cauliflower like growth on the back on large atrophic plaque with hyperkeratotic border
Routine blood tests, X-ray chest and ultrasound abdomen were unremarkable. Elisa test for HIV was
non reactive.
Histopathology from the border of plaque showed hyperkeratosis and a column of parakeratotic cells
- characteristic cornoid lamellae in epidermal invagination and absent granular layer below it which is
consistent with porokeratosis of Mibelli. [Fig 3] Upper dermis showed chronic inflammatory cell infiltrate.
Histopathology of ulcerated masses revealed well differentiated squamous cell carcinoma with characteristic
malignant pearls. [Fig 4]
fig 3: hyperkeratosis, parakeratosis, cornoid lamella in the epidermal invagination and absent granular layer
below the cornoid lamella
Fig 4: well differentiated horn pearls
After confirming the diagnosis of giant porokeratosis with squamous cell carcinoma patient was
referred to radiotherapy department for the management of squamous cell carcinoma.
III.
Discussion
Porokeratosis is a rare disorder of keratinization with autosomal dominant mode of inheritance with
sporadic cases known to occur frequently. There is a predilection for the male sex. Various risk factors involved
in the development of porokeratosis include genetic inheritance, 11 immunosuppression,(11,12) UV radiation and
DOI: 10.9790/0853-14234446
www.iosrjournals.org
45 | Page
Giant Porokeratosis Of Mibelli With Squamous Cell Carcinomas
sun exposure.11 It was first described by Mibelli in 1893 based on the assumption that the columns of
parakeratosis emerge from the ostia of eccrine ducts.2 Porokeratosis is clinically characterized by asymptomatic
or mild pruritic keratotic papules surrounded by a raised keratotic border. Among the five classical clinical
variants, Porokeratosis of Mibelli has the characteristic morphological features as annular plaques with central
atrophy and elevated keratotic borders containing a longitudinal furrow. Giant porokeratosis is considered to be
a morphological variant of porokeratosis of Mibelli by some authors while others consider it as a distinct entity.
The lesions may vary from 10 to 20cm in diameter & the hypekeratotic walls raised greater than 1cm. 4
Malignancy although rare, has been reported in almost all forms of porokeratosis. The factors associated with a
higher risk of malignant transformation include; duration & size of the lesions, age of the patient, large lesions
on the extremity, linear type13 & multiple patterns of porokeratosis.7
The risk for malignant transformation of porokerotosis of Mibelli has been reported to be 7.5 to 11%.7
Squamous cell carcinoma is the most commonly reported malignancy in porokeratosis, and other malignancies
reported are Bowens disease, Basal cell carcinoma and Diffuse Large B cell Lymphoma.5
In this case, patient had some potential risk factors such as her age, long duration of the lesion, large
size, sun exposure (as she is a agricultural worker) all of which strongly justify the conversion to squamous cell
carcinoma.
Several large lesions of Porokeratosis of Mibelli have been reported as giant ones 10 cms diameter;7
1312 cms;4 1410 cms3, 1813 cms6 ; 2550 cms1. Our presenting case measured 6248 cms, largest giant
porokeratosis ever reported to the best of our knowledge with large squamous cell carcinomas which is
extremely rare.
IV.
Conclusion
We conclude that the patients with long standing and large lesions of porokeratosis have high risk of
malignant transformation hence should be monitored regularly to detect malignant changes.
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
[11].
[12].
[13].
Ehsani AH, Shakoei S, Ranjabar M. Giant Porkeratosis of Mibelli with Squamous Cell Carcinoma. Indian J Dermatology
Venereology Leprology 2014; 80: 96-7
Rifaioglu EN, Ozyalvacli G. Follicular Porokeratosis at Alae nasi; A case report and short review of literture. Indian J Dermatology
2014; 59: 398-400
Mohanan Saritha, Rashmi Kumari, Devinder Thappa, Nachiappa G. Rajesh, Surendra Kumar Verma. Benign giant cutaneous horn
formed by giant Porokeratosis of Mibelli with dysplasia . Indian J Dermatology Venereology Leprology 2013; 79: 433-35
Ray Chaudary T, Valsamma DP. Giant Porokeratosis, . Indian J Dermatology Venereology Leprology 2011; 77: 601-2
Sarma N, Boler AK, Bhattachrya SR. Familial Disseminated plaque type Porokeratosis with multiple horns and Squamous cell
carcinoma involving anal skin; Indian J Dermatology Venereology Leprology 2009; 75: 551
Ma DL, Vano-Galvan S. Squamous cell carcinoma arising from Giant Porokeratosis. Dermatol. Surg 2009; 35: 1999-2000
Senguptha S, Das JK, Gangopadhyay. A multicentric squamous cell carcinoma over lesions of Porokeratosis Pamaris et plantaris
disseminate an giant Porokeratosis. Indian J Dermatology Venereology Leprology 2005; 71: 414-6
Vasudevan B, Chatterjee M, Grewal R, Rana V, Lodha N. A case of disseminated superficial Porokeratosis associated with giant
Porokeratosis in pregnancy. Indian J Dermatol 2014; 59: 492-4.
Pavithran K, Disorders of keratinisation. In: Valia RG, Valia AR, editors. IADVL Txtbook and Atlas of Dermatology. 2 nd ed.
Mumbai: Balani Publishing house; 2001. P 805-6.
Palleschi GM, Torchia D, Porokeratosis of Mibelli and superficial disseminated porokeratosis. J Cutan Pathol 2008; 35: 253-5.
Odeyinde S, Belcher H. Isolated single porokeratosis mibelli: An unusual case. Dermatol online J 2012; 18:13
Perez-Crespo M,. Betloch I, Lucas Costa A, Banuls-Roca J, Niveiro de Jaime M, Mataix J. Unusual evolution of giant
porokeratosis developing in two renal transplant patients. Int J Dermatol 2008;47:59-60
Sasson M, Krain AD. Porokeratosis and cutaneous malignancy. A review . Dermatol Surg 1996;22:339-42.
DOI: 10.9790/0853-14234446
www.iosrjournals.org
46 | Page
Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Pharmacotherapy Principles & Practice PDFDokument1.713 SeitenPharmacotherapy Principles & Practice PDFgrace fortunatus92% (51)
- Petroleum As A Cancer CureDokument4 SeitenPetroleum As A Cancer Curedaurel100% (1)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Woman S Era - June First 2016Dokument132 SeitenWoman S Era - June First 2016Amitabh PrasadNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Design and Analysis of Ladder Frame Chassis Considering Support at Contact Region of Leaf Spring and Chassis FrameDokument9 SeitenDesign and Analysis of Ladder Frame Chassis Considering Support at Contact Region of Leaf Spring and Chassis FrameInternational Organization of Scientific Research (IOSR)Noch keine Bewertungen
- Carcinosin SCDokument10 SeitenCarcinosin SCnitkolNoch keine Bewertungen
- Medstar ObGyn 2nd EditionDokument570 SeitenMedstar ObGyn 2nd EditionMerahit Abera100% (2)
- 23 Benefits and Uses For Baking SodaDokument18 Seiten23 Benefits and Uses For Baking SodabrightstarNoch keine Bewertungen
- Youth Entrepreneurship: Opportunities and Challenges in IndiaDokument5 SeitenYouth Entrepreneurship: Opportunities and Challenges in IndiaInternational Organization of Scientific Research (IOSR)100% (1)
- Unseen Trends in Biotechnology-Part1Dokument100 SeitenUnseen Trends in Biotechnology-Part1Shourya17Noch keine Bewertungen
- IHFG Part B Oncology Medical ChemotherapyDokument20 SeitenIHFG Part B Oncology Medical ChemotherapyFransiska OktavianiNoch keine Bewertungen
- Effects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaDokument10 SeitenEffects of Formative Assessment On Mathematics Test Anxiety and Performance of Senior Secondary School Students in Jos, NigeriaInternational Organization of Scientific Research (IOSR)100% (1)
- Factors Affecting Success of Construction ProjectDokument10 SeitenFactors Affecting Success of Construction ProjectInternational Organization of Scientific Research (IOSR)Noch keine Bewertungen
- Necessary Evils of Private Tuition: A Case StudyDokument6 SeitenNecessary Evils of Private Tuition: A Case StudyInternational Organization of Scientific Research (IOSR)Noch keine Bewertungen
- Comparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockDokument2 SeitenComparison of Explosive Strength Between Football and Volley Ball Players of Jamboni BlockInternational Organization of Scientific Research (IOSR)Noch keine Bewertungen
- Design and Analysis of An Automotive Front Bumper Beam For Low-Speed ImpactDokument11 SeitenDesign and Analysis of An Automotive Front Bumper Beam For Low-Speed ImpactInternational Organization of Scientific Research (IOSR)Noch keine Bewertungen
- Fatigue Analysis of A Piston Ring by Using Finite Element AnalysisDokument4 SeitenFatigue Analysis of A Piston Ring by Using Finite Element AnalysisInternational Organization of Scientific Research (IOSR)Noch keine Bewertungen
- Pyrexia of Unknown OriginDokument81 SeitenPyrexia of Unknown OriginJithin Bhagavati Kalam100% (1)
- Tumori Fibrohistiocitare IntermediareDokument39 SeitenTumori Fibrohistiocitare IntermediareOana BarbuNoch keine Bewertungen
- Template Continued On Page 2: Indication: References: NCCN Supportive CareDokument2 SeitenTemplate Continued On Page 2: Indication: References: NCCN Supportive CareJaneNoch keine Bewertungen
- HPV QUANT-21 - Form A6 - Specification of ProductDokument4 SeitenHPV QUANT-21 - Form A6 - Specification of ProductLAB PCRNoch keine Bewertungen
- Physical CarcinogenesisDokument3 SeitenPhysical CarcinogenesisamaraadhithiyaNoch keine Bewertungen
- Hospitals Initiating CoverageDokument23 SeitenHospitals Initiating CoverageAshutosh GuptaNoch keine Bewertungen
- ReishiMax Clinical StudyDokument7 SeitenReishiMax Clinical StudynsagelocspaNoch keine Bewertungen
- Chapter II PDFDokument14 SeitenChapter II PDFjudyline ariolaNoch keine Bewertungen
- LESSON PLAN Rungal 2Dokument31 SeitenLESSON PLAN Rungal 2astha singhNoch keine Bewertungen
- Tagrisso Epar Medicine Overview - enDokument3 SeitenTagrisso Epar Medicine Overview - enPreet ShethNoch keine Bewertungen
- Alcohol MetabolismDokument12 SeitenAlcohol Metabolismjames100% (1)
- Conjunctival Pigmented LesionsDokument0 SeitenConjunctival Pigmented LesionsBhartendu Agarwal0% (1)
- CholangiocarcinomaDokument9 SeitenCholangiocarcinomaloloalpsheidiNoch keine Bewertungen
- Sunlight Robbery Vitamin D 0liver GillieDokument19 SeitenSunlight Robbery Vitamin D 0liver Gillieashlei32Noch keine Bewertungen
- CNS Tumor Map 2020 FullDokument1 SeiteCNS Tumor Map 2020 FullAlves de MeloNoch keine Bewertungen
- 1recent ExamsDokument42 Seiten1recent Examsfamilymedicine1234Noch keine Bewertungen
- 28 11 2019 8th Aitong Medical Camp ReportDokument26 Seiten28 11 2019 8th Aitong Medical Camp ReportStacy NeetNoch keine Bewertungen
- Active Ingredients PomegranateDokument91 SeitenActive Ingredients Pomegranatekennitaharyati100% (1)
- 7 Safety Health Probs WorkplaceDokument2 Seiten7 Safety Health Probs WorkplaceazerNoch keine Bewertungen
- BAGIC Group Mediclaim - BrochureDokument38 SeitenBAGIC Group Mediclaim - BrochureVisakh MahadevanNoch keine Bewertungen
- IMRT & Stereotactic Radiotherapy: Christopher GolbyDokument41 SeitenIMRT & Stereotactic Radiotherapy: Christopher GolbyAmr MuhammedNoch keine Bewertungen
- Care of Clients With Problems in Cellular Aberrations Key TermsDokument2 SeitenCare of Clients With Problems in Cellular Aberrations Key Termsjoyrena ochondraNoch keine Bewertungen