Das könnte Ihnen auch gefallen
- SARS-CoV-2-Specific T Cell Immunity in Cases of COVID-19 and SARS, and Uninfected Controls (Le Bert 2020)Dokument21 SeitenSARS-CoV-2-Specific T Cell Immunity in Cases of COVID-19 and SARS, and Uninfected Controls (Le Bert 2020)gd_hbarNoch keine Bewertungen
- 141 Research Studies Affirm Naturally Acquired Immunity To Covid-19 (Brownstone Institute 2021)Dokument40 Seiten141 Research Studies Affirm Naturally Acquired Immunity To Covid-19 (Brownstone Institute 2021)gd_hbarNoch keine Bewertungen
- Profile of Immunoglobulin G and IgM Antibodies Against SARS-CoV-2 (Qu 2021)Dokument4 SeitenProfile of Immunoglobulin G and IgM Antibodies Against SARS-CoV-2 (Qu 2021)gd_hbarNoch keine Bewertungen
- Neuropilin-1 Facilitates SARS-CoV-2 Cell Entry and Infectivity (Cantuti-Castelvetri 2020)Dokument7 SeitenNeuropilin-1 Facilitates SARS-CoV-2 Cell Entry and Infectivity (Cantuti-Castelvetri 2020)gd_hbarNoch keine Bewertungen
- The Z-Pinch Morphology of Supernova 1987A and Electric Stars (Thornhill 2007)Dokument13 SeitenThe Z-Pinch Morphology of Supernova 1987A and Electric Stars (Thornhill 2007)gd_hbarNoch keine Bewertungen
- The Electric Wind of Venus (Collinson Et Al. 2016)Dokument9 SeitenThe Electric Wind of Venus (Collinson Et Al. 2016)gd_hbarNoch keine Bewertungen
- Electromagnetic Studies in Geothermal Regions (Berktold 1983)Dokument7 SeitenElectromagnetic Studies in Geothermal Regions (Berktold 1983)gd_hbarNoch keine Bewertungen
- How To Create A Socialist State (Saul Alinsky)Dokument1 SeiteHow To Create A Socialist State (Saul Alinsky)gd_hbar100% (2)
- Tdap Vaccine Effectiveness in Adolescents (Acosta 2017)Dokument11 SeitenTdap Vaccine Effectiveness in Adolescents (Acosta 2017)gd_hbarNoch keine Bewertungen
- Birkeland Currents in The Earth's Magnetoshpere (Potemra 1987)Dokument15 SeitenBirkeland Currents in The Earth's Magnetoshpere (Potemra 1987)gd_hbarNoch keine Bewertungen
- Ultrastructural Changes in Alveolar Epithelium in Response To Freund's Adjuvant (Faulkner & Esterly 1971)Dokument16 SeitenUltrastructural Changes in Alveolar Epithelium in Response To Freund's Adjuvant (Faulkner & Esterly 1971)gd_hbarNoch keine Bewertungen
- Security Clearance Application FormDokument8 SeitenSecurity Clearance Application Formgd_hbarNoch keine Bewertungen
- The Effect of Altitude On Relative HumidityDokument6 SeitenThe Effect of Altitude On Relative Humiditygd_hbar100% (1)
- CapecitabineDokument13 SeitenCapecitabinegd_hbar100% (1)
- Crude Manipulation by HFT AlgosDokument72 SeitenCrude Manipulation by HFT Algosgd_hbarNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Vaccination and Autoimmune Disease: What Is The Evidence?: ReviewDokument8 SeitenVaccination and Autoimmune Disease: What Is The Evidence?: Reviewtito7227Noch keine Bewertungen
- Immuno First - Past Years QsDokument48 SeitenImmuno First - Past Years QsAbdallah Essam Al-Zireeni67% (3)
- APhA Immunization Module 2Dokument12 SeitenAPhA Immunization Module 2Gerald GamboaNoch keine Bewertungen
- Activity 28 - Adaptive ImmunityDokument6 SeitenActivity 28 - Adaptive ImmunityKaren Joy MagbanuaNoch keine Bewertungen
- Immune System (Non-Specific & Specific Defences) - ANSWERDokument23 SeitenImmune System (Non-Specific & Specific Defences) - ANSWERincognitus94Noch keine Bewertungen
- Antibody Diversity:Variable Joining Sites and Somatic MutationsDokument11 SeitenAntibody Diversity:Variable Joining Sites and Somatic MutationsFemi Mega LestariNoch keine Bewertungen
- IMMUNOINFORMATICSDokument586 SeitenIMMUNOINFORMATICSAC_AderemiNoch keine Bewertungen
- Subversion of Innate and Adaptive Immune Responses by Toxoplasma GondiiDokument13 SeitenSubversion of Innate and Adaptive Immune Responses by Toxoplasma GondiiAaminnNoch keine Bewertungen
- Immunology Mcqs-4: InstructionsDokument22 SeitenImmunology Mcqs-4: InstructionsadehkordiNoch keine Bewertungen
- 12 TransplantationDokument137 Seiten12 TransplantationLee BoborasNoch keine Bewertungen
- Cell-Mediated Immune ResponsesDokument53 SeitenCell-Mediated Immune ResponsesFarahdina UmarellaNoch keine Bewertungen
- WA10015-Immune Response HIV PDFDokument1 SeiteWA10015-Immune Response HIV PDFLianceNoch keine Bewertungen
- Immunity Questions and AnswersDokument12 SeitenImmunity Questions and Answerskumara guruparanNoch keine Bewertungen
- NonClassical MHC Class I PDFDokument12 SeitenNonClassical MHC Class I PDFRobMarvinNoch keine Bewertungen
- Immunopharmacology - IntroductionDokument51 SeitenImmunopharmacology - IntroductionIsrat Jahan Surovy 2225400672Noch keine Bewertungen
- Sarcoidosis Review. JAMADokument9 SeitenSarcoidosis Review. JAMARafael ReañoNoch keine Bewertungen
- Quiz ImmunologyDokument50 SeitenQuiz ImmunologyMedShare97% (39)
- Architecture For An Artificial Immune System: Steven A. Hofmeyr Stephanie ForrestDokument33 SeitenArchitecture For An Artificial Immune System: Steven A. Hofmeyr Stephanie ForrestIfraNoch keine Bewertungen
- Immnunology Notebook Chapter One: Innate ImmunityDokument45 SeitenImmnunology Notebook Chapter One: Innate ImmunityJavier Alejandro Daza GalvánNoch keine Bewertungen
- UntitledDokument23 SeitenUntitledPravinNoch keine Bewertungen
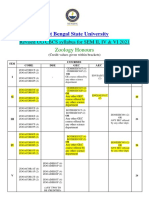
- Revised ZOOLOGY HONOURS UG CBCS Syllabus Sem II, IV, VI-editedDokument5 SeitenRevised ZOOLOGY HONOURS UG CBCS Syllabus Sem II, IV, VI-editedRidhi ChoudharyNoch keine Bewertungen
- Major Histocompatibility ComplexDokument15 SeitenMajor Histocompatibility ComplexsanasharNoch keine Bewertungen
- Immunology MCQDokument51 SeitenImmunology MCQLouise Marie Palamos DamascoNoch keine Bewertungen
- Trends in Molecular Medicine - December 2013Dokument51 SeitenTrends in Molecular Medicine - December 2013Kevin SavouryNoch keine Bewertungen
- SCIENTISTSDokument5 SeitenSCIENTISTSMarica Mae PreNoch keine Bewertungen
- MedChem5 Lead PDFDokument61 SeitenMedChem5 Lead PDFsastraNoch keine Bewertungen
- KPC Mouse ModelDokument16 SeitenKPC Mouse Modeljoe smoNoch keine Bewertungen
- Humanized Mice For The Study of Immuno-Oncology: ReviewDokument16 SeitenHumanized Mice For The Study of Immuno-Oncology: ReviewMaria Camila MejíaNoch keine Bewertungen
- MCQ Immunology BasicDokument71 SeitenMCQ Immunology BasicMatthew HallNoch keine Bewertungen
- MRCP NotesDokument33 SeitenMRCP NotesHemant DanielNoch keine Bewertungen