Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Fascial Stretch TherapyDokument294 SeitenFascial Stretch TherapyDiana Mariș93% (28)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- For Bulletproof Shoulders: 5 Key ElementsDokument8 SeitenFor Bulletproof Shoulders: 5 Key ElementsMarcAnthonyNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Ayurvedic Massage Therapy - Therapeutic Massage Techniques Based On The Ancient Healing Science of AyurvedaDokument197 SeitenAyurvedic Massage Therapy - Therapeutic Massage Techniques Based On The Ancient Healing Science of AyurvedaCesarMello100% (3)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- P90X/P90X2 Hybrid Workout SchedulesDokument3 SeitenP90X/P90X2 Hybrid Workout SchedulesDragouilleNoch keine Bewertungen
- Warm Up Before YogaDokument9 SeitenWarm Up Before YogaShyam_Nair_9667Noch keine Bewertungen
- Reverse Total Shoulder Replacement-Orthoinfo - AaosDokument5 SeitenReverse Total Shoulder Replacement-Orthoinfo - Aaosapi-228773845Noch keine Bewertungen
- AACP Acupuncture Point Reference Manual PDFDokument100 SeitenAACP Acupuncture Point Reference Manual PDFRadhakrishnan Kasthuri100% (4)
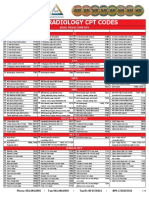
- 2019 Radiology CPT Codes: CT Bone DensitometryDokument2 Seiten2019 Radiology CPT Codes: CT Bone DensitometryDownsyndrome CyborgNoch keine Bewertungen
- Musculoskeletal UltrasonographyDokument33 SeitenMusculoskeletal UltrasonographyAdityaNoch keine Bewertungen
- TOSSM-APKASS 2020 - Conference ProgramDokument3 SeitenTOSSM-APKASS 2020 - Conference Programfajar alatasNoch keine Bewertungen
- UihiuDokument44 SeitenUihiuValentina Alejandra Barros WernerNoch keine Bewertungen
- YogaasanDokument6 SeitenYogaasansmperumal1447Noch keine Bewertungen
- Effects of Scapular Stabilization Exercise Training OnDokument12 SeitenEffects of Scapular Stabilization Exercise Training OnNajoua SalomaoNoch keine Bewertungen
- Acta Orthopaedica Et Traumatologica TurcicaDokument5 SeitenActa Orthopaedica Et Traumatologica TurcicaAdosotoNoch keine Bewertungen
- AOS - Introduction To The Art of SymmetryDokument3 SeitenAOS - Introduction To The Art of SymmetryJeff An100% (1)
- (2022) - Effect of Manipulation Technique Using UltrasoundDokument8 Seiten(2022) - Effect of Manipulation Technique Using UltrasoundCristobal LopezNoch keine Bewertungen
- Frozen ShoulderDokument110 SeitenFrozen ShoulderAchmad ZulfikarNoch keine Bewertungen
- Rundown Acara 3rd National Sport Science Meeting - Sport ClinicDokument9 SeitenRundown Acara 3rd National Sport Science Meeting - Sport ClinicMika KresnaNoch keine Bewertungen
- 2009 Fee ScheduleDokument1.123 Seiten2009 Fee ScheduleNicole HillNoch keine Bewertungen
- Closed Fracture of Middle ClaviculaDokument12 SeitenClosed Fracture of Middle ClaviculachiciNoch keine Bewertungen
- Enfoque Inicial en ReumatologíaDokument33 SeitenEnfoque Inicial en ReumatologíaLuis Alberto Romero JaimesNoch keine Bewertungen
- PATHFIT 1 Training OverviewDokument77 SeitenPATHFIT 1 Training OverviewJasmine Rain H. LogroñoNoch keine Bewertungen
- Waitankung AsliDokument10 SeitenWaitankung AslisuryaNoch keine Bewertungen
- Relieve back and neck pain with self-massage techniquesDokument6 SeitenRelieve back and neck pain with self-massage techniqueskamal kant gargNoch keine Bewertungen
- Kinesiology Send-Ups Exam Paper 2017Dokument2 SeitenKinesiology Send-Ups Exam Paper 2017Chaman Lal Karotia67% (3)
- 13 Rotator Cuff Healing and The Bone Marrow Crimson Duvet From Clinical Observations To Science 1171446194Dokument8 Seiten13 Rotator Cuff Healing and The Bone Marrow Crimson Duvet From Clinical Observations To Science 1171446194César ArveláezNoch keine Bewertungen
- Biomechanics of The Shoulder ComplexDokument83 SeitenBiomechanics of The Shoulder Complexsundar prabhuNoch keine Bewertungen
- Surgical Techniques for Repairing Canine Scapula FracturesDokument12 SeitenSurgical Techniques for Repairing Canine Scapula FracturesasheneyNoch keine Bewertungen
- Shoulder Impingement Exercise Guidelines PDFDokument3 SeitenShoulder Impingement Exercise Guidelines PDFMichele MarengoNoch keine Bewertungen
- The Front Squat and Its Variations: Keywords: Depth Force Flexibility Strength Thoracic KyphosisDokument7 SeitenThe Front Squat and Its Variations: Keywords: Depth Force Flexibility Strength Thoracic KyphosisRosaneLacerdaNoch keine Bewertungen